肺癌合并侵襲性肺曲霉病患者生存率及死亡危險因素分析*
2016-03-16 07:12:36韓瑤劉丹梁宗安王茂筠
西部醫學 2016年1期
韓瑤 劉丹 梁宗安 王茂筠
(四川大學華西醫院呼吸與危重癥醫學科, 四川 成都 610041)
?
肺癌合并侵襲性肺曲霉病患者生存率及死亡危險因素分析*
韓瑤劉丹梁宗安王茂筠
(四川大學華西醫院呼吸與危重癥醫學科, 四川 成都 610041)
【摘要】目的探討肺癌合并侵襲性肺曲霉病(IPA)患者的生存率及死亡危險因素。方法分析2010年1月~2013年12月在華西醫院住院的108例肺癌合并侵襲性肺曲霉病患者的臨床資料,隨訪患者后續治療情況、死亡原因、死亡時間;并以確診肺癌合并IPA后12周為隨訪終點,將患者分為死亡組和存活組,比較兩組間臨床特征的差異,尋求肺癌合并侵襲性肺曲霉病患者短期內死亡的危險因素。 結果至隨訪結束,肺癌合并侵襲性肺曲霉病患者共有67人死亡;單因素分析顯示:年齡≥60歲(P=0.008)、Ⅳ期肺癌(P=0.004)、合并肺部其他感染(P=0.005)、合并器官衰竭(P=0.009)、粒缺≥Ⅲ級(P=0.032)、全身使用糖皮質激素(P=0.007)、低蛋白血癥(P=0.005)、不進行抗曲霉治療(P=0.028)是肺癌合并侵襲性肺曲霉病患者死亡的危險因素。結論肺癌合并侵襲性肺曲霉病患者的全因死亡率為62.0%,1年(52周)生存率為39.6%,中位生存期為12周。年齡≥60歲、Ⅳ期肺癌、合并肺部其他感染、合并器官衰竭、粒缺≥Ⅲ級、全身使用糖皮質激素、低蛋白血癥、不進行抗曲霉治療是肺癌合并侵襲性肺曲霉病患者死亡的危險因素。
【關鍵詞】肺癌; 侵襲性肺曲霉病; 危險因素; 生存率
Survival rate and mortality risk factors in invasive pulmonary spergillosis patients with lung cancerHAN Yao, LIU Dan, LIANG Zong’an,etal
(DepartmentofRespiratoryandCriticalCareMedicine,WestChinaHospital,SichuanUniversity,Chengdu610041,China)
【Abstract】ObjectiveThis study explored the mortality risk factors and survival rate of aspergillosis in patients with lung cancer. MethodsThis study was the retrospective cohort study, which recruited 108 lung cancer patients with invasive pulmonary aspergillosis hospitalized in West China Hospital between January 1, 2010 and December 31, 2013. The clinical data were collected to understand the general situation, treatment process, treatment reaction of the patients, and patients were followed up for the outcome of treatment, cause and date of death. The clinical characteristics of lung cancer patients complicated with invasive pulmonary aspergillosis were statistical analyzed for the survival situation, risk factors, and prognostic factors.ResultsAll-cause mortality of the lung cancer patients with invasive pulmonary aspergillosis was 62%. 1 year (52 weeks) survival rate was 39.6%, and the median survival was 12 weeks. The age of 60 years or older (P=0.008), stage IV lung cancer (P=0.004), pulmonary infection (P=0.005), the other organ failure (P=0.009), Class III or IV neutropenia (P=0.032), systemic administration of corticosteroids (P=0.007), hypoproteinemia (P=0.005), anti-fungal therapy absence (P=0.028) were the main risks of death in lung cancer patients with invasive pulmonary aspergillosis. ConclusionAll-cause mortality of the lung cancer patients with invasive pulmonary aspergillosis was 62%. 1 year (52 weeks) survival rate was 39.6%, and the median survival was 12 weeks. The age of 60 years older, stage IV lung cancer, pulmonary infection, combined with the other organ failure, Class III or IV neutropenia, systemic administration of corticosteroids, hypoproteinemia, antifungal therapy absence were the risk factors of death for lung cancer patients with invasive pulmonary aspergillosis.
