阿司匹林聯(lián)合阿托伐他汀對心血管疾病患者心功能及生活質量的影響
2019-10-30 02:44:35邱淑花
中國當代醫(yī)藥 2019年24期
邱淑花
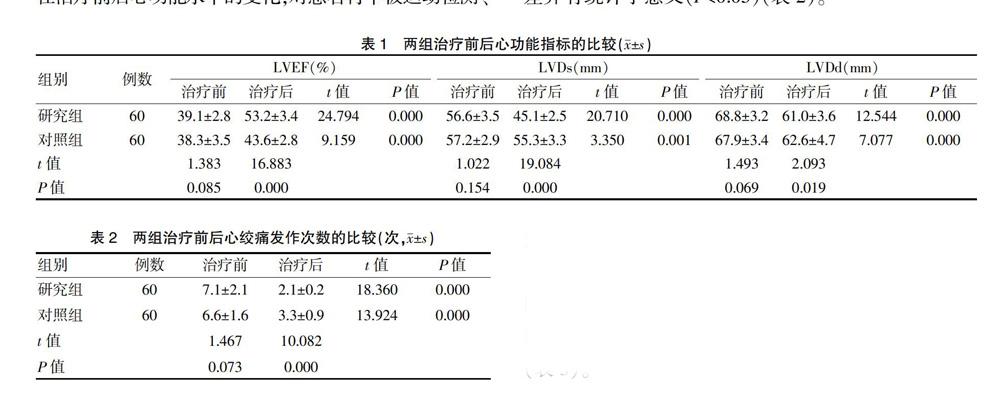
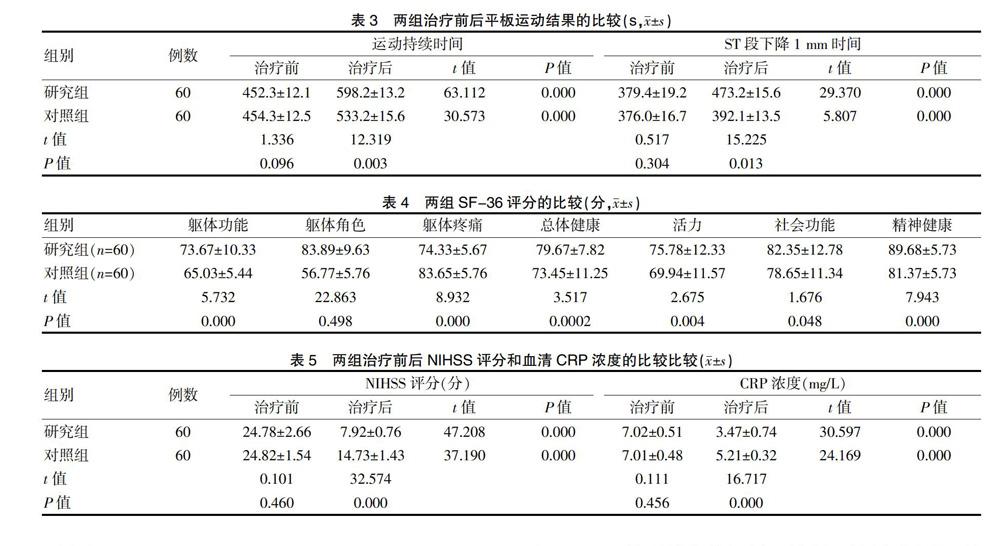
[摘要]目的 探討阿司匹林聯(lián)合阿托伐他汀對心血管疾病患者心功能及生活質量的影響。方法 選取2016年1~12月我院收治的120例心血管疾病患者作為研究對象,根據(jù)治療方法的不同將其分為研究組和對照組,每組各60例。研究組采用阿托伐他汀聯(lián)合阿司匹林治療,對照組僅采用阿司匹林治療,比較兩組的療效、心功能指標和生活質量評分。結果 研究組治療后的左心室射血分數(shù)(LVEF)高于對照組,左心室收縮末期內徑(LVDs)和左心室舒張末期內徑(LVDd)短于對照組,心絞痛發(fā)作次數(shù)少于對照組,運動持續(xù)時間和ST段下降1 mm時間長于對照組,軀體功能、精神健康、活力、社會功能和總體健康評分高于對照組,軀體疼痛程度更低,美國國立衛(wèi)生研究院卒中量表(NIHSS)評分和血清C-反應蛋白(CRP)水平低于對照組,差異均有統(tǒng)計學意義(P<0.05)。結論 采用阿司匹林聯(lián)合阿托伐他汀治療心血管患者,可對心功能和生活質量起到改善作用。
[關鍵詞]阿司匹林;阿托伐他汀;心功能;生活質量
[中圖分類號] R541.4? ? ? ? ? [文獻標識碼] A? ? ? ? ? [文章編號] 1674-4721(2019)8(c)-0095-04
[Abstract] Objective To investigate the effect of Aspirin combined with Atorvastatin on cardiac function and quality of life in patients with cardiovascular disease. Methods All 120 patients with cardiovascular disease in our hospital from January to December 2016 were selected as subjects, and these patients were divided into study group and control group depending on the treatmen method, 60 cases in each group. The study group was treated with Atorvastatin in combination with Aspirin, and the control group was treated with only Aspirin. The curative effect, cardiac function index and quality of life score of the two groups were compared. Results The left ventricular ejection fraction (LVEF) of the study group was higher than that of the control group, the left ventricular end-systolic diameter (LVDs) and left ventricular end-diastolic diameter (LVDd) were shorter than those of