經臍單孔腹腔鏡下子宮肌瘤剔除術治療子宮肌瘤的臨床效果
2020-11-06 07:22:10肖娟羅建秀魏荷花
中國當代醫藥 2020年26期
關鍵詞:并發癥
肖娟 羅建秀 魏荷花


[摘要]目的 探討經臍單孔腹腔鏡下子宮肌瘤剔除術治療子宮肌瘤的臨床效果。方法 選取2018年2月~2019年3月在我院就診的子宮肌瘤患者80例作為研究對象,采用隨機數字表法將其分為對照組與觀察組,每組各40例。對照組采用多孔腹腔鏡子宮肌瘤剔除術治療,觀察組采用經臍單孔腹腔鏡子宮肌瘤剔除術治療,比較兩組患者的臨床指標、術后隨訪情況、疼痛程度、滿意度、并發癥、盆腹腔種植情況。結果 觀察組患者手術時間長于對照組,術中出血量少于對照組,肛門排氣時間短于對照組,差異有統計學意義(P<0.05);兩組患者住院時間比較,差異無統計學意義(P>0.05);術后隨訪6個月,兩組患者的月經正常率比較,差異無統計學意義(P>0.05);觀察組患者肌瘤復發率低于對照組,差異有統計學意義(P<0.05);觀察組疼痛視覺模擬量表(VAS)評分、體象量表(BIS)評分低于對照組,切口美觀滿意度(CS)評分高于對照組,差異有統計學意義(P<0.05);兩組術后并發癥總發生率及盆腹腔種植率比較,差異無統計學意義(P>0.05)。結論 子宮肌瘤患者采用經臍單孔腹腔鏡子宮肌瘤剔除術治療的效果顯著,可有效降低患者的術后疼痛程度,減少肌瘤或肉瘤腹腔種植的可能,術后切口美觀,且不會增加并發癥的發生。
[關鍵詞]子宮肌瘤;單孔腹腔鏡;腹腔鏡下子宮肌瘤剔除術;疼痛程度;切口美觀;盆腹腔種植;并發癥
[中圖分類號] R737.33? ? ? ? ? [文獻標識碼] A? ? ? ? ? [文章編號] 1674-4721(2020)9(b)-0111-04
Clinical effect of transumbilical single port laparoscopic myomectomy for the treatment of uterine fibroids
XIAO Juan? ?LUO Jian-xiu? ?WEI He-hua
Department of Gynecology, Ganzhou People′s Hospital, Jiangxi Province, Ganzhou? ?341000, China
[Abstract] Objective To explore the clinical effect of transumbilical single port laparoscopic myomectomy for the treatment of uterine fibroids. Methods A total of 80 patients with uterine fibroids who were treated in our hospital from February 2018 to March 2019 were selected as the research objects. They were divided into control group and observation group by a random number table method, with 40 cases in each group. The control group was treated with porous laparoscopic myomectomy, and the observation group was treated with transumbilical single-port laparoscopic myomectomy. The clinical indicators, postoperative follow-up, pain degree, satisfaction, complications, and pelvic-abdominal implantation were compared between the two groups. Results The operation time in the observation group was longer than that in the control group, the amount of intraoperative blood loss was less than that in the control group, and the anal exhaust time was shorter than that in the control group, the differences were statistically significant (P<0.05). There was no statistical difference in the length of hospitalization time between the two groups (P>0.05). After 6 months of follow-up, there was no significant difference in normal menstrual rate between the two groups (P>0.05); the recurrence rate of fibroids in the observation group was lower than that in the control group, and the difference was statistically significant (P<0.05); the pain visual analogue scale (VAS) score and the body image scale (BIS) score in the observation group were lower than those in the control group, the cosmetic score (CS) was higher than that in the control group, the differences were statistically significant (P<0.05). There were no significant differences in the total incidence of postoperative complications and the rate of pelvic-abdominal implantation between the two groups (P>0.05). Conclusion The effect of transumbilical single port laparoscopic myomectomy for patients with uterine fibroids is significant, which can effectively reduce the postoperative pain and reduce the possibility of intraperitoneal implantation of fibroids or sarcomas, and the postoperative incision is beautiful and does not increase complications occur.
