磁共振血管壁成像技術現狀及進展
2016-06-27 06:34:28李赟鐸周賾辰李睿苑純
磁共振成像 2016年2期
李赟鐸,周賾辰,李睿*,苑純
?
磁共振血管壁成像技術現狀及進展
李赟鐸1,周賾辰1,李睿1*,苑純2
[摘要]磁共振血管壁成像是利用磁共振原理抑制血管內流動血液信號,獲取血管壁等靜態組織圖像的一種成像方法。由于可以對血管壁進行直接成像,這種方法可以用于評估動脈粥樣硬化斑塊的形態、成分,進而確定斑塊的風險程度。血管壁成像技術的核心問題在于如何有效抑制流動血液的信號,本文就目前磁共振血管壁成像技術的現狀及進展做簡要的總結回顧。
[關鍵詞]磁共振成像;心血管疾病;動脈粥樣硬化斑塊
作者單位:1. 清華大學醫學院生物醫學工程系,生物醫學影像研究中心,北京 100084 2. 美國華盛頓大學放射學系血管成像實驗室,西雅圖
接受日期:2015-12-07
李赟鐸, 周賾辰, 李睿, 等. 磁共振血管壁成像技術現狀及進展. 磁共振成像,2016, 7(2): 142–148.
2Department of Radiology University of Washington, Box 357115, 1959 NE Pacific Ave, Seattle, WA 98195, USA
*Correspondence to: Li R, E-mail: leerui@tsinghua.edu.cn
Received 29 Otc 2015, Accepted 7 Dec 2015
ACKNOWLEDGMENTS This work was part of Fund Project of Beijing Municipal Science and Technology Commission(No. Z131100005213001).
因血管高危斑塊所引發的心腦血管疾病已經成為危害人類健康的頭號殺手。基于影像學手段的血管斑塊監測,對于心腦血管疾病的預測、分期和預后評估都有著非常重要的意義。好的影像學評估方法應能夠充分滿足臨床診治的需要,結合動脈粥樣硬化相關疾病的臨床實踐,其應盡可能滿足以下3點要求[1]:(1)具有非侵入性以保證可以進行短期和長期的研究;(2)能夠提供斑塊在不同時期的形態學、組織成分和炎癥反應的定量信息;(3)能夠被病理學的金標準所驗證。
磁共振成像設備是綜合了物理、電子、材料、計算機、數學、醫學等學科高新技術的現代化儀器。磁共振成像具有高軟組織對比度、多對比度成像、任意截面成像、無電離輻射等諸多優勢,在血管壁成像方面,磁共振成像可以滿足上述3個條件,具有廣闊的發展和應用空間。磁共振血管壁成像技術是基于磁共振物理原理,通過抑制血管內流動血液的信號來獲得血管壁等靜態組織信息的一種方法,能夠對動脈粥樣硬化斑塊的形態和成分進行評估。以下將簡要綜述磁共振血管壁成像技術的發展現狀、前沿進展和臨床應用。
1 磁共振血管壁成像技術
血管壁成像技術的核心問題在于如何有效抑制流動血液的信號,從而準確識別血管腔-壁交界,評估動脈粥樣硬化斑塊的形態和成分。筆者針對磁共振血管壁成像發展歷史上的一些重要技術作簡要綜述。
1.1傳統的二維血管壁成像技術
傳統的二維血管壁成像技術包括飽和帶技術、雙反轉恢復技術以及四反轉恢復技術。飽和帶技術[2-3]是通過在血流流入方向施加飽和帶來實現血流抑制的目的,該技術是最為“古老”的磁共振血管壁成像技術,但其血流抑制效果差容易出現血流偽影,現在已較少在臨床上應用;雙反轉恢復技術[4]通過分別施加一個非選擇性180度反轉脈沖和一個選擇性180度反轉脈沖來實現血流抑制,該方法是目前最常用的血流抑制方法,但由于恢復時間T1較長且只能單層采集,采集效率很低。為解決這一問題,Song HK等[5]提出了利用多層選擇反轉脈沖來提高采集效率,Yarnykh V等[6]隨后又提出了增加反轉脈沖層厚同時覆蓋多層的技術,但其血流抑制效果會受到一定的影響;而四反轉恢復技術[7]通過施加兩組雙反轉脈沖實現血流抑制,該技術對于血液T1值的波動不敏感,可以用于對比增強磁共振血管壁成像,但其原理和雙反轉恢復技術類似,采集效率很低。由于以上技術都基于血流流動方向與成像平面大體垂直這一假設,因此它們均依賴于流入效應來達到血流抑制的效果,無法進行層面內的血流抑制,基本上都只用于二維成像。與二維成像方式相比,三維成像具有采集效率和信噪比較高,以及可以實現各向同性分辨率采集等優勢,近年來,研究人員提出了若干適合三維成像的血管壁成像方法。