the control group, the number of angina attacks was fewer than that of the control group, the duration of exercise and the ST segment decreased by 1 mm were longer than those of the control group (P<0.05). In the study group, physical function, physical pain, mental health, vitality, social function and overall health scores were higher than those of the control group, national institute of health stroke scale (NIHSS) score and serum C-reactive protein(CRP) level were lower than those of the control group, the differences were statistically significant (P<0.05). Conclusion The use of Aspirin combined with Atorvastatin in the treatment of cardiovascular patients can improve the heart function and quality of life.
[Key words] Aspirin; Atorvastatin; Cardiac function; Quality of life
隨著我國人口老齡化的加深,心血管疾病的發(fā)病率不斷升高。根據(jù)我國流行病統(tǒng)計數(shù)據(jù),2017年中國有2.9億人患有心血管疾病,約為總人口的21%,2015年農村心血管疾病死亡率已達到298.4/100 000人,城鎮(zhèn)居民心血管死亡率為268.4/100 000人,心血管死亡率高于腫瘤,目前是我國死因最高的疾病[1]。患病人數(shù)排序如下:高血壓約2.7億人,腦卒中約1300萬人,冠心病約1100萬人,肺源性心臟病約500萬人,心力衰竭約450萬人,風濕性心臟病約250萬人,先天性心臟病約200萬人。同時心血管疾病可伴有心絞痛、呼吸困難等疾病,給患者的生活帶來很多不便,嚴重影響生活質量。因此在心血管疾病治療的過程中,要探索一種能改善患者心功能同時改善生活質量的治療方法。
阿司匹林在循證醫(yī)學的支持下用于預防和治療缺血性中風[4]。它可以抑制環(huán)加氧酶,具有抵抗血小板功能的作用,從而防止血小板黏附,活化,聚集和血栓形成。研究報道,口服阿司匹林可以在治療48 h內顯著降低缺血性中風的復發(fā)率[5]。阿司匹林的藥物代謝動力學特征。吸收:口服后阿司匹林迅速完全吸收。分布:以蛋白質結合形式廣泛分布于體內。代謝:它在肝臟中完全代謝。排泄物:排泄到尿液中[6]。
阿司匹林與阿托伐他汀聯(lián)合可能起到抗凝的協(xié)同作用。心血管疾病在中老年人中高發(fā),常引起殘疾或死亡。根據(jù)國際最新研究發(fā)現(xiàn),阿司匹林在腦梗死中可發(fā)揮作用[7]。動脈粥樣硬化斑塊是腦梗死的主要危險因素。患者的腦組織長時間處于缺氧和缺血狀態(tài),可以導致腦組織壞死并損害神經(jīng)功能從而導致預后不佳[8-9]。如要在短時間內改善腦組織預后,就要考慮如何改善腦組織缺氧和缺血。所以抗凝治療通常用于治療腦梗死。常用藥物包括腸溶阿司匹林和低分子肝素鈉[10-11]。