[Key words] Uterine fibroids; Single port laparoscopy; Laparoscopic myomectomy; Pain degree; Beautiful incision; Pelvic-abdominal implantation; Complications
子宮肌瘤是常見的生殖器官良性腫瘤,多發生于孕齡期女性,臨床主要表現為腹痛及月經紊亂,對患者的日常生活造成較大的影響,甚至會導致患者不孕[1]。臨床治療子宮肌瘤多以手術為主,但傳統開腹手術創傷較大、并發癥較多,對患者術后恢復極為不利[2]。隨著微創技術的發展,可進行損傷小、恢復快的手術,還能保留患者的生育功能,已成為臨床治療的首選[3]。微創手術中單孔腹腔鏡下子宮肌瘤剔除術與多孔腹腔鏡子宮肌瘤剔除術具有代表性。但隨著人們生活水平的提高,子宮肌瘤患者不僅要求保留子宮,而且要求美觀、微創、疼痛較輕的手術[4-5]。基于此,本研究旨在探討經臍單孔腹腔鏡子宮肌瘤剔除術對子宮肌瘤患者疼痛程度及并發癥的影響,現報道如下。
1資料與方法
1.1一般資料
選取2018年2月~2019年3月在我院就診的80例子宮肌瘤患者作為研究對象,采用隨機數字表法將其分為對照組與觀察組,每組各40例。對照組中,年齡22~58歲,平均(38.23±4.48)歲;病程6個月~8年,平均(4.47±0.32)年;疾病類型:漿膜下肌瘤8例,闊韌帶肌瘤9例,肌壁間肌瘤12例,宮頸肌瘤11例。觀察組中,年齡23~57歲,平均(38.46±4.74)歲;病程6個月~7年,平均(4.34±0.38)年;疾病類型:漿膜下肌瘤10例,闊韌帶肌瘤7例,肌壁間肌瘤11例,宮頸肌瘤12例。兩組患者一般資料比較,差異無統計學意義(P>0.05),具有可比性。本研究經我院醫學倫理委員會批準,患者均已簽署知情同意書。
1.2納入及排除標準
納入標準:①患者均符合相關診斷標準,確診為子宮肌瘤[5];②雙側卵巢無異常者。排除標準:①伴有心肺疾病者;②下腹部有手術瘢痕者;③伴有惡性腫瘤者;④合并精神疾病患者;⑤妊娠、期哺乳期婦女;⑥有手術禁忌證者;⑦存在腫瘤標志物指標異常者。
1.3方法
對照組患者行多孔腹腔鏡子宮肌瘤剔除術,氣管插管全身麻醉,取膀胱截石頭低臀高位,在患者臍部及左右麥氏點進行Trocar穿刺,經陰道放置舉宮器,建立氣腹,并維持氣壓在14 mmHg,腹腔鏡觀察患者腹腔及子宮肌瘤情況,觀察子宮肌瘤數量、位置及與盆腔粘連狀態;注入縮宮素10 U,在肌瘤漿膜面采用單極電凝切開子宮肌層深達瘤體組織,鈍性分離肌瘤假包膜并剔除;電凝止血后,縫合漿肌層,關閉瘤腔,單極電凝將漿膜下肌瘤蒂部凝斷、剔除,將腹部切口延長至1.5~2.0 cm,放置肌瘤轉,粉碎肌瘤后取出。
觀察組采用經臍單孔腹腔鏡子宮肌瘤剔除術治療,全身麻醉,取膀胱截石位,對臍部穿刺,建立氣腹,維持壓力在14~15 mmHg,置入Port探查盆腔、子宮及雙側附件,對手術難度作出評價,觀察子宮肌瘤數量、位置及與盆腔粘連狀態;注入縮宮素10 U,在肌瘤漿膜面采用單極電凝切開子宮肌層深達瘤體組織,鈍性分離肌瘤假包膜并剔除;電凝止血后,縫合漿肌層,關閉瘤腔,單極電凝將漿膜下肌瘤蒂部凝斷、剔除。放入一標本袋,將肌瘤裝好后自臍部切口拉出,使用大刀將肌瘤小塊切開后取出。腹腔鏡確認子宮創面,電凝止血后,沖洗盆腔。