1.2運動敏感驅動平衡(motion sensitized driven equilibrium, MSDE)技術
MSDE被廣泛應用于磁共振血管壁成像中,該技術的原理主要是依靠MSDE準備脈沖內設置的梯度場各階矩,使血流散相,從而達到血流抑制的目的,血液流動模式越復雜、流動速度越快,則越容易通過該技術達到抑制效果。該技術最早于2007年被不同的兩個研究組先后提出[8-9],分別被用于3 T主動脈和頸動脈成像上。2010年通過引入雙聚相脈沖針對MSDE準備脈沖的渦流響應及B0和B1特性進行了優化,優化后的技術稱為iMSDE[10](improved MSDE),并結合散相梯度回波(spoiled gradient echo, SPGR)采集方式,得到三維各向同性分辨率血管壁圖像,該技術被稱為3DMERGE技術[11],對管壁增厚程度(斑塊尺寸)的測量更為準確。最近,Obara M等人[12]通過在iMSDE前設置一對雙極性梯度波形,對渦流響應又進行了進一步改善,從而得到了信號強度更為均勻的腦組織圖像。目前,MSDE技術可以實現在很短的時間內(0~18 ms)達到大范圍抑制血流的效果,同時對于主磁場B0和發射場B1的不均勻性也具備一定的抵抗能力。但這種方法在預脈沖當中采用了T2準備脈沖和雙極梯度,從而導致圖像信噪比下降并使圖像的對比度帶有一定的T2和擴散加權。
1.3T2IR技術
2010年,Liu CY等[13]提出了一類只依賴于縱向弛豫時間T1和橫向弛豫時間T2的選擇性血流抑制方法(T2-prepared Inversion Recovery, T2IR),結合二維快速自旋回波(turbo spin echo, TSE)作為數據采集模塊,在1.5 T下被用于主動脈的大范圍成像。2011年在采集方面,利用平衡穩態自由進動(balanced steady state free precession, bSSFP)替換了TSE,序列的采集效率得以改進,被用于1.5 T下肢腘動脈的成像[14]。T2IR還可以與相位敏感技術結合,以犧牲采集效率為代價進一步改善了管腔和管壁之間的對比度,被用于3 T下三維下肢動脈管壁的成像[15]。T2IR技術表面上回避了血液流動問題,但由于特異性選擇血液信號需要較長的T2準備脈沖時間(≥40 ms),使得其無法覆蓋流速較慢或極快的血液。此外,B0和B1場在成像區域內存在不均勻性,有可能導致T2準備脈沖失效,從而對血流抑制的效果造成影響。
1.4DANTE技術
最近有研究人員針對三維黑血預脈沖提出了變延遲進動定制激發(delays alternating with nutation for tailored excitation, DANTE)的血流抑制方法[16],通過連續的小角度激發脈沖結合散相梯度,使得處于運動和靜止的物質產生不同的穩態信號,從而達到抑制血液信號的目的,該方法對于B0和B1的不均勻性不敏感。相對于MSDE方法,DANTE的優勢在于,其對靜態組織信號的保護比較好。但是DANTE的問題在于,如果要達到較好的血流抑制效果,需要反復施加DANTE的血流抑制小單元,使得整個準備模塊的時間較長。同時,該方法對于梯度系統的要求也較高,需要梯度場能夠在短時間內攀升到相對比較大的梯度強度。目前基于該方法已經建立起檢測斑塊內出血(intra plaque hemorrhage, IPH)的三維快速成像序列[17]。DANTE對于流速較慢的腦脊液(cerebral spinal fluid, CSF)也能起到比較好的信號抑制作用,可以為頸部脊髓成像[18]和顱內管壁成像[19]提供更好的對比度。
1.5SNAP技術
此外,針對斑塊特定危險成分的檢測如IPH,也引起了磁共振成像領域的廣泛關注。高鐵血紅蛋白作為一種內源性對比劑,它將導致縱向弛豫常數T1的縮短,從而在T1加權圖像上產生高信號。因此,高鐵血紅蛋白的存在促進了磁共振對IPH的識別,目前最為經典的IPH檢測序列是基于反轉準備脈沖的快速梯度回波(magnetization prepared rapid gradient echo, MPRAGE)序列[20],它既可以顯示出IPH,也可以達到抑制管腔內血液信號的作用[21]。2010年,Wang J等人[22]設計出體選擇相位敏感反轉(slab-selective phase-sensitive inversion-recovery, SPI)序列,該技術降低了對血液T1值估計和序列參數設置準確性的要求,提高了管壁管腔的對比度以及IPH和正常管壁之間的對比度。通過進一步優化采集方式和成像參數,Wang J等人[23]又于2013年提出非增強血管造影和IPH同時成像(simultaneous noncontrast angiography and intraPlaque hemorrhage, SNAP)序列,該技術利用一次采集,就可以同時得到磁共振血管造影的信息以及IPH的分布信息,避免了采集效率上的損失。
