利妥昔單抗聯合甲氨蝶呤在中重度類風濕關節炎中的臨床應用
2016-06-22 06:26:32李威
實用藥物與臨床 2016年5期
關鍵詞:類風濕性關節炎
李 威
·短篇論著·
利妥昔單抗聯合甲氨蝶呤在中重度類風濕關節炎中的臨床應用
李威
本溪市中心醫院急診科,遼寧 本溪 117000
[摘要]目的評價利妥昔單抗(RTX)及甲氨蝶呤(MTX)在中重度類風濕性關節炎中聯合應用的臨床效果。方法將68例中重度類風濕性關節炎患者隨機分為試驗組及對照組,每組34例,分別給予RTX+MTX及安慰劑+MTX治療,觀察兩組間類風濕性關節炎的臨床及化驗指標變化。結果治療后1個月,試驗組觸痛關節數、晨僵時間、Barthel指數與對照組比較,差異有統計學意義(P<0.05)。治療后3個月,試驗組的腫脹關節數、觸痛關節數、晨僵時間、DAS28評分及Barthel指數與對照組比較,差異有統計學意義(P<0.05或P<0.01)。治療后1個月,試驗組CRP、ESR、RF、IL-6低于對照組(P<0.05或P<0.01);治療后3個月,試驗組CRP、ESR、RF、IL-6低于對照組(P<0.01)。隨訪期內,試驗組的并發癥、過敏反應發生率高于對照組(P<0.05)。結論MTX聯合應用RTX治療中重度類風濕性關節炎可達到安全滿意的臨床效果。
[關鍵詞]類風濕性關節炎;利妥昔單抗;甲氨蝶呤
0引言
類風濕性關節炎是一種免疫性疾病,具有病情遷延、病程長及致殘率高的特點[1]。患者由于長期反復的病情發作導致關節功能受損,生活質量降低,甚至由長期發展導致抑郁傾向[2]。類風濕關節炎治療的藥物主要包括激素、非甾體抗炎藥及慢作用抗風濕藥物(Disease modifying anti-rheumatic drugs,DMARDs)[3]。利妥普單抗(Rituximab,RTX)2006被美國FDA批準應用治療中重度類風濕性關節炎。甲氨蝶呤(Methotrexate,MTX)是葉酸拮抗劑,是DMARD中常用的一種藥物,屬抗代謝類藥物。本研究應用甲氨蝶呤聯合利妥昔單抗(RTX)治療類風濕性關節炎,評估其效果及臨床反應,探討其臨床應用價值。
1資料與方法
1.1研究對象以2013年2月至2014年11月在我院風濕免疫科住院治療的68例類風濕關節炎患者為研究對象,男31例,女37例,年齡(53.7±21.9)歲,病程(73.62±47.19)個月。以ACR(American College of Rheumatology,美國風濕病學會)2010年修訂的類風濕診斷標準進行診斷。滿足下列活動條件:腫脹關節數≥4個,觸痛關節數≥4個,紅細胞沉降率(ESR)>28 mm/h,血清C反應蛋白(CRP)>5 mg/L,病情活動度為中重度,類風濕活動指數DAS28≥3.2,采用Barthel指數進行患者的日常生活質量評分。計算機隨機數法隨機分為對照組及試驗組,每組34例。RTX注射液(美羅華)購自上海羅氏制藥有限公司,MTX片購自通化茂祥制藥有限公司。排除標準:伴有心、腦、肺、肝、腎等重要器官疾病或功能不全;有上消化道潰瘍病史者;有炎性關節病或伴有其他結締組織病者;嚴重感染、結核、HIV感染、活動肝炎、腫瘤、血液病患者,曾經接受過單克隆抗體治療的患者;白細胞計數<4×109/L,血紅蛋白<85 g/L,血小板計數<100×109/L;妊娠期、2年內計劃生育女性及哺乳期女性;用藥依從性差者。在應用RTX前,兩組患者的年齡、性別、病程、關節功能分級、腫脹關節數、觸痛關節數、晨僵時間、DAS28評分、Barthel指數、ESR、CRP、RF、IL-6等比較差異均無統計學意義(P>0.05),可進行病例對照研究,無倫理學爭議。
