急性冠狀動脈綜合征患者治療后出血的相關因素分析
2017-01-12 17:02:06牛光美鄭容梅
現代儀器與醫療 2016年6期
關鍵詞:影響因素
牛光美 鄭容梅
[摘 要] 目的:探討急性冠狀動脈綜合征(Acute coronary syndrome,ACS)患者治療后出血的相關因素,為預防出血提供參考。方法:對我科收治的955例ACS患者進行回顧性分析,按照其治療后出血發生情況分為出血組、未出血組,統計出血發生率,比較兩組患者臨床資料并歸納影響ACS患者治療后合并出血的相關因素,探討防治策略。結果:955例患者中,共有48例患者發生治療后出血,發生率為5.03%。Logistic多因素回歸分析示,年齡≥65歲、非ST段抬高型心肌梗死、既往出血事件、既往CABG手術史、合并腎衰、合并心衰、合并血小板減少、接受氯吡格雷治療、接受糖蛋白Ⅱb/Ⅲa受體拮抗劑治療是影響ACS患者治療后合并出血的獨立危險因素。結論:ACS患者治療后合并出血發生風險較高,年齡、既往史、合并癥、治療方案均可影響出血事件發生率,應早期評估患者出血風險,制定個體化治療方案。
[關鍵詞] 急性冠狀動脈綜合征;出血;影響因素
中圖分類號:R541.4 文獻標識碼:B 文章編號:2095-5200(2016)06-021-03
DOI:10.11876/mimt201606008
Analysis on correlation factors of hemorrhage after treatment in patients with acute coronary syndrome NIU Guangmei,ZHENG Rongmei. (Department of cardiologyThe,Third People,s Hospital of Guangyuan,Guangyuan 628400 China)
[Abstract] Objective: This study aimed to investigate the related factors of hemorrhage in patients with acute coronary syndrome (ACS) after treatment, and to provide reference for the prevention of bleeding. Methods: 955 cases of patients with ACS were retrospectively analyzed, and divided into bleeding group and non-bleeding group according to the occurrence of bleeding after treatment, bleeding incidence was stastically analyzed, clinical data were compared between the two groups, the related factors influencing the hemorrhage of ACS patients after treatment, and the prevention and treatment strategies were discussed. Results: Among 955 patients, there were 48 patients with hemorrhage after treatment, the incidence rate was 5.03%. Logistic regression analysis showed that age more than 65 years old, non-ST-elevation myocardial infarction, previous bleeding, previous coronary