腹腔鏡與開腹全系膜切除術治療直腸癌臨床療效的Meta分析
2017-08-07 08:43:33葉家友李遠強馬松鶴陳愛軍
臨床外科雜志 2017年2期
葉家友 李遠強 馬松鶴 陳愛軍
·論著·
腹腔鏡與開腹全系膜切除術治療直腸癌臨床療效的Meta分析
葉家友 李遠強 馬松鶴 陳愛軍
目的 比較腹腔鏡與開腹全直腸系膜切除術治療直腸癌的臨床療效。方法 計算機檢索PubMed、EMBASE、Cochrane Library、CNKI、萬方、維普等數據庫2010年9月1日至2015年9月1日期間公開發表的腹腔鏡與開腹全直腸系膜切除術的隨機對照研究,2位評價者按納入排除標準獨立完成文獻篩選,交叉審核,提取相關結局指標數據,應用RenMan 5.1軟件進行Meta分析。結果 最終納入10篇對照研究,總病例數2820例,腹腔鏡全直腸系膜切除術(laparoscopic total mesorectal excision,LTME)組1595例,開腹全直腸系膜切除術(open total mesorectal excision,OTME)組1225例。圍手術期相關指標:LTME組手術時間較OTME組長30.34 ml,LTME組術中出血量較OTME組少78.26 ml,LTME組術后肛門首次通氣時間平均短1.13天,LTME組術后平均住院時間平均短2.60天,同時LTME組術后切口感染發生率更低。而LTME組與OTME組淋巴結清掃數,環切緣陽性例數,吻合口瘺、腸梗阻發生率比較,差異均無統計學意義。預后相關研究指標:LTME組與OTME組3年局部復發、3年總生存率、3年無病生存率(DFS)、5年OS、5年DFS比較,差異均無統計學意義。結論 LTME治療直腸癌短期療效優勢明顯,術中出血少,肛門通氣時間早,術后平均住院時間短,切口感染發生率低。二者遠期療效比較LTME組不亞于OTME組。
直腸癌; 腹腔鏡; 開腹手術; 療效; Meta分析
直腸癌腹腔鏡全系膜切除術(laparoscopic total mesorectal excision,LTME)相比于開腹全系膜切除術(open total mesorectal excision,OTME),具有手術視野充分、術中出血少、術后恢復時間快等優點。但直到2015年美國國家癌癥綜合網絡(NCCN)結直腸治療指南仍未推薦腹腔鏡手術作為結直腸腫瘤外科治療的可行術式[1]。主要考慮目前對于二者手術療效及安全性的研究,由于大多數樣本量較小,方法學質量較低,觀察的結局指標不一致,結論尚存在爭議。本研究以公開發表的LTME與OTME治療直腸癌的臨床療效及安全性行Meta分析。
材料與方法
1.檢索策略:英文檢索詞“laparoscopic”、“ open surgery”、“ outcomes”、“ rectal cancer”、“rectum carcinoma”、“rectum tumour”限定于摘要在PubMed、EMBASE、Cochrane Library等英文數據庫中檢索;中文檢索詞“腹腔鏡”、“開腹手術”、“全直腸系膜切除”、“直腸癌”、“療效”限定于摘要在CNKI、萬方、維普等數據庫檢索。時間限定于2010年9月1日至2015年9月1日。語言是英文或中文的公開發表文獻。
2.納入標準:(1)研究對象為術前經活組織病理檢查確診為直腸癌的患者;(2)術前經結腸鏡、CT、MRI等輔助檢查評估可行全系膜切除;(3)干預措施為腹腔鏡手術(實驗組)與傳統開放手術(對照組)比較的隨機對照研究(RTCs)或非隨機對照研究(non-RTCs);(4)術前實驗組及對照組患者均未出現腸梗阻、腸穿孔等急診癥狀而需急診手術者;(5)總研究病例數≥50例;(6)至少有一項主要結局指標可提取。