1.6變角度多自旋回波序列
基于自旋回波序列的各種改進構成了血管壁成像方法的另一大類,為了提高采集效率,一般都采用帶有回波鏈的快速自旋回波進行成像,這種序列當中存在大量的180度回聚脈沖,一方面會使采集效率變低,另一方面會產生過高的特定吸收率(specific absorption rate, SAR)。針對這一問題,一系列基于拓展相位圖(extended phase graph,EPG)方法設計的變角度硬脈沖方法[24-26]應運而生,可以使快速自旋回波在高場下能夠完成三維大范圍成像采集。另一方面,變角度的回聚脈沖對于抑制血流也會產生更好的效果[27-28],這是由于變角度回聚脈沖會產生多條回波通路,使得分布在回聚脈沖前后的散相梯度對運動變得更為敏感,這一現象也能夠通過類似DANTE的血流抑制原理來解釋。此外有研究人員還通過在第一個180度回聚脈沖前后各引入一個單極梯度,進一步改善變角度回聚TSE序列的血流抑制效果[29]。這一系列改進使得TSE序列可以應用于從顱內動脈至下肢動脈的全身各部位血管床的黑血管壁成像[29-32]。該序列雖然保證了管壁信號具有足夠高的SNR,但其采集效率相對于梯度回波序列而言較低。
伴隨著磁共振軟硬件技術的迅速發展,磁共振血管壁成像技術已日趨成熟,成像空間維度由二維發展到三維,成像范圍不斷擴大,血流抑制效果不斷優化,對于管壁斑塊成分的識別和定量分析也更加準確。血管壁成像技術的發展歷程詳見圖1。
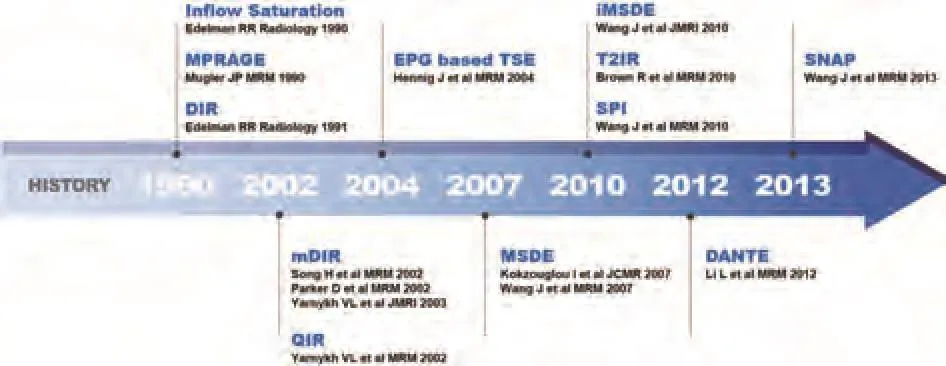
圖1 血管壁成像技術的發展歷程Fig. 1 The development of vessel wall imaging techniques
2 臨床應用
在臨床上,磁共振血管壁成像技術被用于多個血管床成像,針對不同血管床的結構和血流,研究人員開發了不同的技術,以滿足相應的臨床應用需求。
頸動脈因其所處位置較為表淺,并且尺寸與磁共振成像的分辨率較為匹配,因此針對頸動脈血管壁已建立起較為成熟的磁共振動脈粥樣硬化斑塊風險評估體系[33-35]。臨床上,研究人員通過多對比度成像的方法,可以識別血管斑塊的成分,如斑塊內出血(intra-plaque hemorrhage, IPH)、鈣化(calcification, CA)、脂質核(lipid rich necrotic core, LRNC)、纖維帽(fibrous cap, FC)等,進而達到對血管斑塊定量分析的目的。目前采用的二維成像序列包括T1和T2加權的TSE序列,以及三維飛行時間(time of flight, TOF)序列。以上3個序列與質子密度加權的基準序列配合,可以用來識別鈣化和脂質核。此外,利用釓對比劑增強T1加權圖像,可以使脂質核的評估更為準確,同時對比劑增強也有利于識別及測量纖維帽。不同斑塊成分所對應的圖像強度特性見表1。
除頸動脈以外,也有大量針對顱內血管床管壁成像的研究,通過多對比成像的方式來進行顱內斑塊成分的識別[36-37]。顱內血管床由于走形迂曲,且血管內徑較細,對磁共振血管壁成像技術提出了諸多挑戰。最近,有研究者將變角度TSE序列和DANTE配合使用,應用于大范圍顱內外血管壁成像,成像質量和血流抑制效果都顯著優于單獨使用變角度TSE序列[38]。目前顱內血管壁成像技術的分辨率已經可以觀測到大腦中動脈[39-40],文獻報道的最高的三維成像空間分辨率達到0.4~0.5 mm(各向同性)[31]。
近年來,也有研究開始將血管壁成像應用于冠狀動脈的評估。與頸動脈和顱內動脈相比,冠狀動脈管壁面臨著更多的技術挑戰,包括心臟搏動、呼吸所造成的運動偽影,以及冠脈管壁較細等,都對成像的時間和空間分辨率提出了一定要求。早期的研究嘗試通過二維TSE成像并要求受試者屏氣[41]或使用導航門控[42]的方式,對冠脈進行管壁成像。為了實現快速采集,三維螺旋采集[43]和放射狀采集[44]技術,也被用于三維冠脈管壁成像。以上技術也逐步開始應用于冠脈外向重構[45-50](outward remodeling)、冠脈斑塊[51-54]和對比劑增強成像[55-58]的研究,但成像質量和穩定性都有待提高。近年來,有研究者提出多時相冠脈管壁成像[59-60](multiphase acquisitions)的技術,與以往只采集心動周期單個特定時相的圖像不同,多時相管壁成像在一個心動周期內,選擇多個時間點進行采集,允許圖像判讀人員從多幅圖像選擇質量最優的進行分析,這樣使得總體成像的質量和穩定性得到提升。