artery bypass grafting surgery (CABG) surgery, complicated with renal failure, heart failure and thrombocytopenia, accepting clopidogrel therapy and glycoprotein II b/ III a receptor antagonist therapy were independent risk factors of the hemorrhage after treatment of ACS patients. Conclusions: There is high risk bleeding incidence in ACS patients after treatment, age, past history, complication, treatment therapy affect the incidence of bleeding events, the risks of hemorrhage in ACS patients should be early assessed for making individualized treatment decisions.
[Key words] acute coronary syndrome; hemorrhage; influencing factors
急性冠狀動脈綜合征(Acute coronary syndrome,ACS)發病率及死亡率均處于較高水平,在全球范圍內造成了極大的醫學及社會經濟負擔[1]。經皮冠脈介入治療(Percutaneous coronary intervention,PCI)可通過重新開放狹窄甚至閉塞的冠脈管腔,改善心肌血流灌注,在近年來ACS的臨床治療中得到了廣泛應用[2]。但隨著急診溶栓、PCI及冠脈搭橋術的廣泛開展及抗凝、抗血小板藥物的大量應用,近年來ACS患者治療后出血的發生風險不斷上升,影響患者預后質量[3]。因此,尋求臨床治療及預防出血的平衡點,可提高ACS治療效果。本研究選取955例ACS患者進行回顧性分析,旨在明確患者治療后合并出血相關因素。
1 資料與方法
1.1 納入標準與排除標準
于我院2012年5月至2016年5月收治的ACS患者中進行篩選。納入患者參照文獻相關標準確診ACS[4]:①心電圖2個或以上相鄰導聯ST段下移≥0.1 mV;②可見典型急性心肌梗死心電圖演變;③心肌損傷標志物上升;④冠脈造影結果示至少1支主要血管管腔狹窄程度≥75%。符合上述任意1條標準即可確診。臨床資料保存完整。排除合并肥厚型心肌病、合并血液系統疾病或高危出血傾向、合并嚴重肝、腎功能不全、合并阿司匹林、氯吡格雷使用禁忌證、合并惡性腫瘤。共955例符合標準者納入分析。
1.2 分析方法
1.2.1 出血事件分析 出血評價方法[5]:重度:出現顱內出血或心臟填塞,血紅蛋白(Hb)下降>50 g/L
或血細胞比容(PCV)下降>15%。;中度:出血部位明確,Hb下降30~50 g/L,PCV下降>10%,或出血部位不明確,Hb下降40~50 g/L,PCV下降12%~15%;輕度:臨床、影像學可見明顯出血表現,Hb下降<30 g/L,PCV下降<9%。將治療后出血者納入出血組,將未出血者納入未出血組,計算患者治療后出血事件發生率。
1.2.2 相關因素分析 比較兩組患者一般臨床資料差異,計數資料以(n/%)表示,并采用χ2檢驗,計量資料以(x±s)表示,將存在統計學差異的因素納入Logistic多因素回歸分析,總結影響ACS患者治療后合并出血的相關因素,并分析預防策略。
2 結果
2.1 出血事件發生率
955例患者中,共有48例患者發生治療后出血,發生率為5.03%。出血患者中,顱內出血15例,臟器出血11例,體表出血22例,出血事件分度:重度5例,中度31例,輕度12例。
2.2 一般資料比較
