Extra—gastrointestinal Stromal Tumor :Clinical Characteristics, Diagnosis, Treatment, and Prognosis
2015-11-13 08:36:45趙善峰閆丙健周巖冰
科教導(dǎo)刊 2015年28期
趙善峰 閆丙健 周巖冰
Abstract Objective:To explore the clinicopathological characteristics,treatment and prognosis of extrogastrointestinal stromal tumor (EGIST). Methods:In our study,Clinicopathological data of EGISTs from January 2010 to October 2014 were systematically investigated.Pathology results were rechecked.Patients also were followed Up.Prognostic factors were evaluated using Cox proportional hazard models and univariate and multivariate with Log-rank test. Results: An amount of ?EGISTs cases were selected due to inclusion criteria,including 28males and 26Females,with age from 18 To 78 years(median,58).Patients were follwed up.12cases were dead. The 1-,3-,5-year survival rates were 91%,75%,66%.Patients undergoing R0 resection had a better 5-year overall survival rate than those undergoing R1 resection(75%vs46%,P<0.05).For patients with high risk of recurrence after surgery, the 5-year overall survival rate was 62% and 40% respectively(P<0.05). Conclusions:Tumor size,mitotic count and tumor rupture affect the prognosis of patients after resection of primary EGISTs independently.Adjuvant imatinib can effectively improve the prognosis of the patients with high risk of recurrence, and the survival rate of patients after surgery.Surgical resection is the main treatment of EGIST, and R0 resection helps to prolong the survival time.
Key words Gastrointestinal Stromal tumors; Extra-gastrointestinal Stromal tumors; imatinib; prognosis
中圖分類號:R735.2 ? 文獻(xiàn)標(biāo)識碼:A ? DOI:10.16400/j.cnki.kjdks.2015.10.069
Introduction
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal tumors of the gastrointestinal (GI) tract.GISTs are neoplasms arising from, or differentiating along, a line similar to the gastrointestinal pacemaker cells, the interstitialcells of Cajal (ICCs).[1]GISTs may occur in the entire length of gastrointestinal tract from the esophagus to the anus; however, the most common sites are stomach (60%), small intestine (30%), rectum (5%), and esophagus (<5%) [2].Sometimes, these tumors may arise from the omentum, mesentery, and retroperitoneum, separate from the stomach and the intestine,[3-4]but similarly in histomorphology and immunophenotype; the neoplasm is defined as extra-gastrointestinal stromal tumors(EGISTs).EGISTs arising from pancreas are extremely rare, and only 20 cases have been reported in the literature from 2000 to 2013.[5-25]Here,we collected individual patient data on prognostic factors from population-based series to establish a large database.
The concept of GIST has recently been established, due to the progress in immunohistochemical analyses. It is presumed that these tumors originate from the interstitial cells of Cajal (ICCs), pacemaker cells, which are present throughout the wall of the gastrointestinal tract and which regulate the motility. ICCs share many characteristics with EGISTs, including expression of CD117 and CD34.[26]In fact, the most selective immunohistochemical markers differentiating GISTs from true smooth muscle tumors is the expression of the c-Kit receptor tyrosine kinase(CD117 antigen)in 95% of GISTs.In 2004, Yamamoto et al[27] reported that EGISTs show similar KIT mutations of typical GISTs suggesting that these tumors have a similar origin. However, at present the origin of EGISTs remains controversial.some authors believe that GISTs and EGISTs arise from the common precursor cell of ICCs and the smooth muscle cells of the gut,which may account for their growth within and outside the gastrointestinal tract.[28] Other, simpler, explanation suggests that EGISTs are in fact mural GISTs with extensive extramural growth, resulting in eventual loss of their connection with the gut wall.[29] GISTs exhibit a broad spectrum of clinical behaviors, with some low-risk lesions remaining stable for years, while others progress rapidly to widely metastatic diseases. There has been extensive study on EGIST to determine which factors predict the prognosis.A risk category assignment, which was proposed by Fletcher and has been widely accepted, has standardized prediction of the behavior of EGIST.
Methods
Procedure
In our study,We need pay attention to two points of EGISTs.The first objective was RFS, which was referred to the period of time from the date of randomization to the date of death or recurrence,with tomography(CT) or magnetic resonance imaging (MRI) of the abdomen and pelvic cavity, CT of the chest,or immunohistochemistry or gene detection,whichever occurred first;patients who were alive without recurrence were censored on the date of last follow-up. Second cancers were not considered events.The secondary objective was overall survival, defined as a period of time from the date of randomization to death reviewing patients who were alive on the date of last follow-up; and GIST-specific survival,defined as the time period from the date of randomization to the date of death considered to be caused by GIST, reviewing patients alive on the date of last follow-up and those who died from another cause on the date of death.Prognostic factors were compared by a Cox proportional hazards model.Survival between groups was compared by the log-rank test and Kaplan-Meier life-table method(P values) or unstratified Cox proportional hazards model(HRs).Frequency tables were analyzed using Fisher exact test.All analyses were done with SPSS version 16.0.