3.排除標準:(1)綜述或僅有摘要的文獻;(2)結腸癌、直腸癌混合研究的文獻;(3)術前病理檢查疑似直腸癌,術后確診為其他病變者;(4)研究文獻重復發表;(5)全文經與作者聯系、文獻傳遞等方式確實不可獲得或是文獻數據不可提取;(6)不符合以上納入標準。
4.納入研究質量評價:隨機對照研究采用改良Jadad評分[2],評價指標包括:隨機序列的產生、盲法、分配隱藏、數據缺失等,滿分7分,>3分認為高質量文獻;非隨機對照研究采用NOS量表評分[3],評價指標包括:病例的定義、病例的代表性、對照的選擇、對照的定義、病例與對照的可比性、暴露的確定、暴露的方法及無應答率等,>6分認為高質量文獻。質量評估由2名研究者獨立進行并交叉核對,如遇意見不統一,則請第3名研究者協助解決。
5.數據提取:(1)納入文獻基本資料:作者、發表年份、病例數、年齡、TNM分期、結局指標;(2)圍手術期相關指標:手術時間(min)、術中出血量(ml)、肛門通氣時間(天)、術后平均住院時間(天)、淋巴結清掃數(個)、環切緣(circumferential resection margin,CRM)陽性、吻合口瘺、腸梗阻、切口感染;(3)預后相關指標:隨訪3年局部復發、3年總生存率(OS)、3年無病生存率(DFS)、5年OS、5年DFS。以上數據由2名研究者獨立進行并交叉核對,如遇意見不統一,則請第3名研究者協助解決。
6.統計分析:應用RenMan 5.1軟件進行Meta分析。二分類資料采用相對危險度(rate ratio,RR)分析統計,連續性資料采取均數差( mean difference,MD)分析統計,使用風險比(hazard ratio,HR)對OS、DFS進行分析[4]。HR由原文直接提取或從Kaplan-Meier曲線中計算獲得[5]。顯著性水準設為α=0.05,取95%可信區間(confidenceinterval,95%CI)。采用I2對異質性進行定量分析,若I2>50%,P≤0.1,則認為存在統計學異質性。在各實驗組之間無臨床異質性的前提下,存在統計學異質性時,采用隨機效應模型,反之采取固定效應模型。若存在臨床異質性,則放棄合并分析。P<0.05為差異有統計學意義。潛在的發表偏倚用倒漏斗圖分析。
結 果
一、檢索流程及納入文獻基本特征
嚴格按照檢索策略共檢索出中英文文獻804篇,遵循納入排除標準,閱讀題目、摘要、全文,去除重復發表等篩選,最終納入10篇文獻,共2 820例研究對象。提取每個納入研究的基本資料見表1。
二、結果
1.圍手術期相關研究指標:本研究共提取手術時間(min)、術中出血量(ml)、肛門通氣時間(天)、術后平均住院時間(天)、淋巴結清掃數(個)、CRM陽性(例)、吻合口瘺(例)、腸梗阻(例)、切口感染(例)9項圍手術期指標,比較LTME與OTME。Meta分析結果顯示:LTME組手術時間比OTME組平均長30.34 min(P<0.01,95%CI:21.61~39.07);LTME組術中出血量平均少78.26 ml(P<0.01,95%CI:-116.20~-40.32);LTME組術后肛門首次通氣時間平均短1.13天(P<0.01,95%CI:-1.49~-0.78);LTME組術后平均住院時間平均短2.60天(P<0.01,95%CI:-1.49~-0.78);同時LTME組術后切口感染發生率更低(P<0.01,95%CI:0.19~0.43)。LTME組與OTME組比較,淋巴結清掃數、CRM陽性例數,吻合口瘺、腸梗阻發生率比較,差異均無統計學意義。以術中出血量為例,Meta分析森林圖及發表偏倚倒漏斗圖見圖1,其余相關指標分析結果以同樣方法得出。各指標Meta分析見表2。
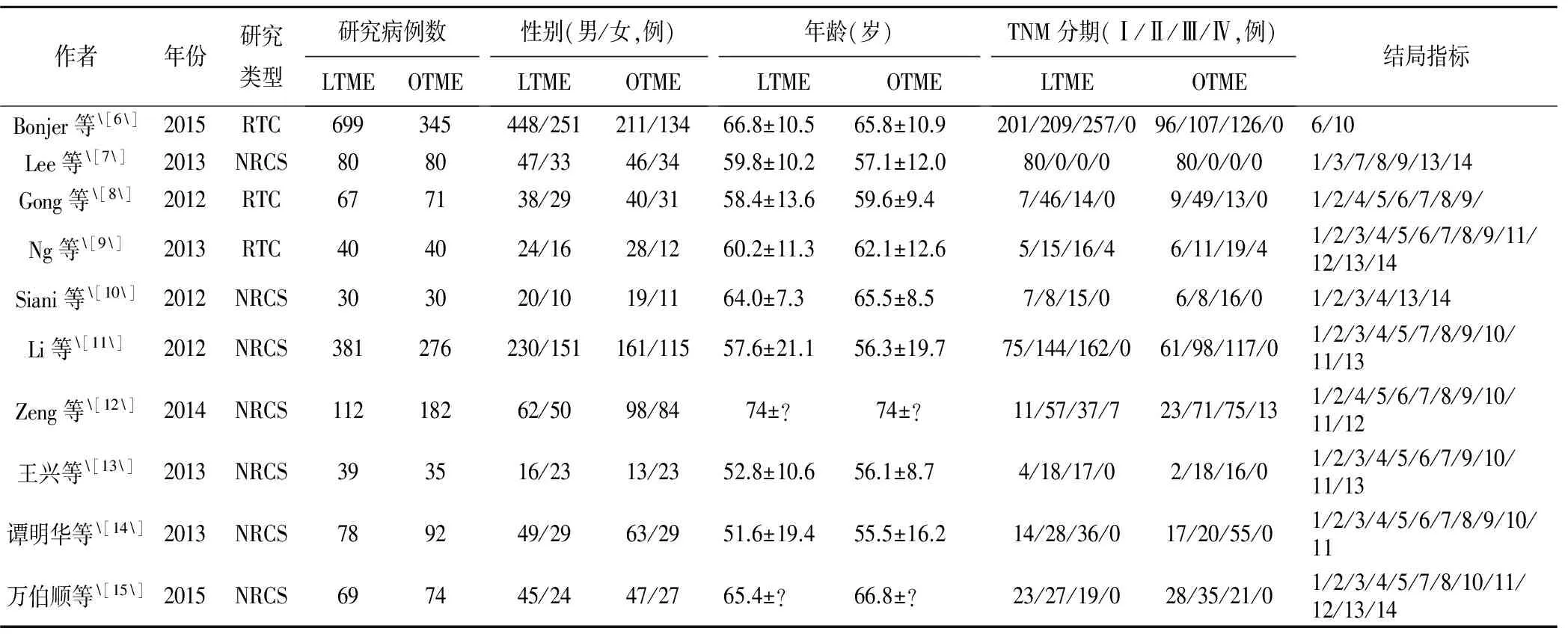