【Key words】Lung cancer; Invasive pulmonary aspergillosis; Risk factors; Survival rate
肺癌是全球最常見的惡性腫瘤, 同時也是全球發病率最高的惡性腫瘤,現在我國肺癌的發病率和死亡率呈持續走高態勢,預計到2025年,我國肺癌病人將達到100萬。其中肺部感染的約占肺癌死因的20%~68.1%不等[1]。國內有文獻報道有11. 6%的惡性腫瘤患者并發醫院內真菌感染,而肺部感染占真菌感染的23.1%[2],在肺癌患者中發生肺部真菌感染率為18.7%[3],特別是曲霉感染所占比例升高明顯[4,5],在導致肺部感染的條件性致病真菌中占第1位(57%)[6]。由于肺癌及侵襲性肺曲霉病(invasive pulmonary aspergillosis,IPA)均是高病死率的疾病,治療時間長,花費高,給社會、家庭、個人均造成嚴重的負擔,本研究旨在通過單中心的住院病例回顧,了解該類患者的生存率及其死亡的危險因素,以期為臨床診治提供參考和幫助。
1對象與方法
1.1研究對象2010年1月~2013年12月,在四川大學華西醫院住院治療的肺癌合并侵襲性肺曲霉病的患者108例納入研究,其中男性79例,女性29例,年齡≥60歲者63例,<60歲45例(見表1)。
納入標準:年齡>18歲;符合2008年EORTC/MSG制訂的侵襲性肺真菌病定義標準及中國侵襲性真菌感染工作組于2013年發布的血液病/惡性腫瘤患者侵襲性真菌病的診斷標準(第四次修訂版)的確診及臨床診斷患者;脫落細胞或組織標本經病理證實為肺癌的患者;送檢標本為痰液時,應符合痰液篩選標準。
排除標準:合并血液系統疾病;器官移植史;除肺癌以外其他惡性腫瘤;除肺癌以外其他因素引起的免疫受損狀態(HIV感染,長期使用免疫抑制劑等)。
1.2研究方法收集108例患者診斷肺癌合并IPA時的基線數據,包括人口統計學資料、合并癥及實驗室指標等。以患者診斷侵襲性肺曲霉病的時間為觀察起點,病人死亡或失訪時間為觀察終點,所有患者的隨訪終止時間為2014年11月28日。采取電話隨訪,隨訪內容包括:詢問生存情況及現有治療情況,若患者已死亡,了解死亡原因和死亡時間。失訪的病例歸為截尾數據,以失訪之日為隨訪終點。
1.3統計學分析采用軟件SPSS 19.0進行統計學處理,計數資料采用例數及構成比(%)表示,比較時選用卡方檢驗或Fisher’s 精確檢驗;計量資料采用均數±標準差表示。P<0.05為差異有統計學意義。將可能引起肺癌合并侵襲性肺曲霉病患者死亡的危險因素分別進行單因素及多因素分析;將單因素分析中P<0.1的危險因素納入,進行多因素Logistic回歸分析,并采用逐步回歸方式進行檢驗。采用Kaplan-Meier分析方法,對肺癌合并侵襲性肺曲霉病患者進行生存分析,失訪病人及截止觀察終點仍存活病人均視為截尾數據,繪制生存函數曲線,預估該類患者的總體生存率及中位生存期。
2結果
2.1患者基線資料 2010年1月~2013年12月在華西醫院住院的患者中共有3791名出院診斷符合肺癌;最終有108名患者判定為存在侵襲性肺曲霉病,患病率為2.85%。患者的的基本情況,見表1。
表1108例肺癌合并侵襲性肺曲霉病患者基本情況[n(×10-2)]
