Lesson Fifty-seven Differences in negative T waves among acute coronary syndrome,acute pulmonary embolism,and Takotsubo cardiomyopathy
2014-05-16 09:22:54
心電與循環(huán)
2014年1期
●心電學(xué)英語(yǔ)
Lesson Fifty-seven Differences in negative T waves among acute coronary syndrome,acute pulmonary embolism,and Takotsubo cardiomyopathy
Negative T waves are common electrocardiographic changes in patients with non-ST-segment elevation acute coronary syndrome(ACS).In particular,negative T waves in the precordial leads suggest severe ischemia of the left ventricular anterior wall due to a critical stenosis of the left anterior descending coronary artery(LAD). However,this electrocardiographic finding is also frequently observed in patients with acute pulmonary embolism(APE),especially in those at risk for adverse outcomes.Furthermore,Takotsubo cardiomyopathy(TC)1is a recently recognized novel cardiac syndrome characterized by new electrocardiographic abnormalities (ST-segment elevation,negative T waves),elevated cardiac enzymes and transient left ventricular apical ballooning without obstructive coronary disease.
APE and TC should thus be included in the differential diagnosis of ACS in patients who have precordial negative T waves at initial presentation.Prompt differentiation among these three diseases is essential to ensure selection of an appropriate management strategy and thus improve outcomes.The 12-lead ECG is a simple,prompt,inexpensive,and most widely available initial clinical diagnostic examination.
300 consecutive patients(198 with ACS,81 with APE and 21 with TC)were admitted to coronary care unit and fulfilled the following criteria:(1)admission within 48 h after the onset of symptoms such as chest pain/discomfort,dyspnea or other ischemic symptoms; (2)no conditions precluding the evaluation of ST-segment changes on ECG(i.e.complete left or right bundle branch block,left ventricular hypertrophy,ventricular pacing or receiving drugs with potential effects on ECG); (3)no obvious past history of cardiopulmonary disease; and(4)fully assessable ECG on admission with negative T waves of at least 1.0 mm in two or more contiguous precordial leads(V1to V4).Patients with new ST-segment elevation of at least 2.0 mm in two contiguous precordial leads on admission ECG were excluded.
Patients with ACS who had an unstable pattern of symptoms,including rest,new-onset,or increasing angina were studied.The culprit lesion was defined as the lesion associated with angiographic findings suggesting local thrombus,the most severe lesion,or both, and it was confirmed to be located in the LAD.The diagnosis of APE was confirmed by pulmonary angiography,lung perfusion scintigraphy or computed tomographic scan.The patients with TC showed the following features:(1)transient hypokinesis,akinesis or dyskinesis2of the left ventricular apical segment(and midventricular segment)with regional wall-motion abnormalities extending beyond a single epicardial vascular distribution;(2)the absence of significant(>50%)obstructive coronary artery disease or angiographic evidence of acute plaque rupture;(3)new electrocardiographic abnormalities(T wave inversions);and(4)the absence of pheochromocytoma or myocarditis.
In this study,the anatomically contiguous Cabrera sequence3(Ⅲ,aVF,Ⅱ,-aVR,Ⅰand aVL)was used todisplay the limb leads.
Electrocardiographic findings on admission are presented in Table 1.APE was more frequently associated with P pulmonale,S1S2S3pattern and clockwise rotation.Right axis deviation and S1Q3T3pattern were observed in only APE.ACS was more frequently associated with ST-segment depression as well as greater summed ST-segment depression.The number and maximal amplitude of negative T waves were greatest in patients with TC,followed by those with ACS and were lowest in patients with APE.The prevalence of negative T waves in the three groups is shown in Figure 1.In the limb leads,negative T waves were frequently observed in leads I and aVL,particularly in the latter,and were rare in inferior leads and lead-aVR in patients with ACS.In contrast,the prevalence of negative T waves gradually decreased from leadsⅢto-aVR,and negative T waves were not found in leadⅠor aVL in patients with APE,whereas a high prevalence of negative T waves centered around4lead-aVR in patients with TC.In the precordial leads,the distribution of negative T waves centered around lead V3in patients with ACS. In contrast,negative T waves were consistently observed in leads V1and V2,and their prevalence gradually decreased from leads V3to V6in patients with APE, whereas a high prevalence of negative T waves was noted in precordial leads except for lead V1in patients with TC.Negative T waves in both leadsⅢand V1were present in 90%of patients with APE,but only in 3%of patients with ACS or TC.Negative T waves in lead-aVR (i.e.positive T waves in lead aVR)and no negative T waves in lead V1were observed in 95%of patients with TC in contrast to only 3%of patients with ACS or APE. Negative T waves in leadⅢwas highly predictive of APE;furthermore,the diagnostic accuracy of this finding combined with negative T waves in lead V1was very high,representing the highest predictive accuracy.Negative T waves in lead-aVR(i.e.positive T waves in lead aVR)and no negative T waves in lead V1were highly predictive of TC,but the positive predictive values of these findings were low.However,the combination of these two findings resulted in the highest ability to differentiate TC.Figure 2 shows representative ECGs for one patient from each group.