表1 納入研究的基本資料
注:結局指標中,1:手術時間;2:術中出血量;3:肛門通氣時間;4:術后平均住院時間;5:淋巴結清掃數;6:環切緣CRM陽性;7:吻合口瘺;8:腸梗阻;9:切口感染;10:隨訪3年局部復發;11:3年OS;12:3年DFS;13:5年OS;14:5年DFS

表2 圍手術期研究指標的Meta分析
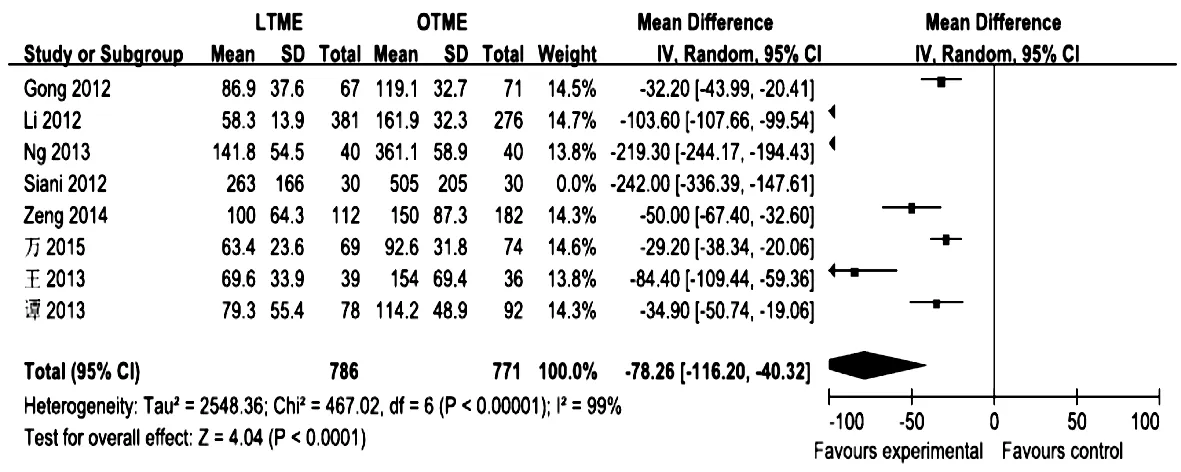

圖1 圍手術期術中出血Meta分析的森林圖及發表偏倚倒漏斗圖
2.預后相關指標:本研究提取隨訪3年局部復發、3年OS、3年DFS、5年OS、5年DFS共5個指標。LTME與OTME比較,3年局部復發(RR=1.14,P>0.05,95%CI:0.76~1.73)、3年OS(HR=0.92,P>0.05,95%CI:0.71~1.19)、3年DFS(HR=0.95,P>0.05,95%CI:0.75~1.21)、5年OS(HR=0.99,P>0.05,95%CI:0.84~1.16)、5年DFS(HR=1.01,P>0.05,95%CI:0.0.58~1.76)比較,差異均無統計學意義。見表3。
討 論
20世紀90年代,腹腔鏡技術開始用于結直腸腫瘤的治療,其優勢、短期療效及遠期療效在一些RTCs研究中被證實。在2005年,美國結直腸外科醫師協會(ASCRS)發表了一個關于腹腔鏡治療直腸腫瘤的聲明:由于缺乏5年生存數據,腹腔鏡直腸切除術治愈癌癥過早被認可[16]。直到2012年NCCN的直腸癌臨床實踐指南依舊認為,由于缺乏LTME與OTME的長期療效的比較,LTME術只適合臨床試驗[17]。2015版中國結直腸癌診療規范則首次出現腹腔鏡結腸腫瘤切除的條件[18]。由此看來,LTME手術的遠期療效及安全性仍缺乏大樣本、多中心的RTCs。

表3 預后相關研究指標的Meta分析
本系統評價納入10篇中外文文獻,分析了LTME組對比OTME組的短期及長期療效,結果顯示,圍手術期指標中,術中出血量、肛門首次通氣時間、術后平均住院時間、切口感染LTME組均少于OTME組,同時LTME組手術時間長于OTME組,而淋巴結清掃數、CRM陽性、吻合口瘺、腸梗阻兩組間均無明顯統計學差異。遠期療效相關指標3年局部復發、3年OS、3年DFS、5年OS、5年DFS,LTME相較于OTME組均無明顯統計學意義。本研究結果與Jiang等[19]研究小組所得Meta分析結果相近。
本系統評價的局限性:(1)納入的對照研究僅有三篇報告了具體隨機方法,總體質量一般;(2)納入研究總數偏少,結局指標不盡相同,導致部分結局指標偏少;(3)部分結局指標異質性較大,在一定程度上影響結果的可靠性;(4)檢索文獻僅限于中英文,有一定程度的語言偏倚。
[1] Liu,Y,Yao H,Gao G.Review for the NCCN clinical guideline in oncology of rectal cancer on surgical treatment from 2005 to 2015[J].Zhonghua Wai Ke Za Zhi,2015,53(1): 68-71.
[2] Lin S,Jiang HG,Chen ZH,et al.Meta-analysis of robotic and laparoscopic surgery for treatment of rectal cancer[J].World J Gastroenterol,2011,17(47):5214-5220.
[3] Lo CK,Mertz D,Loeb M.Newcastle-Ottawa Scale: comparing reviewers' to authors' assessments[J].BMC Med Res Methodol ,2014 ,14(1):45.