1.2研究方法所有納入研究病例治療前均使用過1種或幾種改善病情抗風濕藥(激素、非甾體抗炎藥或DMARDs)且效果不滿意。1個月內停用激素、非甾體抗炎藥及DMARDs。試驗組:MTX 10 mg/周,口服,維持穩定劑量6周,RTX 1 000 mg加入500 mL生理鹽水靜脈滴注給藥2次,兩次間隔15 d。對照組:給予MTX 10 mg/周口服,維持穩定劑量6周,安慰劑(生理鹽水500 mL)靜脈滴注給藥2次,兩次間隔15 d。

2結果
2.1兩組臨床資料比較隨訪至治療后3個月,兩組患者治療后腫脹關節數少于對照組,觸痛關節數、晨僵時間較短,DAS28評分及Barthel指數均有改善,在治療后1個月,試驗組的觸痛關節數目少于對照組,晨僵時間較對照組縮短,差異有統計學意義(P<0.05),Barthel指數高于對照組(P<0.05)。治療后3個月,試驗組的腫脹關節數、觸痛關節數、晨僵時間及DAS28評分低于對照組,差異有統計學意義(P<0.05或P<0.01),Barthel指數高于對照組(P<0.01)。見表1。
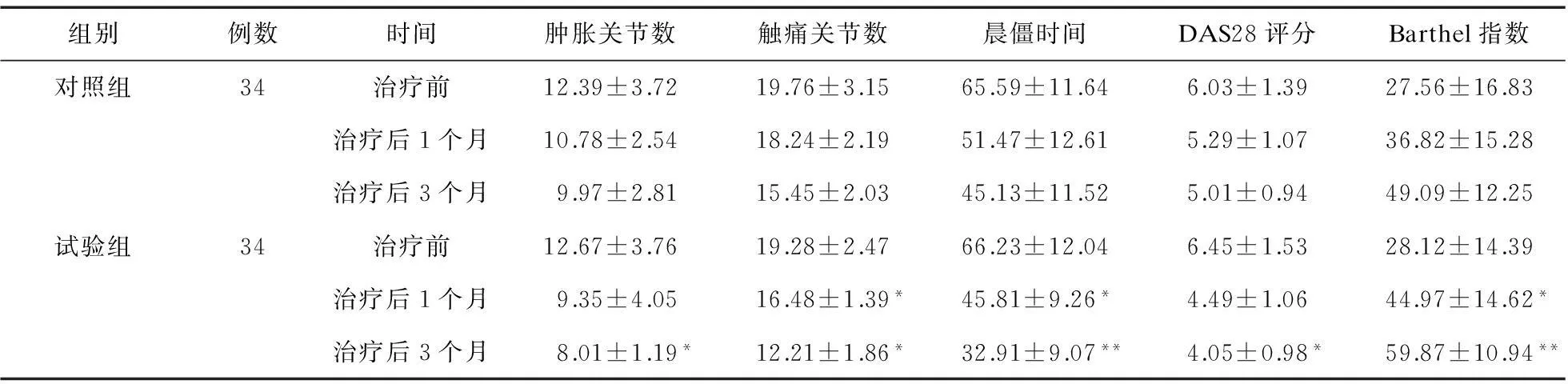
表1 兩組臨床指標比較
注:與對照組比較,*P<0.05,**P<0.01
2.2兩組化驗指標比較隨訪至治療后3個月,兩組CRP、ESR、RF、IL-6均改善。治療后1個月,試驗組CRP、ESR、RF、IL-6低于對照組(P<0.05或P<0.01);治療后3個月,兩組比較差異有統計學意義(P<0.01),見表2。

表2 兩組化驗指標比較
注:與對照組比較,*P<0.05,**P<0.01
2.3兩組藥物不良反應比較隨訪期間,兩組患者均無肝壞死、心肌毒性及過敏休克等嚴重不良反應事件發生,兩組胃腸道反應、血糖異常、神經癥狀、肝功能變化、白細胞減少、黏膜潰瘍及感染等并發癥比較差異無統計學意義(P>0.05),試驗組過敏反應率高于對照組(P<0.05)。見表3。

表3 患者藥物不良反應發生情況(例,%)
注:與對照組比較,*P<0.05
3討論
類風濕性關節炎病情遷延,患者痛苦,生活質量下降[4]。藥物治療無論是激素、非甾體抗炎藥還是DARMDs均需要長期應用,不良反應較大,對于一部分中重度患者治療效果并不滿意[5]。MTX是DMARDs中的一種,屬于抗代謝類藥,能通過抑制二氫葉酸還原酶及甲酰基轉移酶生物活性,從而抑制IL、TNF等細胞因子釋放,發揮抗炎效果,減輕關節腫脹及疼痛[7]。RTX用于治療中重度類風濕性關節炎患者,與DMARDs類藥物聯合使用,或應用于1種及多種抗TNF-α抗體效果不顯著時[8]。RTX是嵌合鼠/人單克隆抗體,該抗體可與B淋巴細胞膜上的CD20結合,引發B細胞進入溶解免疫反應,細胞溶解機制包括抗體依賴性細胞毒性和補體依賴性細胞毒性[9]。有研究認為,RTX可用于MTX聯合其他的抗風濕藥或其他非生物抗風濕藥物治療效果不滿意的類風濕性關節炎病例[10]。本研究聯合應用RTX及MTX治療中重度類風濕性關節炎,結果顯示,隨訪至治療后3個月,兩組治療后腫脹關節數目、觸痛關節數目、晨僵時間、DAS28評分及Barthel指數均有改善,且CRP、ESR、RF、IL-6均得到改善,但RTX組的臨床指標及化驗指標改善更為明顯,Van Vollenhoven等[11]研究顯示,其臨床癥狀、體征及化驗指標在應用RTX 8~16周明顯改善。本研究顯示,用藥4周后癥狀開始出現改善,3個月后明顯改善。Genovese等[12]研究顯示,RTX聯合MTX達到ACR50緩解的比例達51%,RTX組在ACR緩解指標上有明顯優勢,在影像學表現、關節功能改善、生活質量提高等方面都有良好的效果。而且,RTX單獨應用也可達到臨床緩解的目的。MTX的不良反應包括惡心、嘔吐、飽脹及腹瀉等消化道癥狀,血糖異常,肝腎功能損傷,致畸及精神癥狀等[13],RTX不良反應除了消化道癥狀、肝腎毒性外,變態反應的發生率也較高[14]。本研究結果顯示,在藥物不良反應方面,RTX增加了患者過敏反應的發生幾率。RTX可能并發難以控制的感染,但本研究納入患者中沒有出現嚴重感染病例,所發生感染病例為泌尿系感染及癤腫等,經抗炎治療均治愈。