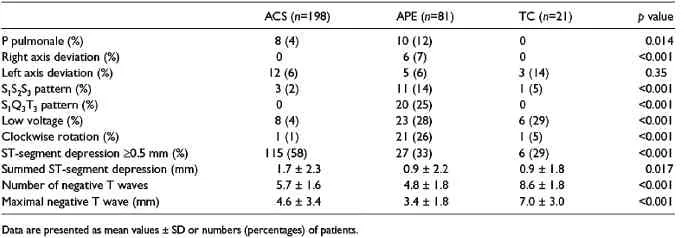
Table 1 Electrocardiographic findings
Negative T waves in ACS
In patients with ACS caused by LAD disease in this study,negative T waves were distributed primarily around leads V2to V4in the precordial leads,facing the anterior region of the left ventricle,and in lead aVL in the limb leads,facing the lateral region of the left ventricle.Negative T waves in lead V1were observed in 63%of these patients.Lead V1is considered to reflect the right paraseptal region,often supplied by the septal branch of the LAD.Negative T waves in this lead may suggest severe ischemia in the interventricular septum caused by more proximal LAD disease.In this study,the majority(75%)of patients with ACS had proximal LAD disease.Conversely,the prevalence of negative T waves in lead-aVR and inferior leads was very low.Lead -aVR(+30°)bridges the gap between5leadⅠ(0°)and leadⅡ(60°);in other words,lead-aVR faces the apical region of the left ventricle.The perfusion territory of the LAD might not extend to the inferior as well as the
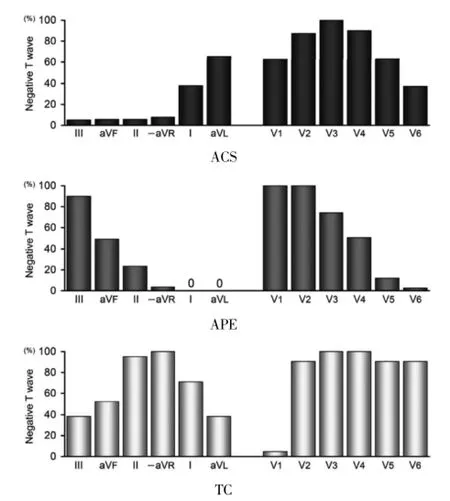
Figure 1 Prevalence of negative T waves in patients with ACS,APE and TC.apical regions of the left ventricle,resulting in less negative T waves in leads facing these regions.
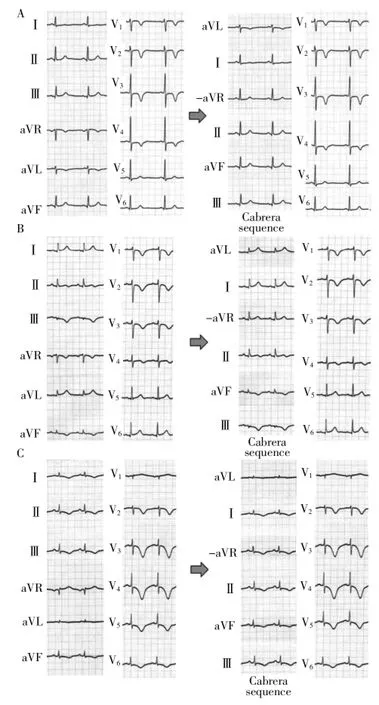
Figure2 Representative ECGs of ACS,APE and TC.A.ACS:Negative T waves were observed in leads aVL and V1to V4.When the limb leads were displayed according to the anatomically contiguous Cabrera sequence,negative T waves were seen in only lead aVL,which faces the upper lateral region of the left ventricle. Coronary angiography revealed 90%stenosis of the proximal lesion of the LAD.B.APE:Negative T waves were observed in leadsⅢ,aVF and V1to V4.When the limb leads were displayed according to the Cabrera sequence,the amplitude of negative T waves was greatest in leadⅢ,which faces the inferior region of the right ventricle,and smaller in lead aVF.T wave was slightly inverted in leadⅡ.A computed tomographic scan of the chest showed multiple filling defects in the main right and left pulmonary arteries.Lung perfusion scintigraphy revealed filling defects in the right upper,right middle and left upper lung fields.C.TC:Negative T waves were observed in leadsⅠ,Ⅱ,Ⅲ,aVF and V2to V6.In lead aVR,positive T waves were observed.When the limb leads were displayed
Negative T waves in APE
In the present study,electrocardiographic findings associated with APE,such as P pulmonale,right and left axis deviation,S1S2S3and S1Q3T3patterns,low voltage and clockwise rotation were specific,but not sensitive for APE.In the present study,negative T waves in leadsⅢ,V1and V2were very common in patients with APE. LeadⅢfaces the inferior region of the right ventricle, and leads V1and V2face the anterior region of the right ventricle.With increasing severity of right heart failure and dilation of the right ventricle towards the left owing to limited pericardial expansion,negative T waves are thought to move towards the left,i.e.from leadsⅢto aVF toⅡin the limb leads and from leads V1to V6in the precordial leads.