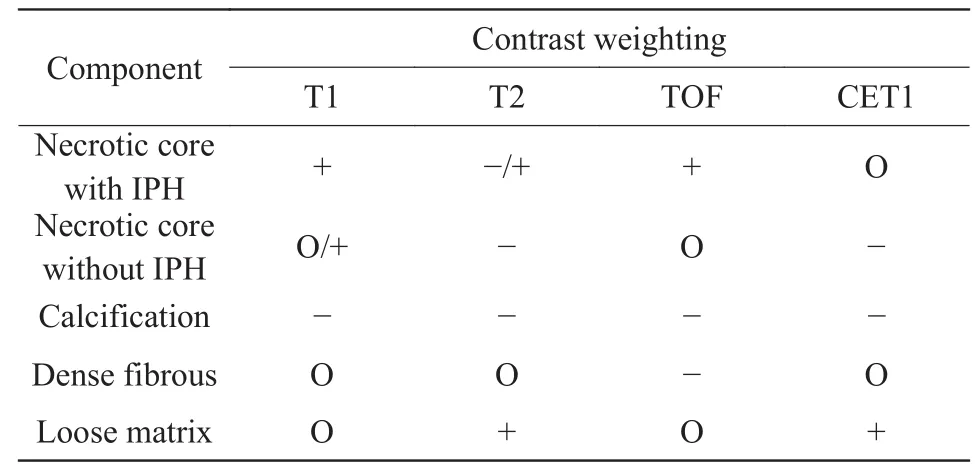
表1 多對比度磁共振斑塊成分區分標準[34]Tab. 1 Criteria for the identification of plaque components in MR plaque imaging[34]
3 問題及展望
傳統的多對比度血管壁成像技術,在技術層面還存在一些問題亟待解決和優化:(1)目前還需要通過掃描多個序列才能獲取血管壁的較為完整的信息,這就會帶來諸如掃描時間較長、因病人在序列間隙移動而導致序列之間的圖像錯配、以及臨床上圖像判讀復雜等問題;(2)受限于線圈覆蓋范圍等技術問題,傳統的血管壁成像技術的成像范圍較小,難以對諸如顱內外血管床等大范圍血管床進行全面評估;(3)目前的血管壁成像技術成像速度較慢,單次檢查至少需要15~20 min,限制了其在臨床上的應用。針對這些問題,在今后的研究中,磁共振血管壁成像技術還可以進一步發展。
近年來,研究人員在已有血管壁成像技術的基礎上,又提出了一些新的成像方案。2014年,Fan Z等人[61]開發了MATCH(multi-contrast atherosclerosis characterization)技術,實現了在5 min之內采集多對比度的2D圖像。通過在一個重復時間(repetition time,TR)中多次采集,MATCH可以獲取到T1、T2加權,以及灰血的圖像,通過解讀這些圖像,可以在一個成像序列內分辨出斑塊內出血、鈣化和脂質核等斑塊成分信息。該技術目前只實現了2D成像,并且覆蓋范圍僅限于頸動脈。
為了對顱內外血管同時成像,在臨床上全面評估顱內外血管病變,清華大學生物醫學影像研究中心利用自主研發的36通道神經血管線圈,采用3D-MERGE、VISTA(volumetric isotropic TSE acquisition)序列和SNAP序列,實現了可覆蓋頸動脈直至顱內的大范圍多對比度3D黑血成像[62](圖2)。該方法可以在15 min之內完成大范圍多對比度的三維血管壁圖像,其較長的掃描時間在一定程度上限制大范圍血管壁成像技術在臨床上的應用。
通過數據降采,在圖像重建層面實現快速成像,也是未來磁共振血管壁成像領域的一個重要發展方向。近年來,有研究嘗試將壓縮感知和3DMERGE序列結合,在不影響血流抑制效率和成像質量的情況下,提高了成像速度[63-65]。Gong E等人[66]利用多對比度不同序列圖像中可共享的信息,優化了壓縮感知結合部分并行成像,提出了可應用于血管壁多對比度成像的應用可共享數據的并行成像及壓縮感知的重建方法(parallelimaging and compressed sensing reconstruction of multicontrast imaging using sharablE information,PROMISE),該方法對于序列之間病人的運動更為不敏感,提高了管壁斑塊多對比度圖像的重建質量。Zhou Z等人[67]開發了一種基于自支撐定制k空間估計的并行成像(self-supporting tailored k-space estimation for parallel imaging reconstruction,STEP)方法,進一步提升了重建質量。

圖2 經曲面重建后的大范圍多對比度黑血成像,覆蓋范圍從頸總動脈至大腦中動脈。從上至下依次為SNAP、T2w-VISTA和MERGEFig. 2 Large-coverage multi-contrast black blood imaging (after curved reconstruction), which covers an area from common carotid artery to middle cerebral artery. Different imaging sequences are SNAP(upper panel), T2-VISTA(middle panel) and MERGE(lower panel), respectively.