本研究通過聯合應用MTX及RTX對中重度類風濕性關節炎進行治療,結果顯示,聯合應用RTX可明顯改善患者臨床癥狀,對常規抗風濕治療效果不明顯的患者,可以考慮給予RTX治療。
參考文獻:
[1]Gashi AA,Rexhepi S,Berisha I,et al.Treatment of rheumatoid arthritis with biologic DMARDS (Rituximab and Etanercept) [J].Med Arch,2014,68(1):51-53.
[2]Roshique KK,Ravindran V.Efficacy and safety of a biosimilar rituximab in biologic na?ve patients with active rheumatoid arthritis[J].Clin Rheumatol,2015,34(7):1289-1292.
[3]Harrold LR,Reed GW,Shewade A,et al.Effectiveness of rituximab for the treatment of rheumatoid arthritis in patients with prior exposure to anti-TNF:results from the CORRONA registry[J].J Rheumatol,2015,42(7):1090-1098.
[4]Reddy V,Cambridge G,Isenberg DA,et al.Internalization of rituximab and the efficiency of B cell depletion in rheumatoid arthritis and systemic lupus erythematosus[J].Arthritis Rheumatol,2015,67(8):2046-2055.
[5]Wu B,Song Y,Leng L,et al.Treatment of moderate rheumatoid arthritis with different strategies in a health resource-limited setting:a cost-effectiveness analysis in the era of biosimilars[J].Clin Exp Rheumatol,2015,33(1):20-26.
[6]Yamada K,Oshiro Y,Okamura S,et al.Clinicopathological characteristics and rituximab addition to cytotoxic therapies in patients with rheumatoid arthritis and methotrexate-associated large B lymphoproliferative disorders[J].Histopathology,2015,67(1):70-80.