Negative T waves in both leadsⅢand V1could differentiate APE from ACS in patients who had precordial negative T waves.
Negative T waves in TC
Electrocardiographic changes in TC have been shown to be similar to those in anterior acute myocardialaccording to the Cabrera sequence,negative T waves were broadly distributed in all leads except for lead aVL,which faces the upper lateral region of the left ventricle. Echocardiography showed transient akinesis of the left ventricular apical and mid-ventricular segments,and coronary angiography revealed no significant coronary stenosis.
infarction.TC was associated with a greater amplitude and higher prevalence of negative T waves,as compared with ACS and APE.In addition,negative T waves were more broadly distributed around lead-aVR in the limb leads and the precordial leads except lead V1.These findings are probably ascribed to the fact that wall motion abnormalities in TC are centered around the apical region of the left ventricle faced by lead-aVR and less frequently extend to the regions faced by lead V1,i.e.the right ventricular anterior region as well as the right paraseptal region.Moreover,less negative T waves in lead V1may be attributed to another reason:TC,but not ACS caused by LAD disease or APE,is usually associated with wall motion abnormalities in the posterolateral region,resulting in negative T waves in this region.
詞匯
balloon n.&v.&adj.氣球;使鼓起,使激增,鼓起,激增;像氣球般鼓起的
preclude v.阻止,妨礙,排除
assessable adj.可評(píng)價(jià)的,可征稅的
contiguous adj.連續(xù)的,相鄰的,接觸的
scintigraphy n.閃爍掃描術(shù)
pheochromocytoma n.嗜鉻細(xì)胞瘤
注釋
1.Takotsubo cardiomyopathy指應(yīng)激性心肌病、左心室心尖球囊綜合征,其主要特征為可逆的左心室室壁運(yùn)動(dòng)異常而無(wú)冠狀動(dòng)脈的異常。
2.hypokinesis,akinesis,dyskinesis分別指運(yùn)動(dòng)低下,運(yùn)動(dòng)喪失,反向或異常運(yùn)動(dòng)。這三個(gè)詞均由kinesis(運(yùn)動(dòng))加不同的前綴構(gòu)成,類似構(gòu)成的詞有hypotonic(低張力的),atonic(無(wú)張力的),dystonic(張力異常的)。
3.Cabrera sequence又稱Cabrera format。我們目前所用心電圖額面六軸系統(tǒng)中,沒(méi)有-aVR,只有aVR(210°),而其鏡像虛構(gòu)導(dǎo)聯(lián)即為-aVR(30°),位于Ⅰ(0°)與Ⅱ(60°)正中間,使得Ⅲ、aVF、Ⅱ、-aVR、Ⅰ和aVL之間的夾角均為30°,這種順序關(guān)系即稱為Cabrera sequence或Cabrera format。-aVR的心電圖可由aVR的心電圖作一個(gè)上下翻轉(zhuǎn)獲得。-aVR作為標(biāo)準(zhǔn)導(dǎo)聯(lián)最早見(jiàn)于瑞典的相關(guān)文獻(xiàn)中。
4.center around指以…為中心,如center around human being以人為本。
5.bridges the gap between指消除…之間的隔閡,彌合…之間的差異。
參考譯文
第57課急性冠狀動(dòng)脈綜合征、肺栓塞和應(yīng)激性心肌病T波倒置的差異
T波倒置是非ST段抬高急性冠狀動(dòng)脈綜合征(ACS)常見(jiàn)的心電圖表現(xiàn)。特別是胸導(dǎo)聯(lián)T波倒置,提示左前降支(LAD)明顯狹窄導(dǎo)致的左心室前壁嚴(yán)重缺血。然而,這種心電圖變化也常見(jiàn)于急性肺栓塞(APE)患者,特別是那些有不良后果危險(xiǎn)的患者。此外,應(yīng)激性心肌病(TC)是新近發(fā)現(xiàn)的新型心臟綜合征,特征表現(xiàn)為新發(fā)的心電圖異常(ST段抬高,T波倒置),心肌酶增高,一過(guò)性左心室心尖球樣擴(kuò)張而無(wú)冠狀動(dòng)脈阻塞。
對(duì)于初始胸導(dǎo)聯(lián)T波倒置的ACS患者,APE和TC應(yīng)包含在鑒別診斷之列。對(duì)于這三種疾病,為保證選擇合適的治療方案和改善預(yù)后,快速鑒別至關(guān)重要。……
登錄APP查看全文