腸溶阿司匹林可刺激血小板內環(huán)氧化酶的乙酰化,減少血栓素A2的合成,對溶栓酶誘導的血小板聚集起抑制作用,抑制血栓形成,促進血栓溶解[12]。低分子量肝素鈉是通過亞硝酸鹽的分解,濃縮和純化獲得的未分級肝素。阿托伐他汀是臨床抗氧化和氧自由基損傷的常用藥物[13]。它可減輕腦梗死患者腦組織的炎癥反應,降低腦水腫程度,保護局部腦組織。此外,阿托伐他汀還可抑制一氧化氮的神經(jīng)毒性[14]。阿托伐他汀鈣是一種輕質甲基戊二酸單體輔酶A還原酶抑制劑,可有效改善患者的HDL-C。它對由高膽固醇血癥和LDL-C引起的動脈粥樣硬化有良好的拮抗作用。并且它可降低血漿CRP的濃度,起到藥物的抗炎作用,也可在一定的過程中使用。腫瘤壞死因子-α,白介素-6和其他炎癥因子的程度降低[15]。阿托伐他汀鈣和抗凝藥物聯(lián)合治療腦梗死,能起到藥物協(xié)同作用,可進一步提高藥物對血小板聚集的抵抗力,調節(jié)血液黏稠度,防止血栓形成,從而有效提高藥物的作用治療,使得患者神經(jīng)功能損傷的恢復效果良好[16-17]。
有研究表明,單用阿司匹林治療難以實現(xiàn)有效治療,如果單獨使用阿司匹林治療缺血性卒中,超過一半的缺血性卒中患者會復發(fā),效果不理想[18]。這種結果可能與某些患者的阿司匹林依從性有關,環(huán)氧合酶基因多態(tài)性及影響阿司匹林的其他藥物的藥理作用等因素有關[19]。最近的研究發(fā)現(xiàn),他汀類藥物可以選擇性地抑制羥甲基戊二酰輔酶A還原酶,增加LDL-C受體,降低血清LDL-C水平,并抑制頸動脈粥樣硬化斑塊的形成[20]。同時,他汀類藥物還可減少頸動脈粥樣硬化斑塊形成過程中產(chǎn)生的各種炎癥介質,并在抑制炎癥反應和穩(wěn)定頸動脈粥樣硬化斑塊中發(fā)揮作用。本研究結果顯示,阿司匹林聯(lián)合阿托伐他汀對于心血管患者的心功能有明顯改善,同時能改善生活質量。
[參考文獻]
[1]中華醫(yī)學會心血管病學分會.慢性穩(wěn)定性心絞痛診斷與治療指南[J].中華心血管雜志,2007,35(3):195-206.
[2]袁小蓉,徐蘋,楊博.阿托伐他汀聯(lián)合曲美他嗪對冠心病患者Caspase-1和IL-18表達水平的影響[J].河北醫(yī)學,2017,23(2):134-145.
[3]鄒行斌,黃鶴.阿托伐他汀并曲美他嗪對冠心病患者血脂、炎性因子及心功能的療效[J].心血管康復醫(yī)學雜志,2016,25(3):276-280.
[4]冒益芳.曲美他嗪聯(lián)合阿托伐他汀治療冠心病的療效及對患者血脂和血液流變學的影響[J].中國基層醫(yī)藥,2014, 21(2):195-197 .
[5]Chiang KH,Cheng WL,Shih CM,et al.HMG-CoA reductase inhibitors,improve neovascula rization by increasing the expression density of CXCR4 in endothelial progenitor cells[J].PLoS One,2015,10(8):237-275.
[6]Montaner J,Bustamante A,Garcia-Matas S,et al.Combination of thrombolysis and statins in acute stroke is safe:results of the STARS randomized trial (stroke treatment with acute reperfusion and simvastatin)[J].Stroke,2016,47(17):2870-2873.