Results
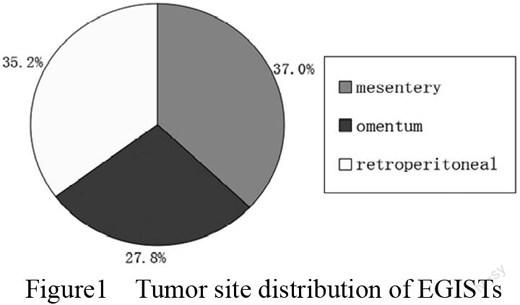
In our study,.The median age of EGISTs was 58years (range 18–78).The main symptoms: abdominal mass(24.1%,13/54), abdominal distension(33.3%,18/54), abdominal pain(42.6%,23/54).Tumor site:20cases of mesentery,15 cases of omentum, 19 cases of retroperitoneal.(Figure1)43patients underwent complete resection(R0),and 11 cases underwent incomplete resection or cytoreductive surgery(R1).Compared with R0 and R1 surgery,the overall 5 years survival rate was 75% and 46%,and the RFS was 69% and 42%,respectively(P<0.01).We used the National Institute of Health (NIH) consensus criteria (Fletchers criteria) for patient selection, with recurrence risk classification:extremely low risk of recurrence(3.7%,2/54),low risk of recurrence(16.7%,9/54),intermediate risk of recurrence(25.9%,14/54), the high risk of recurrence(53.7%,29/54). Estimated 1-year,3-year, 5-year overall survival time in the pooled series were 91%,75%,66% respectively.
Figure1 ? ?Tumor site distribution of EGISTs
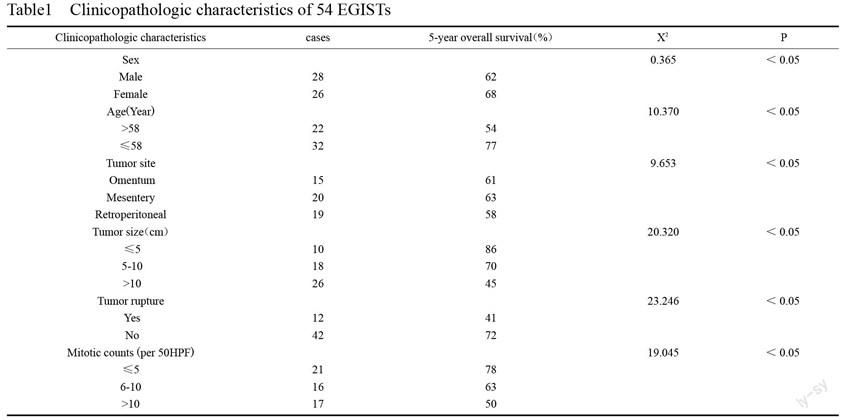
Using Single factor analysis, according to the results of EGIST, we conclude age, tumor location, tumor size, and ?tumor rupture were related to the prognosis.Multivariate analysis revealed that age,tumorsize mitotic count and tumor rupture were independent prognostic factors.(Table1)
Conclusion
Gastrointestinal stromal tumors (GIST) are the most common gastrointestinal mesenchymal tumor, and the incidence of each year is 1~2/10000.[30]GISTs tend to arise with a higher frequency in the stomach and the small bowel.[31]In fewer than 5% of cases, they originate primarily from extro-gastrointestinal tumors(EGISTs). Emory[32] has reported 67 cases of EGIST (6.7%) are located in the omentum and mesenter(80%),and in the retroperitoneal(20%)among 1004 cases of GIST. The 5-year overall survival rate is 70%.In 2560 cases of cohort study from Joensuu[33-35], report the 5-year overall survival rate is 72.3%.The clinical feature of EGISTs is variable,relying on the size and location of the tumors.The tumor may be found accidentally.The most frequent clinical symptoms are: abdominal pain,bleeding,anemia,ileus and weight loss.In our study,the patients mainly present with abdominal mass, abdominal distension, abdominal pain.The diagnosis of EGIST is based on histological, immunohistochemical,and molecular features.Microscopically,this tumor, consisted of spindle cell and epithelioid cells.Various parameters are proposed to predict the malignant potential of EGIST,such as tumor size, mitotic activity, tumor location, nonradical resection, tumor rupture, peritoneal dissemination,metastasis, and invasion into adjacent organs.
The main treatment of EGIST is relying on surgery, which ensure negative tumor edge with R0 resection.As is indicated in our study,Patients undergoing R0 resection had a better 5-year overall survival rate than those undergoing R1 resection.