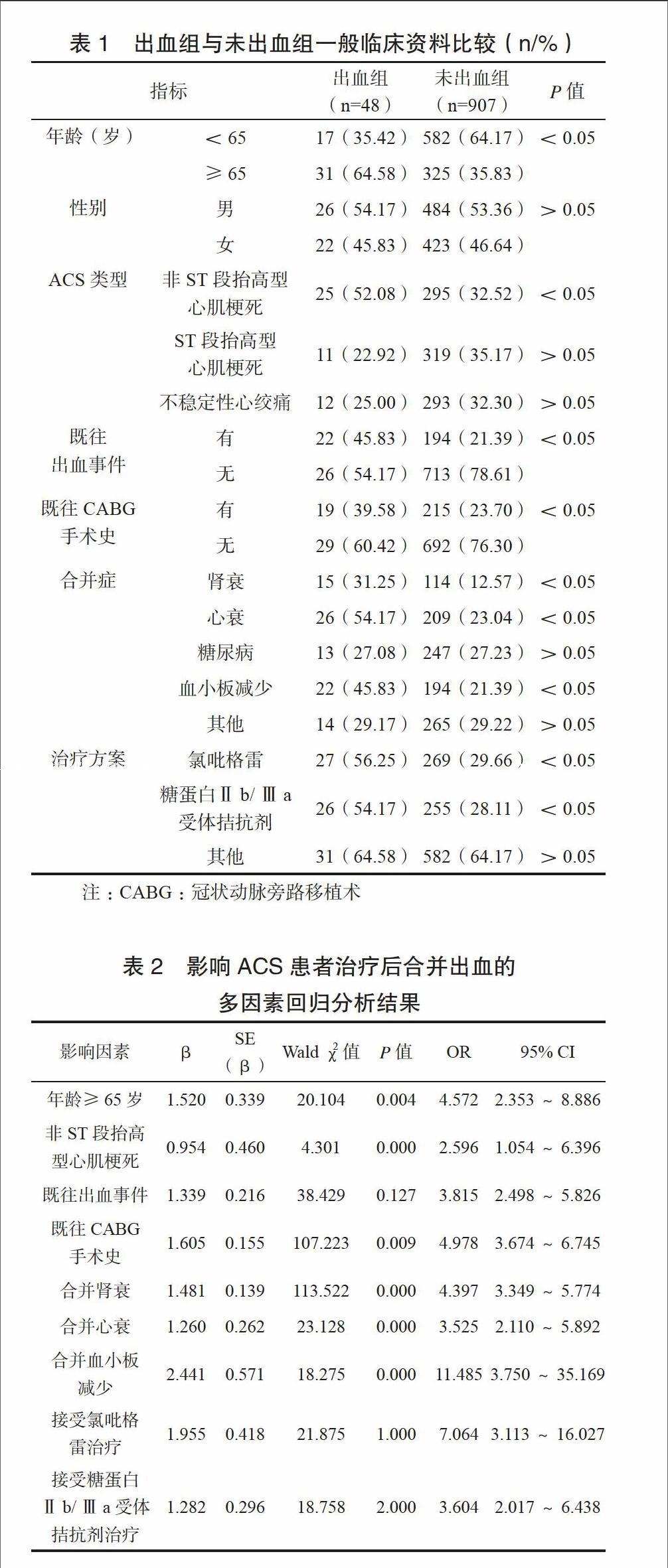
一般資料單因素分析可見年齡、ACS類型、既往出血時間、既往CABG手術史、合并心衰等、治療方案比較,差異有統計學意義(P<0.05),見表1。
2.3 Logistic多因素回歸分析
將單因素分析有統計學差異指標納入Logistic多因素回歸分析,如表2所示:年齡≥65歲、非ST段抬高型心肌梗死、既往出血事件、既往CABG手術史、合并腎衰、合并心衰、合并血小板減少、接受氯吡格雷治療、接受糖蛋白Ⅱb/Ⅲa受體拮抗劑治療是影響ACS患者治療后合并出血的獨立危險因素(P<0.05)。
3 討論
本研究955例患者治療后出血發生率達5.03%,ACS患者治療后出血事件往往具有進展快、治療矛盾、后果嚴重等特點[6],因此,在ACS患者的臨床治療中,如何尋求預防缺血及引發出血的平衡,早期識別治療后合并出血高危人群十分關鍵[7-8]。
研究表明,年齡每增加10歲,患者出血風險即上升1%[9],加之老年患者往往伴有高血壓、心腦血管系統疾病、慢性呼吸系統疾病等合并癥,常年服用阿司匹林等非甾體抗炎藥,藥物對血小板凝血功能的影響及胃粘膜的損傷大大增加了臟器出血發生風險。Xian等[10]認為,老年人群血管硬化、心功能下降、循環功能衰退、新陳代謝下降等病理生理改變亦導致臟器儲備代償功能不良、組織粘膜保護能力下降,增加出血事件風險。非ST段抬高型心肌梗死患者病情往往較重,需接受更大劑量溶栓、抗凝、抗血小板藥物治療,藥物對患者凝血功能的影響可導致其出血風險上升。既往有出血事件及CABG手術史患者,其凝血功能往往不夠理想,加之過往出血、抗凝治療的矛盾與復雜病變的長期介入操作,均在增加出血機會中扮演了重要角色[11-12]。Mega等[13]發現,合并嚴重腎功能不全患者,其出血風險較殘存腎功能患者增加4倍,而合并心衰患者均處于血容量減少、心肌耗氧量增加狀態,血管長期受損,出血不易終止,大出血發生風險更高[14]。
本研究顯示氯吡格雷可導致出血發生率增加,但亦有學者指出,氯吡格雷不會導致致命性出血、失血性休克發生風險增加,安全性仍值得肯定[15-16]。作為冠心病的二級預防用藥,糖蛋白Ⅱb/Ⅲa受體拮抗劑單獨應用不會導致ACS患者治療后出血風險升高,但由于多數患者均接受肝素抗凝治療,糖蛋白Ⅱb/Ⅲa受體拮抗劑聯合大劑量肝素可導致嚴重出血并發癥風險急劇上升[17]。
因此,在今后的臨床實踐中,應早期意識到老年ACS患者治療后合并出血風險,嚴格控制抗凝、抗血小板藥物的劑量及使用時間,針對存在危險因素的患者提倡出血事件的早預防、早發現、早治療[18],避免潛在、不必要出血事件的發生。
參 考 文 獻
[1] Alexopoulos D, Stavrou K, Koniari I, et al. Ticagrelor vs prasugrel one-month maintenance therapy: impact on platelet reactivity and bleeding events[J]. Thromb Haemost, 2014, 112(3): 551-557.
[2] 孫靜. 介入治療對高齡急性冠狀動脈綜合征患者預后的影響[D]. 承德:承德醫學院, 2015.
[3] Ducrocq G, Schulte P J, Becker R C, et al. Association of spontaneous and procedure-related bleeds with short-and long-term mortality after acute coronary syndromes: an analysis from the PLATO trial[J]. EuroIntervention, 2015, 11(8): 737-745.
[4] 許俊堂, 胡大一. 對急性冠狀動脈綜合征分型的看法[J]. 中華心血管病雜志, 2001, 29(09):566-568.