[4] Parmar MK,Torri V,Stewart L.Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints[J].Stat Med,1998,17(24):2815-2834.
[5] Tierney JF,Stewart LA,Ghersi D,et al.Practical methods for incorporating summary time-to-event data into meta-analysis[J].Trials,2007,8(1):16.
[6] Bonjer HJ,Deijen CL,Abis GA,et al.A randomized trial of laparoscopic versus open surgery for rectal cancer[J].New Engl J Med,2015,372(14):1324-1332.
[7] Lee SD,Park SC,Park JW,et al.Laparoscopic versus open surgery for stage i rectal cancer: long-term oncologic outcomes[J].World J Surg,2013,37(3):646-651.
[8] Gong J.Short-term outcomes of laparoscopic total mesorectal excision compared to open surgery[J].World J Gastroenterol,2012,18(48):7308.
[9] Ng SS,Lee JF,Yiu RY,et al.Laparoscopic-assisted versus open total mesorectal excision with anal sphincter preservation for mid and low rectal cancer: a prospective,randomized trial[J].Surgical Endoscopy,2014,28(1):297-306.
[10]Siani L M,Ferranti F,Benedetti M,et al.Laparoscopic versus open total mesorectal excision for stage I-III mid and low rectal cancer: a retrospective 5 years analysis[J].G Chir,2012,33(11-12):404-408.
[11]Li Z,Ying X,Shen Y,et al.Laparoscopic versus open surgery for rectal cancer: a clinical comparative study[J].J Int Med Res,2012,40(4):1599-1607.
[12]Zeng W,Zhou Z,Hou H,et al.Outcome of laparoscopic versus open resection for rectal cancer in elderly patients[J].J Surg Res,2015,193(2):613-618.
[13]王興,周毅,林啟謀,等.腹腔鏡輔助低位直腸癌保肛手術與傳統開腹手術的療效對比分析[J].消化腫瘤雜志(電子版),2013,5(2):104-108.