[7]Bazzichi L,Biasi D,Tinazzi E,et al.Safety of rituximab in the routine treatment of rheumatoid arthritis in Italy in patients refractory to anti-TNFa drugs:results from the observational retrospective-prospective RUBINO study[J].Reumatismo,2014,66(3):224-232.
[8]Valleala H,Korpela M,Hienonen-Kempas T,et al.Long-term real-life experience with rituximab in adult finnish patients with rheumatoid arthritis refractory or with contraindication to anti-tumor necrosis factor drugs[J].J Clin Rheumatol,2015,21(1):24-30.
[9]Gamonet C,Deschamps M,Marion S,et al.The alternative CD20 transcript variant is not a surrogate marker for resistance to rituximab in patients with rheumatoid arthritis[J].Rheumatology (Oxford),2015,54(9):1744-1745.
[10]Schattner A.ACP Journal Club.Review:In rheumatoid arthritis,adding rituximab to methotrexate improves clinical outcomes[J].Ann Intern Med,2015,162(12):JC9.
[11]Van Vollenhoven RF,Emery P,Bingham CO,et al.Long-term safety of rituximab in rheumatoid arthritis:9.5-year follow-up of the global clinical trial programme with a focus on adverse events of interest in RA patients[J].Ann Rheum Dis,2013,72(9):1496-1502.

[13]Kudo-Tanaka E,Shimizu T,Nii T,et al.Early therapeutic intervention with methotrexate prevents the development of rheumatoid arthritis in patients with recent-onset undifferentiated arthritis:A prospective cohort study[J].Mod Rheumatol,2015,30(4):1-6.
[14]Isvy A,Meunier M,Gobeaux-Chenevier C,et al.Safety of rituximab in rheumatoid arthritis:a long-term prospective single-center study of gammaglobulin concentrations and infections[J].Joint Bone Spine,2012,79(4):365-369.
Clinical application of rituximab combined with methotrexate in the treatment of rheumatoid arthritis
LI Wei
(Emergency Department,Benxi Central Hospital,Benxi 117000,China)
[Abstract]ObjectiveTo evaluate the clinical efficacy of rituximab combined with methotrexate in the treatment of rheumatoid arthritis.MethodsSixty-eight patients diagnosed with moderate or severe rheumatoid arthritis were divided into experiment group (n=34) and control group (n=34) who accepted RTX+MTX and placebo+MTX respectively.The clinical and laboratory indexes were observed.ResultsCompared with control group,the number of tender joint and time of morning stiffness in experiment group were lower at 1 month after treatment (P<0.05),and the Barthel index was higher (P<0.05).The number of swollen joint and tender joint,the time of morning stiffness and DAS28 score in experiment group were lower than those of control group at 3 months after treatment (P<0.05 or P<0.01) with higher Barthel index (P<0.05).The levels of CRP (C-reactive protein),ESR (erythrocyte sedimentation),RF (rheumatoid factor) and IL-6 (Interleukin 6) in experiment group were lower than those of control group at 1 month (P<0.05 or P<0.01) and 3 months (P<0.01) after treatment.The allergic rate in experiment group was higher than that of control group during follow-up period (P<0.05).ConclusionRituximab combined with methotrexate is effective and safe with satisfactory result in the treatment of rheumatoid arthritis.
Key words:Rheumatoid arthritis;Rituximab;Methotrexate
收稿日期:2015-09-09
DOI:10.14053/j.cnki.ppcr.201605032
猜你喜歡
醫學信息(2017年1期)2017-02-28 00:21:02
中國民族民間醫藥·上半月(2016年12期)2017-01-11 14:57:56
現代養生·下半月(2016年5期)2017-01-09 09:45:45
中國實用醫藥(2016年24期)2016-10-17 05:36:05
中國實用醫藥(2016年17期)2016-07-26 23:07:39
飲食與健康·下旬刊(2016年7期)2016-05-10 12:39:40
中國實用醫藥(2016年11期)2016-05-04 13:45:25
中國當代醫藥(2015年4期)2015-08-03 17:51:25
中國現代醫生(2015年8期)2015-04-17 10:52:15