Table 1Characteristics in 108 cases of IPA among patients with lung cancer
注:①部分病人2種以上合并癥
2.2患者生存率所有患者的中位隨訪時間為50周。至隨訪結束,108例肺癌合并侵襲性肺曲霉病患者共有67人死亡,全因死亡率為62.04%。共有7名患者失訪,總失訪率為6.48%。所有肺癌合并IPA患者的Kaplan-Meier生存函數曲線。肺癌合并侵襲性肺曲霉病患者的1年(52周)生存率為39.6%。中位生存期為12周,見圖1、表2。

圖1肺癌合并侵襲性肺曲霉病患者的生存函數曲線圖
Figure 1Kaplan-Meier plot of survival probability from time of diagnosis of IPA in lung cancer patients

表2 肺癌合并IPA患者生存率
2.3患者短期死亡的危險因素以確診肺癌合并IPA后12周為隨訪終點,將108名患者分為死亡組和存活組,比較兩組間臨床特征的差異,以得出肺癌合并侵襲性肺曲霉病患者短期內死亡的危險因素,見表3。
表3肺癌合并侵襲性肺曲霉病死亡的危險因素的單因素分析(12周內)
Table 3Risk factor for overall mortality in 108 cases of IPA among patients with lung cancer (12 weeks)
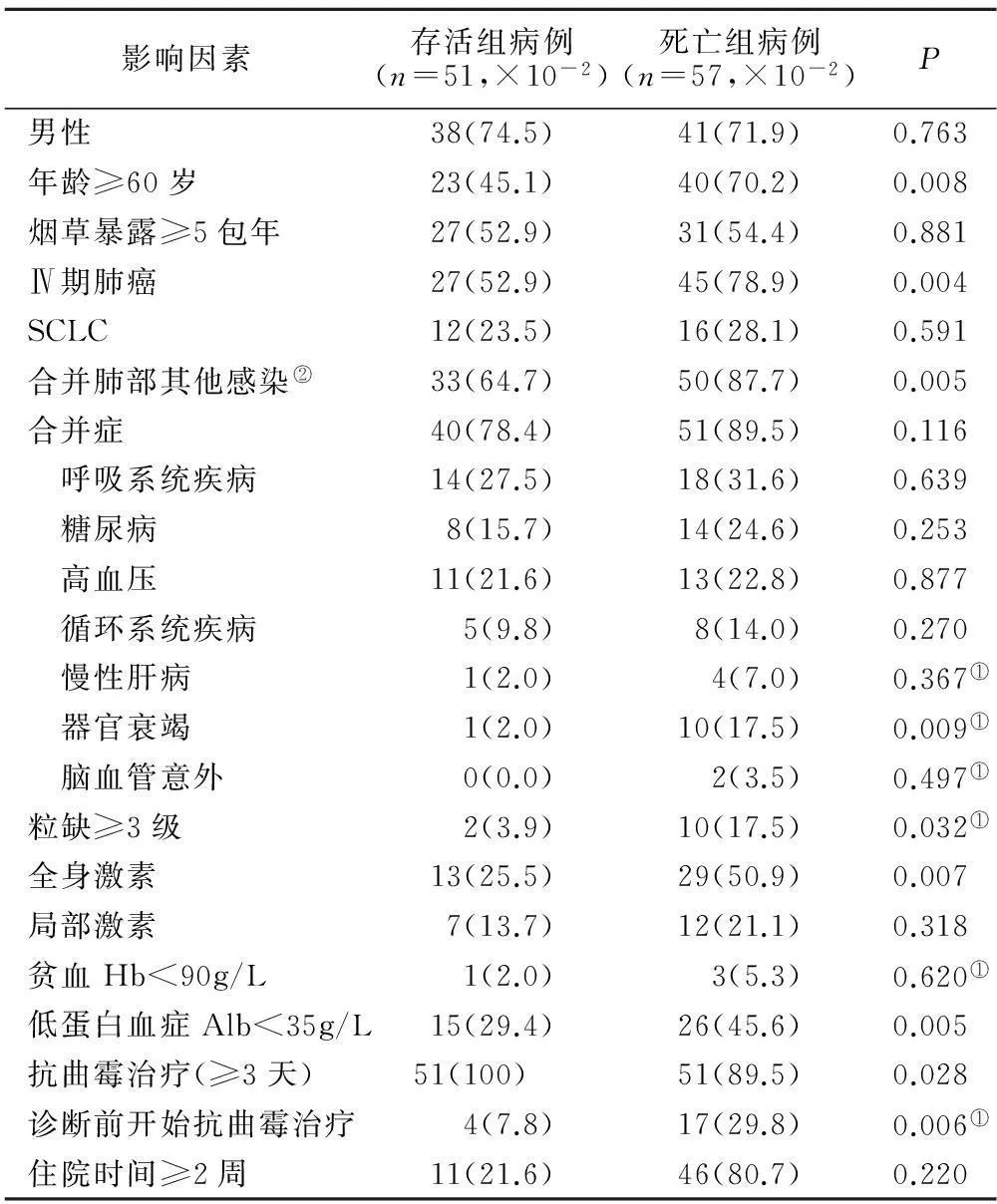
影響因素存活組病例(n=51,×10-2)死亡組病例(n=57,×10-2)P男性38(74.5)41(71.9)0.763年齡≥60歲23(45.1)40(70.2)0.008煙草暴露≥5包年27(52.9)31(54.4)0.881Ⅳ期肺癌27(52.9)45(78.9)0.004SCLC12(23.5)16(28.1)0.591合并肺部其他感染②33(64.7)50(87.7)0.005合并癥40(78.4)51(89.5)0.116 呼吸系統疾病14(27.5)18(31.6)0.639 糖尿病8(15.7)14(24.6)0.253 高血壓11(21.6)13(22.8)0.877 循環系統疾病5(9.8)8(14.0)0.270 慢性肝病1(2.0)4(7.0)0.367① 器官衰竭1(2.0)10(17.5)0.009① 腦血管意外0(0.0)2(3.5)0.497①粒缺≥3級2(3.9)10(17.5)0.032①全身激素13(25.5)29(50.9)0.007局部激素7(13.7)12(21.1)0.318貧血Hb<90g/L1(2.0)3(5.3)0.620①低蛋白血癥Alb<35g/L15(29.4)26(45.6)0.005抗曲霉治療(≥3天)51(100)51(89.5)0.028診斷前開始抗曲霉治療4(7.8)17(29.8)0.006①住院時間≥2周11(21.6)46(80.7)0.220
注:①采用Fisher檢驗;②含細菌感染、病毒感染及其他類型真菌感染
3討論