1.4觀察指標及評價指標
①比較兩組患者的臨床指標,包括手術時間、住院時間、術中出血量、肛門排氣時間。②術后隨訪6個月比較兩組患者肌瘤復發及月經恢復正常情況。③比較兩組術后24 h疼痛程度及身體、切口美觀滿意度,其中疼痛程度采用視覺模擬量表(VAS)[6],分值范圍為0~10分,分數越高疼痛越劇烈;身體、切口美觀滿意度分別采用體像自評問卷(BIQ)[7]調查,包括體象量表(BIS)評分及切口美觀滿意度(CS)評分,其中BIS分值范圍為0~30分,分數越高表明存在的問題越多;CS分值范圍為3~24分,分數越高患者的滿意程度越好。④術后隨訪6個月,比較兩組患者并發癥(感染、下肢靜脈栓塞、陰道出血)發生情況。⑤術后隨訪6個月,比較兩組患者術后盆腹腔種植情況。
1.5統計學方法
采用SPSS 18.0統計學軟件進行數據處理,計量資料用均數±標準差(x±s)表示,組間比較用獨立樣本t檢驗,組內比較用配對樣本t檢驗,計數資料采用率表示,組間比較采用χ2檢驗,以P<0.05為差異有統計學意義。
2結果
2.1兩組臨床指標的比較
觀察組患者手術時間長于對照組,術中出血量少于對照組,肛門排氣時間短于對照組,差異有統計學意義(P<0.05);兩組患者住院時間比較,差異無統計學意義(P>0.05)(表1)。
2.2兩組肌瘤復發、月經正常情況的比較
術后隨訪6個月,兩組患者月經正常率比較,差異無統計學意義(P>0.05);但觀察組患者的肌瘤復發率低于對照組,差異有統計學意義(P<0.05)(表2)。
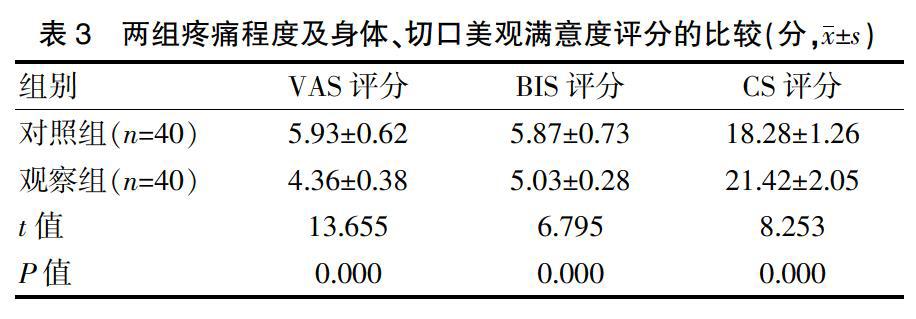
2.3兩組疼痛程度及身體、切口美觀滿意度評分的比較
觀察組患者的VAS評分和BIS評分低于對照組,CS評分高于對照組,差異有統計學意義(P<0.05)(表3)。
2.4兩組并發癥總發生率的比較
兩組患者的并發癥總發生率比較,差異無統計學意義(P>0.05)(表4)。
2.5兩組盆腹腔種植情況的比較
術后隨訪6個月,觀察組患者出現盆腔種植1例,盆腹腔種植率為2.50%(1/40);對照組患者出現盆腔種植2例,腹腔種植1例,盆腹腔種植率為7.50%(3/40)。兩組患者盆腹腔種植率比較,差異無統計學意義(χ2=0.263,P=0.608)。
猜你喜歡
今日健康(2016年12期)2016-11-17 13:30:12
今日健康(2016年12期)2016-11-17 13:13:23
今日健康(2016年12期)2016-11-17 12:59:44
中國現代醫生(2016年23期)2016-11-15 03:26:59
中國現代醫生(2016年23期)2016-11-15 03:17:26
中國現代醫生(2016年23期)2016-11-15 03:03:50
人間(2016年27期)2016-11-11 17:32:04
人人健康(2016年21期)2016-11-05 11:32:22
科技視界(2016年18期)2016-11-03 21:58:33
中國實用醫藥(2016年24期)2016-10-17 05:58:58