[14]譚明華,朱勁濤,呂益中,等.腹腔鏡輔助與傳統開腹直腸癌根治術的療效比較[J].消化腫瘤雜志(電子版),2013,5(3):168-171.
[15]萬伯順,陳躍宇,史佩東,等.腹腔鏡與開腹低位直腸癌根治術的療效對比[J].結直腸肛門外科,2015,21(1):24-28.
[16]Tjandra JJ,Kilkenny JW,Buie WD,et al.Practice parameters for the management of rectal cancer(revised)[J].Dis Colon Rectum.2005,48(3):411-423.
[17]Benson AB 3rd,Bekaii-Saab T,Chan E,et al.Rectal cancer[J].J Natl Compr Canc Netw,2012,10(12):1528-1564.
[18]中華人民共和國衛生和計劃生育委員會醫政醫管局,中華醫學會腫瘤學分會.中國結直腸癌診療規范(2015版)[J].中華消化外科雜志,2015,14(6):783-799.
[19]Jiang J,Jiang K,Dai Y,et al.Laparoscopic versus open surgery for mid-low rectal cancer: a systematic review and Meta-analysis on short- and long-term outcomes[J].J Gastrointest Surg,2015,19(8):1497-1512.
(本文編輯:彭波)
Laparoscopic versus open total mesorectal excision for rectal cancer:a Meta-analysis
YEJiayou,LIYuanqiang,MASonghe,etal.
(DepartmentofGastrointestinalSurgery,theFirstClinicalMedicalCollegeofThreeGorgesUniversity,YichangCentralPeople'sHospital,Hubei443000,China)
Objective To evaluate the clinical outcomes of laparoscopic versus open surgery for rectal cancer.Methods A search of Pubmed,EMBASE,Cochrane library,CNKI,Wangfang and VIP database was undertaken and studies published from Sep.2010 to Sep.2015 were identified.Two evaluators independently reviewed articles,extracted data and cross-checked the quality of included studies according to Cochrane Handbook.Meta-analyses were conducted by using RevMan5.1 software.Results Ten studies met the final inclusion criteria.A total of 2820 patients undergoing rectal surgery were examined,including 1595 cases in the laparoscopic total mesorectal excision(LTME)group and 1225 cases in the open total mesorectal excision(OTME)group.Meta-analysis showed that the amount of operation time in the LTME group was longer than the OTME group(MD=30.34,95%CI:21.61 to 39.0,P<0.00001); the amount of blood loss during operation in the LTME group was smaller than the OTME group(MD=-78.26,95%CI:-116.20 to -40.32,P<0.0001,); the time of first flatus(MD=-1.13,P<0.00001,95%CI:-1.49 to -0.78)and postoperative hospital stay(MD=-2.6,P<0.00001,95%CI:-3.5 to -1.7)in the LTME group were shorter than the OTME group; the morbidity of postoperative wound infection in the LTME group was lower than the OTME group(RR=0.28,P<0.00001,95%CI:0.19 to 0.43).There were no significant differences in the number of harvested lymph nodes,the positive rate of circumferential margin,the rate of anastomotic leak or obstruction between the two groups.In the long-term effects,there were no significant differences in 3-year postoperative local recurrence,3-year overall survival and disease-free survival,and 5-year survival and disease free survival between the groups.Conclusion This study suggests that the long-term outcomes of LTME appear to be equivalent to the open surgery for treatment of rectal cancer.Besides,it has more favorable short-term benefits,fewer intraoperative blood lost,shorter time to first flatus and postoperative hospital stay,and lower rate of postoperative wound infection.
laparoscopic; open surgery; outcomes; rectal cancer; Meta-analysis
10.3969/j.issn.1005-6483.2017.02.014
443000 湖北宜昌,三峽大學第一臨床醫學院(宜昌市中心人民醫院)
陳愛軍,Email:chenaijun@163.net
2015-12-13)
猜你喜歡
腹腔鏡外科雜志(2022年7期)2022-08-16 04:31:06
民用飛機設計與研究(2020年4期)2021-01-21 09:15:02
中華養生保健(2020年1期)2020-11-16 00:47:38
中國中醫急癥(2019年10期)2019-05-21 07:20:30
電子制作(2018年18期)2018-11-14 01:48:24
中國醫藥指南(2017年3期)2017-11-13 02:57:31
中國內鏡雜志(2017年2期)2017-03-20 16:18:12
山東工業技術(2016年15期)2016-12-01 05:31:22
腹腔鏡外科雜志(2016年11期)2016-06-01 12:10:09
腹腔鏡外科雜志(2016年9期)2016-06-01 12:10:07