Or mesenteric and omental tumor,if finding adjacent organ invasion oradhesion,operator should prevent tumor deposit or disseminate with tumor excision.For retroperitoneal EGIST, the tumor is larger and fixed,resulting in the infringement of the adjacent organs or large blood vessels around intra-abdominal, increasing the difficulty of R0 resection. For internal multiple primary EGIST,the patients undergoing R0 resection are also difficult.The extent of the tumor rupture increases the high risk of recurrence after surgery,so the prognosis is usually poor.In all,we should avoid tumor rupture in surgery; while the volume of EGIST is larger, inappropriate activity can also cause tumor spontaneous rupture, increasing the high risk of recurrence.
Imatinib has become the most effective adjuvant therapy for EGISTs.At present,not only does it use in the first-line drugs treatment of postoperative risk and high risk patients, but also it can be used for preoperative adjuvant therapy for patients so as to the effect of down staging.In this study,13 cases of EGISTs can not accepted R0 resection but imatinib adjuvant therapy(3-6 month)due to large tumor size and preoperative evaluation.For patients with high risk of recurrence after surgery,91 cases accepted imatinib adjuvant therapy.For patients with intermediate risk of recurrence after surgery,12 cases accepted imatinib adjuvant therapy.For patients with intermediate risk of recurrence between taking imatinib and not taking imatinib therapy,the 5-year overall survival rates have no obvious statistical significance.For patients with high risk of recurrence between taking imatinib and not taking imatinib therapy ,the 5-year overall survival rate was 62% and 40% respectively(P<0.05).There are still a few patients appearing the secondary resistance after a period of time, as a result increasing the dose of 400 mg/d to 600 mg/d or 1 case of EGISTs in use of Sunitinib adjuvant therapy.The only caveat about the extensive use of preoperative.the treatment or would need a higher dose of IM by performing mutational testing.If mutational testing is not available,the alternative is to assess response carefully in the firstweeks of therapy to be sure to treat patients effectively.
To sum up, age, tumor size,mitotic count and tumor rupture were independent factors affecting EGISTs after surgery.R0 resection is the first choice for the treatment of patients.Imatinib can effectively improve the prognosis of patients with high risk of recurrence.For patients with intermediate risk of recurrence after surgery,survival prognosis between taking imatinib and not taking imatinib need to be further discussed.Thus,for sustaining imatinib treatment time of the preoperative and postoperative,there is no clearly reported.In our group of pancreatic EGISTs,we need to continue to follow up and do further validation in order to observe its curative.
References
[1] Robinson TL, Sircar K, Hewlett BR, Chorneyko K, Riddel RH, Huizinga JD:Gastrointestinal stromal tumors may originate from a subset of CD34-positiva interstitial cells of Cajal. Am J Pathol 2000, 156:1157-1163.
[2] Beham AW, Scheefer IM, Schuler P, Cameron S, Ghadimi BM:Gastrointestinal stromal tumors. Int J Colorectal Dis 2012, 27:689-700.
[3] Reith JD, Goldblum GR, Lyles RH, Weiss SW: Extragastrintestinal (soft tissue) stromal tunor s: an analysis of 48 cases with emphasis on histologic predictors of outcome. Mod Pathol 2000, 13:577-585.
[4] Miettinen M, Lasota J: Gastrointestinal stromal tumors: pathology and prognosis at different sites. Semin Diagn Pathol 2006, 23:70-83
[5] Neto MR, Machuca TN, Pinho RV, Yuasa LD, Bleggi-Torres LF: Gastrointestinal stromal tumor: report of two unusual cases. Virchows Arch 2004,444:594-596.
[6] Yamura K, Kato K, Mijazawa M, Haba Y, Muramatsu A, Miyata K, Koide N:Stromal tumor of the pancreas with expression of c-kit protein: report of a case. J Gastrointestinal Hepatol 2004, 19:467-470.
[7] Krska Z, Peskov?M, Povysil C, Horejs J, Sedl郼kov?E, Kudrnov?Z: GIST of pancreas. Prague Med Rep 2005, 106:201-208.
[8] Daum O, Klecka J, Ferda J, Treska V, Vanecek T, Sima R, Mukensnabi P, Michal M: Gastrointestinal stromal tumor of the pancreas: Case report with documentation of KIT gene mutation. Virchows Arch 2005, 446:470-472.
[9] Showalter SL, Loyd JM, Glassman DT, Berger AC: Extra-intestinal stromal tumor of the pancreas: case report and a review of the literature.Arch Surg 2008, 143:305-308.
[10] Yan BM, Pai RK, Dam JV: Diagnosis of pancreatic gastrointestinal stromal ? ? tumor by EUS guided FNA. JOP 2008, 9:192-196.
[11] Yang F, Jin C, Fu D, Ni Q: Extra-gastrointestinal stromal tumor of the pancreas: ? Clinical characteristics, diagnosis, treatment, and outcome.J Surg Oncol 2011, ? ?103:739-740.