4 總結
綜合以上討論,磁共振血管壁成像可以提供精細的空間分辨率和斑塊成分的定量分析,有潛力成為臨床評估動脈粥樣硬化致病風險的重要手段。當前,磁共振黑血成像技術還面臨一些挑戰:第一,磁共振黑血成像技術雖然對于頸動脈管壁成像效果較好,但是在其他動脈血管壁成像,如冠狀動脈成像方面,仍存在一定局限性[68];第二,其成像速度較慢[69],這成為該技術向臨床推廣應用的一大瓶頸。如何在短時間內獲得大范圍、高質量的、包含斑塊各成分信息的圖像,將成為磁共振血管壁成像領域未來的發展方向。
參考文獻[References]
[1]Yuan C, Kerwin WS, Yarnykh VL, et al. MRI of atherosclerosis in clinical trials. NMR Biomed, 2006, 19(6): 636-654.
[2]Edelman RR, Atkinson DJ, Silver MS, et al. Frodo pulse sequences: a new means of eliminating motion, flow, and wraparound artifacts. Radiology, 1988, 166(1): 231-236.
[3]Felmlee JP, Ehman RL. Spatial presaturation: a method for suppressing flow artifacts and improving depiction of vascular anatomy in MR imaging. Radiology, 1987, 164(2): 559-564.
[4]Edelman RR, Chien D, Kim D. Fast selective black blood MR imaging. Radiology, 1991, 181(3): 655-660.
[5]Song HK, Wright AC, Wolf RL, et al. Multislice double inversion pulse sequence for efficient black-blood MRI. Magn Reson Med, 2002, 47(3): 616-620.
[6]Yarnykh VL, Yuan C. Multislice double inversion-recovery black-blood imaging with simultaneous slice reinversion. J Magn Reson Imaging, 2003, 17(4): 478-483.
[7]Yarnykh VL, Yuan C. T1-insensitive flow suppression using quadruple inversion-recovery. Magn Reson Med, 2002, 48(5): 899-905.
[8]Koktzoglou I, Li D. Diffusion-prepared segmented steady-state free precession: application to 3D black-blood cardiovascular magnetic resonance of the thoracic aorta and carotid artery walls. J Cardiovasc Magn Reson, 2007, 9(1): 33-42.
[9]Wang J, Yarnykh VL, Hatsukami T, et al. Improved suppression of plaque-mimicking artifacts in black-blood carotid atherosclerosis imaging using a multislice motion-sensitized driven-equilibrium (MSDE) turbo spin-echo (TSE) sequence. Magn Reson Med, 2007, 58(5): 973-981.
[10]Wang J, Yarnykh VL, Yuan C. Enhanced image quality in black-blood MRI using the improved motion-sensitized drivenequilibrium (iMSDE) sequence. J Magn Reson Imaging, 2010,31(5): 1256-1263.
[11]Balu N, Yarnykh VL, Chu B, et al. Carotid plaque assessment using fast 3D isotropic resolution black-blood MRI. Magn Reson Med, 2011, 65(3): 627-637.
[12]Obara M, Kuroda K, Wang J, et al. Comparison between two types of improved motion-sensitized driven-equilibrium (iMSDE) for intracranial black-blood imaging at 3.0 tesla. J Magn Reson Imaging, 2014, 40(4): 824-831.
[13]Liu CY, Bley TA, Wieben O, et al. Flow-independent T2-prepared inversion recovery black-blood MR imaging. J Magn Reson Imaging, 2010, 31(1): 248-254.
[14]Kawaji K, Nguyen TD, Zou Z, et al. Three-dimensional flowindependent balanced steady-state free precession vessel wall MRI of the popliteal artery: preliminary experience andcomparison with flow-dependent black-blood techniques. J Magn Reson Imaging, 2011, 34(3): 696-701.