近年來,隨著器官移植的廣泛開展、免疫抑制劑和廣譜抗生素的大量應用,惡性腫瘤及HIV感染人群的增加,肺部曲霉感染的發病率呈逐年上升趨勢。在我們的研究中,從四川大學華西醫院住院患者中納入的3791名肺癌患者中滿足侵襲性肺曲霉病確診及臨床診斷的共有108名,患病率為2.85%,高于既往研究中實體腫瘤患者中IPA的患病率0.7~2.63%[7-9]。這可能與以下因素相關:①我們的研究中納入的是確診及臨床診斷患者,其中42例(38.9%)臨床診斷的患者中有34例的病原學證據來自于痰培養;而既往研究中選取的多為確診病例。②相較于既往研究中的其他部位實體腫瘤,我們選擇的是肺癌,這類患者更易合并其他肺部疾病,可能肺部的結構改變與免疫損傷更易導致侵襲性肺曲霉病感染。
在侵襲性肺曲霉病患者中,有48.3%合并血液系統惡性腫瘤,29.2%的患者接受實體器官移植,27.9%接受造血干細胞移植,22.7%合并實體腫瘤[10,11]。盡管近來伏立康唑、卡泊芬凈等藥物的使用已經改善了侵襲性肺曲霉病患者的預后,但IPA的病死率仍高達30%以上[12],Cornillet等發表的一項為期6年的單中心回顧性分析顯示其非粒缺患者病死率高達88.9%[13],這可能與非粒缺患者病情進展緩慢、起病程度較輕,容易漏診或誤診相關。Lin等[14]匯總分析了1941例侵襲性曲霉病的死亡率,其中IPA的死亡率在29.5%~60.2%之間,而肺癌合并IPA患者的死亡率在51.1%~60%,本研究中患者的全因死亡率在62.0%,接近既往文獻數據。國內文獻報道肺癌的1年生存率為37.42%~59.16%[15,16],本研究中入組的肺癌合并IPA患者的1年(52周)生存率為39.6%,中位生存期為12周,沒有觀察到與整體肺癌患者的1年生存率有明顯差異。
在本研究中以診斷12周為觀察終點,比較肺癌合并侵襲性肺曲霉病患者死亡組與存活組的臨床特征,我們發現年齡≥60歲(P=0.008)、Ⅳ期肺癌(P=0.004)、合并肺部其他感染(P=0.005)、合并器官衰竭(P=0.009)、粒缺≥Ⅲ級(P=0.032)、全身使用糖皮質激素(P=0.007)、低蛋白血癥(P=0.005)、不進行抗曲霉治療(P=0.028)是肺癌合并IPA患者死亡的危險因素。有研究表明影響侵襲性肺曲霉病預后的因素包括粒細胞缺乏癥、激素治療,年齡增長[7,17]。血清白蛋白水平被認為是一項客觀評價患者營養狀態的指標,營養不良與全身炎癥均可抑制白蛋白的合成,因此血漿白蛋白水平也可間接反映疾病的嚴重程度。研究發現,低白蛋白血癥增加患者院內死亡的風險,是醫院內感染和住院時間長短的預測因素[18,19],與該組患者的結果相似。本研究顯示Ⅳ期肺癌患者的死亡率高于其他臨床分期患者,這與Ⅳ期患者并發的其他器官轉移致多臟器功能缺陷,免疫防御下降,腫瘤負荷更大有關。在已發表的文獻資料有的認為早期抗真菌治療能改善患者預后[12,20,21],有的則沒有得出有利的結果[7,22]。該組患者抗曲霉治療藥物為伏立康唑(61例,59.8%)、卡泊芬凈(17例,16.7%)、米卡芬凈(10例,9.8%)、兩性霉素B(5例,4.9%)及伊曲康唑(9例,8.8%),新型抗真菌藥物的使用可能是導致其得出抗曲霉治療能改善患者預后的原因。
4結論