[5] Mega J L, Braunwald E, Murphy S A, et al. Rivaroxaban in Patients Stabilized After a ST-Segment Elevation Myocardial Infarction: Results From the ATLAS ACS-2–TIMI-51 Trial [J]. J Am Coll Cardiol, 2013, 61(18): 1853-1859.
[6] Kaul P, Tanguay J F, Newby L K, et al. Association between bleeding and mortality among women and men with high-risk acute coronary syndromes: insights from the Early versus Delayed, Provisional Eptifibatide in Acute Coronary Syndromes (EARLY ACS) trial[J]. Am Heart J, 2013, 166(4): 723-728.
[7] 曾秋棠, 彭昱東. 關注急性冠狀動脈綜合征抗栓和出血的平衡[J]. 臨床心血管病雜志, 2013, 29(5): 321-323.
[8] Chhatriwalla A K, Amin A P, Kennedy K F, et al. Association between bleeding events and in-hospital mortality after percutaneous coronary intervention[J]. JAMA, 2013, 309(10): 1022-1029.
[9] 張予. 急性冠狀動脈綜合征相關研究[D]. 武漢:華中科技大學, 2014.
[10] Xian Y, Wang T Y, McCoy L A, et al. Association of Discharge Aspirin Dose With Outcomes After Acute Myocardial Infarction Insights From the Treatment with ADP Receptor Inhibitors: Longitudinal Assessment of Treatment Patterns and Events after Acute Coronary Syndrome (TRANSLATE-ACS) Study[J]. Circulation, 2015, 132(3): 174-181.
[11] Tang X F, Fan J Y, Meng J, et al. Impact of new oral or intravenous P2Y12 inhibitors and clopidogrel on major ischemic and bleeding events in patients with coronary artery disease: a meta-analysis of randomized trials[J]. Atherosclerosis, 2014, 233(2): 568-578.
[12] 何菲, 殷躍輝, 李芝峰, 等. 不同性別急性冠脈綜合征患者的臨床特征分析:480例回顧性研究[J]. 解放軍醫學雜志, 2014, 39(6): 489-493.
[13] Mega J L, Braunwald E, Wiviott S D, et al. Comparison of the Efficacy and Safety of Two Rivaroxaban Doses in Acute Coronary Syndrome (from ATLAS ACS 2–TIMI 51)[J]. Am J Cardiol, 2013, 112(4): 472-478.
[14] Krantz M J, Kaul S. The ATLAS ACS 2–TIMI 51 Trial and the Burden of Missing Data:(Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects With Acute Coronary Syndrome ACS 2–Thrombolysis In Myocardial Infarction 51)[J]. J Am Coll Cardiol, 2013, 62(9): 777-781.
[15] 張偉, 孫中華, 米杰, 等. 三聯抗血小板對急性冠脈綜合征患者經皮冠狀動脈介入術后30天內的作用[J]. 中華急診醫學雜志, 2013, 22(7): 721-725.
[16] Levine G N, Jeong Y H, Goto S, et al. Expert consensus document: World Heart Federation expert consensus statement on antiplatelet therapy in East Asian patients with ACS or undergoing PCI[J]. Nat Rev Cardiol, 2014, 11(10): 597-606.
[17] Tantry U S, Bonello L, Aradi D, et al. Consensus and update on the definition of on-treatment platelet reactivity to adenosine diphosphate associated with ischemia and bleeding[J]. J Am Coll Cardiol, 2013, 62(24): 2261-2273.
[18] Klingenberg R, Heg D, R?ber L, et al. Safety profile of prasugrel and clopidogrel in patients with acute coronary syndromes in Switzerland[J]. Heart, 2015, 101(11): 854-863.
猜你喜歡
現代經濟信息(2016年19期)2016-10-20 18:46:44
現代經濟信息(2016年19期)2016-10-20 18:12:28
現代經濟信息(2016年19期)2016-10-20 16:20:30
中國科技博覽(2016年19期)2016-10-19 13:33:22
中國科技博覽(2016年18期)2016-10-19 10:49:54
中國科技博覽(2016年18期)2016-10-19 08:16:45
中國科技博覽(2016年18期)2016-10-19 06:39:44
中國市場(2016年36期)2016-10-19 03:54:01
中國市場(2016年35期)2016-10-19 02:30:10
商(2016年27期)2016-10-17 07:09:07