[15]Xie J, Bi X, Fan Z, et al. 3D flow-independent peripheral vessel wall imaging using T2-prepared phase-sensitive inversionrecovery steady-state free precession. J Magn Reson Imaging,2010, 32(2): 399-408.
[16]Li L, Miller KL, Jezzard P. DANTE-prepared pulse trains: a novel approach to motion-sensitized and motion-suppressed quantitative magnetic resonance imaging. Magn Reson Med,2012, 68(5): 1423-1438.
[17]Li L, Chai JT, Biasiolli L, et al. Black-blood multicontrast imaging of carotid arteries with DANTE-prepared 2D and 3D MR imaging. Radiology, 2014, 273(2): 560-569.
[18]Li L, Kong Y, Zaitsu Y, et al. Structural imaging of the cervical spinal cord with suppressed CSF signal using DANTE pulse trains. Magn Reson Med, 2015, 74(4): 971-977.
[19]Wang JN, Helle M, Zhou ZC, et al. Joint blood and cerebrospinal fluid suppression for intracranial vessel wall MRI. Magn Reson Med, 2015, 13(3): 25667
[20]Mugler JP, Brookeman JR. Three-dimensional magnetizationprepared rapid gradient-echo imaging (3D MP RAGE). Magn Reson Med, 1990, 15(1): 152-157.
[21]Moody AR, Pollock JG, O'Connor AR, et al. Lower-limb deep venous thrombosis: direct MR imaging of the thrombus. Radiology, 1998, 209(2): 349-355.
[22]Wang J, Ferguson MS, Balu N, et al. Improved carotid intraplaque hemorrhage imaging using a slab-selective phasesensitive inversion-recovery (SPI) sequence. Magn Reson Med,2010, 64(5): 1332-1340.
[23]Wang J, B?rnert P, Zhao H, et al. Simultaneous noncontrast angiography and intraplaque hemorrhage (SNAP) imaging for carotid atherosclerotic disease evaluation. Magn Reson Med,2013, 69(2): 337-345.
[24]Hennig J, Weigel M, Scheffler K. Calculation of flip angles for echo trains with predefined amplitudes with the extended phase graph (EPG)-algorithm: principles and applications to hyperecho and TRAPS sequences. Magn Reson Med, 2004,51(1): 68-80.
[25]Busse RF, Hariharan H, Vu A, et al. Fast spin echo sequences with very long echo trains: design of variable refocusing flip angle schedules and generation of clinical T2 contrast. Magn Reson Med, 2006, 55(5): 1030-1037.
[26]Park J, Mugler J, Horger W, et al. Optimized T1-weighted contrast for single-slab 3D turbo spin-echo imaging with long echo trains: application to whole-brain imaging. Magn Reson Med, 2007, 58(5): 982-992.
[27]Storey P, Atanasova IP, Lim RP, et al. Tailoring the flow sensitivity of fast spin-echo sequences for noncontrast peripheral MR angiography. Magn Reson Med, 2010, 64(4): 1098-1108.
[28]Busse RF. Flow sensitivity of CPMG sequences with variable flip refocusing and implications for CSF signal uniformity in 3D-FSE imaging. In Proceedings of the 14th Annual Meeting of ISMRM 2006, 2430.
[29]Fan Z, Zhang Z, Chung YC, et al. Carotid arterial wall MRI at 3T using 3D variable-flip-angle turbo spin-echo (TSE) with flow-sensitive dephasing (FSD). J Magn Reson Imaging, 2010,31(3): 645-654.
[30]Mihai G, Chung YC, Merchant A, et al. T1-weighted-SPACE dark blood whole body magnetic resonance angiography (DBWBMRA): initial experience. J Magn Reson Imaging, 2010,31(2): 502-509.
[31]Qiao Y, Steinman DA, Qin Q, et al. Intracranial arterial wall imaging using three-dimensional high isotropic resolution black blood MRI at 3.0 T esla. J Magn Reson Imaging, 2011, 34(1): 22-30.
[32]Qiao Y, Zeiler SR, Mirbagheri S, et al. Intracranial plaque enhancement in patients with cerebrovascular events on highspatial-resolution MR images. Radiology, 2014, 271(2): 534-542.
[33]Kerwin WS, Canton G. Advanced techniques for MRI of atherosclerotic plaque. J Magn Reson Imaging, 2009, 20(4): 217-225.
[34]Kerwin WS. Carotid artery disease and stroke: assessing risk with vessel wall MRI. ISRN Cardiol, 2012, 2012(2012): 180710.
[35]Kerwin WS, Hatsukami T, Yuan C, et al. MRI of carotid atherosclerosis. AJR Am J Roentgenol, 2013, 200(3): 304-313.
[36]Bodle JD, Feldmann E, Swartz RH, et al. High-resolution magnetic resonance imaging: an emerging tool for evaluating intracranial arterial disease. Stroke, 2013, 44(1): 287-292.
[37]Ryu CW, Kwak HS, Jahng GH, et al. High-resolution MRI of intracranial atherosclerotic disease. Neurointervention, 2014,9(1): 9-20.