[7]Wenaweser P,Windecker S,Billinger M,et al.Effect of atorvastatin and pravastatin on platelet inhibition by aspirin and clopidogrel treatment in patients with coronary stent thrombosis[J].Am J Cardiol,2007,99(3):353-356.
[8]馬丕勇.曲美他嗪對老年慢性心力衰竭患者自主神經(jīng)功能的影響[J].中國全科醫(yī)學,2011,14(12):1290-1291,1295.
[9]Hong KS,Lee SH,Kim EG,et al.Recurrent ischemic lesions after acute atherothrombotic stroke: clopidogrel plus aspirin versus aspirin alone[J].Stroke,2016,47(9):2323-2330.
[10]中華醫(yī)學會心血管病學分會,中華心血管病雜志編輯委員會.中國心力衰竭診斷和治療指南2014[J].中華心血管病雜志,2014,42(2):98-122.
[11]Athyros VG,Papageorgiou AA,Mercouris BR,et al.Treatment with atorvastatin to the national cholesterol educational program goals versus usual care in secondary coronary heart disease prevention. The Greek atorvastatin and coronary-heart-disease evaluation(GREACE)study[J].Curr Med Res Opin,2002,18(4):220-228.
[12]Kurita H,Wakai S.Validity and reliability of the Bangla version of WHOQOL-BREF on an adolescent population in Bangladesh validity[J].Qual Life Res,2005,14(7):1783-1789.
[13]Gurwitz JH,Go AS,F(xiàn)ortmann SP.Tatins for primary prevention in older adults:uncertainty and the need for more evidence[J].JAMA,2016,316(19):1971-1972.
[14]Ridker PM,Lonn E,Paynter NP,et al.Primary prevention with statin therapy in the elderly:new meta-analyses from the contemporary JUPITER and HOPE-3 randomised trials[J].Circulation,2017,135(33):1979-1981.
[15]Collins R,Reith C,Emberson J,et al.Interpretation of the evidence for the efficacy and safety of statin therapy[J].Lancet,2016,389(10 059):2532-2561.
[16]Ofori-Asenso R,Jakhu A,Curtis AJ,et al.A systematic review and meta-analysis of the factors associated with non-adherence and discontinuation of statins among people aged ≥65 years[J].J Gerontol A Biol Sci Med Sci,2018,73(25):798-805.
[17]姚廣明,趙真真.抗凝藥物聯(lián)合阿托伐他汀鈣在腦梗死治療中的臨床價值分析[J].中國醫(yī)藥指南,2017,15(30):154-155.
[18]曾群娣,梁建尤,溫泉.缺血性腦卒中應用他汀類藥物聯(lián)合阿司匹林的治療與預防效果分析[J].黑龍江醫(yī)學,2017, 41(7):667-669.
[19]張斯時,張艷.環(huán)氧合酶-1和環(huán)氧合酶-2基因多態(tài)性與阿司匹林抵抗的相關性研究[J].中國臨床藥理學雜志,2015,31(17):1724-1726.
[20]譚志暉,郭瑞威,譚志勝,等.他汀類藥物在治療急性心肌梗死的臨床應用和研究進展[J].中國醫(yī)藥導報,2018, 15(20):27-30.
(收稿日期:2019-03-15? 本文編輯:崔建中)
猜你喜歡
護士進修雜志(2017年2期)2017-02-26 14:32:29
中外醫(yī)學研究(2016年28期)2016-11-28 07:03:50
今日健康(2016年12期)2016-11-17 13:43:42
今日健康(2016年12期)2016-11-17 13:31:00
今日健康(2016年12期)2016-11-17 12:06:09
今日健康(2016年12期)2016-11-17 11:46:28
中國現(xiàn)代醫(yī)生(2016年23期)2016-11-15 03:14:57
中國實用醫(yī)藥(2016年24期)2016-10-17 04:34:04
中國衛(wèi)生標準管理(2015年18期)2016-01-20 09:27:12
中國醫(yī)藥科學(2015年2期)2015-02-27 12:32:09