本文結果顯示,住院治療的肺癌患者中侵襲性肺曲霉病的患病率為2.85%。肺癌合并IPA患者的全因死亡率為62.0%,1年(52周)生存率為39.6%,中位生存期為12周。年齡≥60歲、Ⅳ期肺癌、合并肺部其他感染、合并器官衰竭、粒缺≥Ⅲ級、全身使用糖皮質激素、低蛋白血癥、不進行抗曲霉治療是肺癌合并IPA患者死亡的危險因素。
【參考文獻】
[1]Allemani C, Weir HK, Carreira H,etal. Global surveillance of cancer survival 1995-2009: analysis of individual data for 25,676,887 patients from 279 population-based registries in 67 countries (CONCORD-2)[J]. Lancet, 2015,385(9972):977-1010.
[2]王存德,劉坤,江波,等.惡性腫瘤患者并發醫院真菌感染的臨床分析[J].中華醫院感染學雜志,2003,13(8):730-731.
[3]楊艷榮,張志強,臧樹志. 肺癌患者肺部真菌感染臨床分析[J]. 中華醫院感染學雜志,2014(16): 115-117.
[4]Olobatoke AO, David D, Hafeez W,etal. Pulmonary carcinosarcoma initially presenting as invasive aspergillosis: a case report of previously unreported combination[J]. Diagn Pathol, 2010,5(11):1746-1749.
[5]Wu T, Li P, Wang M, Wang Q,etal. Pulmonary solid tumor with coexisting pulmonary aspergillosis: Case reports and literature review[J]. Clin Respir J, 2015,10(11):11-15.
[6]Chen KY,KoSC,HsuehPR,etal.Pulmonary Fungal Infection Emphasison Microbiological Spectra,Patient Outcome,and Prognostic Factors[J].Chest,2001,120(1):177-184.
[7]Xi Yan,Mei Li,Ming Jiang,etal. Clinical Characteristics of 45 Patients With Invasive Pulmonary Aspergillosis: Retrospective Analysis of 1711 Lung Cancer Cases[J].Cancer,2009,115(21):5018-5025.
[8]Ohmagari N, Raad II, Hachem R,etal. Invasive aspergillosis in patients with solid tumors[J]. Cancer, 2004,101(10):2300-2302.