[38]Xie Y, Yang Q, Xie G, et al. Improved black-blood imaging using DANTE-SPACE for simultaneous carotid and intracranial vessel wall evaluation. Magn Reson Med, 2015, 17(1): 1-2.
[39]Xu WH, Li ML, Gao S, et al. In vivo high-resolution MR imaging of symptomatic and asymptomatic middle cerebral artery atherosclerotic stenosis. Atherosclerosis, 2010, 212(2): 507-511.
[40]Li ML, Xu WH, Song L, et al. Atherosclerosis of middle cerebral artery: evaluation with high-resolution MR imaging at 3 T. Atherosclerosis, 2009, 204(2): 447-452.
[41]Fayad Z, Fuster V, Fallon J, et al. Noninvasive in vivo human coronary artery lumen and wall imaging using black-blood magnetic resonance imaging. Circulation, 2000, 102(5): 506-510.
[42]Botnar R, Stuber M, Kissinger K, et al. Noninvasive coronary vessel wall and plaque imaging with magnetic resonance imaging. Circulation, 2000, 102(21): 2582-2597.
[43]Botnar R, Kim W, Bornert P, et al. 3D coronary vessel wall imaging utilising a local inversion technique with spiral image acquisition. Magn Reson Med, 2001, 46(5): 848-854.
[44]Katoh M, Spuentrup E, Buecker A, et al. MRI of coronary vessel walls using radial k-space sampling and steady state free rpeces- sion imaging. AJR Am J Roentgenol, 2006, 186(6): s401-s406.
[45]Kim W, Stuber M, Bornert P, et al. Three-dimensional blackblood cardiac magnetic resonance coronary vessel wall imaging detects positive arterial remodeling in patients with nonsignificant coronary artery disease. Circulation, 2002, 106(3):296-299.
[46]Fernandes JL, Serrano CV Jr, Blotta MH, et al. Regression of coro- nary artery outward remodeling in patients with non-ST-segment acute coronary syndromes: a longitudinal study using noninvasive magnetic resonance imaging. Am Heart J, 2006,152(6): 1123-1132.
[47]Miao C, Chen S, Macedo R, et al. Positive remodelling of the coro- nary arteries detected by MRI in an asymptomatic population: the multi-ethnic study of atherosclerosis (MESA). J Am Coll Cardiol, 2009, 53(18): 1708-1715.
[48]Terashima M, Nguyen P, Rubin G, et al. Right coronary wall CMR in the older asymptomatic advance cohort: positive remodelling and associations with type 2 diabetes. J Cardiovasc Magn Reson, 2010, 12(1): 75-81.
[49]Kim W, Astrup S, Stuber M, et al. Subclinical coronary and aortic atherosclerosis detected by magnetic resonance imaging in type 1 diabetes with and without diabetic nephropathy. Circulation, 2007, 115(2): 228-235.
[50]Scott A, Keegan J, Mohiaddin R, et al. Noninvasive detection of coronary artery wall thickening with age in healthy subjects using high resolution MRI with beat-to-beat respiratory motion correction. J Magn Reson Imaging, 2011, 34(4): 824-830.
[51]Finn A, Nakona M, Narula J, et al. Concept of vulnerable/ unstable plaque. Arterioscler Thromb Vasc Biol, 2010, 30(7): 1282-1292.
[52]Maintz D, Ozgun M, Hoffmeier A, et al. Selective coronary plaque visualisation and differentiation by contrast-enhanced inversion prepared MRI. Eur Heart J. 2006, 27(14): 1732-1736.
[53]Kawasaki T, Koga S, Noguchi T, et al. Characterization of hyper- intense plaque with noncontrast T1-weighted cardiac magnetic resonance coronary plaque imaging: comparison with multislice computed tomography and intravascular ultrasound. JACC Cardiovasc Imaging, 2009, 2(6): 720-728.
[54]Noguchi T, Kawasaki T, Tanaka A, et al. High-intensity signals in coronary plaques on non-contrast T1-weighted magnetic resonance imaging as a novel determinant of coronary events. J Am Coll Cardiol, 2014, 63(10): 989-999.
[55]Yeon S, Sabir A, Clouse M, et al. Delayed-enhancement cardiovascular magnetic resonance coronary artery wall imaging: comparison with multi-slice computed tomography and quantitative coronary angiography. J Am Coll Cardiol, 2007,50(5): 441-447.
[56]Ibrahim T, Makowski M, Jankauskas A, et al. Serial contrastenhanced cardiac magnetic resonance imaging demonstrates regression of hyperenhancement within the coronary artery wall in patients after acute myocardial infarction. JACC Cardiovasc Imaging, 2009, 2(5): 580-588.
[57]Schneeweis C, Schnackenburg B, Stuber M, et al. Delayed contrast-enhanced MRI of the coronary artery wall in takayasu arteritis. PLoS One, 2012, 7(12): e50655.
[58]Hussain T, Fenton M, Peel SA, et al. Detection and grading of coronary allograft vasculopathy in children with contrastenhanced magnetic resonance imaging of the coronary vessel wall. Circ Cardiovasc Imaging, 2013, 6(1): 91-98.
[59]Abd-Elmoniem K, Gharib A, Pettigrew R. Coronary vessel wall 3 T MR imaging with time-resolved acquisition of phasesensitive dual inversion recovery (TRAPD) technique: initial results in patients with risk factors for coronary artery disease. Radiology, 2012, 265(3): 715-723.
[60]Abd-Elmoniem K, Weiss R, Stuber M. Phase-sensitive blackblood coronary vessel wall imaging. Magn Reson Med, 2010,63(4): 1021-1030.
[61]Fan Z, Yu W, Xie Y, et al. Multi-contrast atherosclerosis characterization (MATCH) of carotid plaque with a single 5-min scan: technical development and clinical feasibility. J Cardiovasc Magn Reson, 2014, 16(1): 53-64.
[62]Zhou Z, Li R, Zhao X, et al. Evaluation of 3D multi-contrast joint intra- and extracranial vessel wall cardiovascular magnetic resonance. J Cardiovasc Magn Reson, 2015, 17(1): 41-51.
[63]Makhijani MK, Balu N, Yamada K, et al. Accelerated 3D MERGE carotid imaging using compressed sensing with a hidden markov tree model. Magn Reson Med, 2012, 36(5): 1194-1202.
[64]Li B, Dong L, Chen B, et al. Turbo fast three-dimensional carotid artery black-blood MRI by combining three-dimensional MERGE sequence with compressed sensing. Magn Reson Med,2013, 70(5): 1347-1352.
[65]Li B, Li H, Li J, et al. Relaxation enhanced compressed sensing three-dimensional black-blood vessel wall MR imaging: preliminary studies. Magn Reson Imaging, 2015, 33(7): 932-938.
[66]Gong E, Huang F, Ying K, et al. Promise: parallel-imaging and compressed-sensing reconstruction of multicontrast imaging using sharable information. Magn Reson Med, 2015, 73(2): 523-535.
[67]Zhou Z, Wang J, Balu N, et al. STEP: self-supporting tailored kspace estimation for parallel imaging reconstruction. Magn Reson Med, 2015, 11(3): 25663.
[68]Yuan C, Zhao XH. MR imaging of vulnerable plaque: consensus and challenges. Chin J Magn Reson Imaging, 2010,1(6): 429-431.苑純, 趙錫海. 易損斑塊磁共振成像:共識與挑戰. 磁共振成像, 2010, 1(6): 429-431.
[69]Zhang ZQ, He Y, Dai QY, et al. Accuracy of MR imaging to identify the coronary artery plaque: comparison with intravascular ultrasound. Chin J Magn Reson Imaging, 2010,1(2): 94-97.張兆琪, 賀毅, 戴沁怡, 等. 磁共振黑血序列冠狀動脈管壁成像評價粥樣硬化斑塊初步研究結果:與血管內超聲對照研究. 磁共振成像, 2010, 1(2): 94-97.
Current status and progress in magnetic resonance vessel wall imaging
LI Yun-duo1, ZHOU Ze-chen1, LI Rui1*, YUAN Chun21Center for Biomedical Imaging Research, Department of Biomedical Engineering,Medical School, Tsinghua University, Beijing 100084, China
Key wordsMagnetic resonance imaging; Cardiovascular diseases; Atherosclerotic plaque
AbstractMR vessel wall imaging (MRVWI) acquires the information of vessel wall by suppressing the signal of flowing blood in lumen area. MRVWI techniques can visualize vessel wall directly and evaluate plaque vulnerability by measuring morphology and components of plaque. The main target of MRVWI techniques is to suppress the signal of the flowing blood. In this survey, we will briefly review the current status and progress in MRVWI techniques.
基金項目:北京市科學技術委員會基金項目(編號:Z131100005213001)
通訊作者:李睿,E-mail: leerui@tsinghua.edu.cn
收稿日期:2015-10-29
中圖分類號:R445.2;R543
文獻標識碼:A
DOI:10.12015/issn.1674-8034.2016.02.012
猜你喜歡
中國實用醫藥(2016年29期)2016-12-26 10:14:12
心腦血管病防治(2016年5期)2016-12-19 07:30:05
華夏醫學(2016年4期)2016-12-12 00:49:41
中國實用醫藥(2016年28期)2016-12-07 22:14:45
今日健康(2016年12期)2016-11-17 12:48:07
中國現代醫生(2016年23期)2016-11-15 03:35:37
科技視界(2016年18期)2016-11-03 20:32:54
體育時空(2016年8期)2016-10-25 20:39:04
飲食與健康·下旬刊(2016年7期)2016-05-10 12:42:54
養生保健指南(2016年4期)2016-03-22 12:16:38