[9]Peghin M,Ruiz-Camps I, Garcia-Vidal C,etal.Unusual forms of subacute invasive pulmonary aspergillosis in patients with solid tumors[J].J Infect, 2014,69(4):387-395.
[10] Steinbach WJ, Marr KA, Anaissie EJ,etal.Clinical epidemiology of 960 patients with invasive aspergillosis from the PATH Alliance registry[J].J Infect, 2012,65(5):453-464.
[11] Choi SH, Kang ES, EoH,etal. Aspergillus galactomannan antigen assay and invasive aspergillosis in pediatric cancer patients and hematopoietic stem cell transplant recipients[J].Pediatr Blood Cancer, 2013, 60(2):316-322.
[12] Li D, Chen L, Ding X,etal. Hospital-acquired invasive pulmonary aspergillosis in patients with hepatic failure[J]. BMC Gastroenterol, 2008,8(32):1186-1191.
[13] Garbino J, Rohner P, Kolarova L,etal. Successful treatment of pulmonary invasive aspergillosis with voriconazole in patients who failed conventional therapy[J]. Infection, 2003,31(4):241-243.
[14] Lin SJ, Schranz J, Teutsch SM. Aspergillosis case-fatality rate: systematic review of the literature[J]. Clin Infect Dis, 2001,32(3):358-366.
[15] 韓雪,喬鵬,謝夢,等. 2002-2010年上海市楊浦區居民肺癌發病與死亡分析[J].中華腫瘤雜志,2012,34(9):712-717.
[16] 凌莉,柳青,曾楚華,等.廣州市越秀區1996-1999年惡性腫瘤患者生存率分析[J].癌癥,2000,19(11):1040-1042.
[17] Upton A, Kirby KA, Carpenter P,etal. Invasive aspergillosis following hematopoietic cell transplan- tation: outcomes and prognostic factors associated with mortality[J]. Clin Infect Dis, 2007,44(4):531-540.
[18] Boston KM,BaraniukS,O’HeronS,etal.Risk factors for spinal surgical site infection,Houston,Texas[J].Infect Control Hosp Epidemiol,2009,30(9):884-889.
[19] Sacks GS,DearmanK,ReplogleWH,etal.Use of subject global assessment to idengtify nutrition-associated complcations and death in geriatric long-term care facility residents[J].J Am Coll Nutr,2000,19(5):570-577.
[20] Garbino J, Rohner P, Kolarova L,etal. Successful treatment of pulmonary invasive aspergillosis with voriconazole in patients who failed conventional therapy[J]. Infection, 2003,31(4):241-243.
[21] Rijnders BJ, Cornelissen JJ, Slobbe L,etal. Aerosolized liposomal amphotericin B for the prevention of invasive pulmonary aspergillosis during prolonged neutropenia: a randomized, placebo-controlled trial[J]. Clin Infect Dis, 2008,46(9):1401-1408.
[22] Burgos A, Zaoutis TE, Dvorak CC,etal. Pediatric invasive aspergillosis: a multicenter retrospective analysis of 139 con- temporary cases[J]. Pediatrics, 2008,121(5): 1286-1294.
(收稿日期:2015-09-01; 編輯: 陳舟貴)
通訊作者:梁宗安,教授,本刊常務編委,E-mail:liang.zongan@163.com
基金項目:國家自然科學基金(81201851);四川省科技廳科技支撐計劃項目(2014SZ0231)
【中圖分類號】R 734.2
【文獻標志碼】A
doi:10.3969/j.issn.1672-3511.2016.01.011
猜你喜歡
保健醫苑(2023年2期)2023-03-15 09:03:04
中國臨床醫學影像雜志(2022年2期)2022-05-25 13:24:34
今日健康(2016年12期)2016-11-17 14:41:50
今日健康(2016年12期)2016-11-17 13:12:34
今日健康(2016年12期)2016-11-17 12:29:29
科技資訊(2016年19期)2016-11-15 10:33:36
中國實用醫藥(2016年24期)2016-10-17 05:32:48
養生保健指南(2016年4期)2016-03-22 12:25:57
癌變·畸變·突變(2016年3期)2016-02-27 06:15:34
醫學研究雜志(2015年12期)2015-06-10 06:57:46
