Evaluation of the effect of ICCC model based comprehensive intervention with community participation initiative on diabetic blindness
2019-09-06 09:28:06RanTaoLeiGaoLeiLeiZhan2WeiYingLi3LiBao3YueSun
國際眼科雜志 2019年9期
Ran Tao, Lei Gao, Lei-Lei Zhan2, Wei-Ying Li3, Li Bao3, Yue Sun
1Baotou Medical College of Inner Mongolia University of Science & Technology, Baotou 014040, Inner Mongolia Autonomous Region, China 2National Institute of Hospital Administration, Beijing 100036, China 3Baogang Hospital of Inner Mongolia, Baotou 014040, Inner Mongolia Autonomous Region, China
Abstract
?KEYWORDS:diabetic eye care; intervention strategy; effect evaluation
INTRODUCTION
Diabetes mellitus (DM) is a chronic and intractable lifelong disease. As one of the complications of DM, diabetic retinopathy (DR) has become one of the main reasons causing blindness and posed heavy economic burden on patients’ families and society as well. Regular eye examinations have been recommended to insure early detection and treatment of DR, at the time when laser photocoagulation therapy is most effective for preserving sight[1].The risk of vision loss and blindness is proven to be reduced with regular examinations, early detection and appropriate laser treatment by some 90%[2]. Despite that widely accepted consensus guidelines recommend annual retinal examinations for diabetic patients and given the proven benefits of early detection, many patients do not follow the guidelines due to various reasons. On average, less than 50% of diabetic patients in the United States meet these recommendations[3-5]. According to the studies in different countries, main barriers to the compliance are DM patients’ lack of perception, related knowledge toward diabetic eye care and low compliance to seek regular eye check to prevent diabetic blindness[6-10]. Educational programs can improve patients’ KAP and thus compliance to routine diabetic retinopathy screening in promoting diabetic eye care with different patterns and approaches[11-16], such as BASNEF model or Procede-Proceed model. Evidence provides that CCM model oriented intervention is effective in improving the health of people who have diabetes and receive care including eye care in primary care settings[17]. This study compared the effect of community based intervention with different strategies in improving diabetic eye care, and evaluated the effect of ICCC based comprehensive intervention with community participation initiative on diabetic blindness prevention in Baotou city of Inner Mongolia Autonomous Region.
SUBJECTS AND METHODS
This was a perspective and experimental intervention study. Research population were type II diabetic patients diagnosed based on WHO standard in 1999[18]who have registered in Baogang 4thcommunity health center from October 2015 to September 2016 were enrolled in this study. Those who have mental disorders and little self-care ability in daily living were excluded. The intervention lasted for 1y from January 2017 to December 2017. All participants were informed and consented to participate the study voluntarily. DM patients were divided into two groups by random sampling. Patients in the control group received diabetic eye health education as part of conventional chronic condition management strategy, which was initiated and conducted by community health care center. The patients in the study group received eye health educational activities that were initiated, organized and conducted by community based social service organization. Both groups received baseline survey and final survey before and after different approaches of intervention.
QuestionnaireThe questionnaire was designed by ophthalmologist, general practitioner, and public health specialist after reviewing related documents. The Cronbach’s coefficient was 0.909. By Cronbach alpha and factor analysis the questionnaire reflects high reliability and validity. Two parts were included in the questionnaire, one part is about general information, and the other part is about the patients’ awareness, perception and understanding, and behavior status towards diabetic blindness prevention, which includes 3 dimensions with 35 items of questions. Among them there were 20 questions regarding diabetic blindness prevention related knowledge, 1 point for correct answer, no score for wrong answer, and 20 points in total; 10 questions for diabetic blindness prevention beliefs by Likert scale, with the highest score of 2 points, lowest of -2 points, and 20 points in total; 10 questions for diabetic eye health related behaviors by binary scale, with 1 point for answer of yes, no score for answer of no, and 10 point in total. The questionnaire was distributed through door to door visit in community and data was collected by face to face structured interview. Baseline survey for both study and control groups was conducted by the questionnaire in January of 2017, and final survey with the same questionnaire for the same groups was conducted in December of 2017.
Intervention Strategy and Method
ControlgroupAs part of community health service, chronic disease management service including diabetic care was provided by local Community Health Center (CHC). Conventional chronic disease management approach initiated by medical organization was conducted as follows: 1) Each community team from local CHC was comprised of 1 GP, 1 nurse and 1 health care staff for children or women. There were 16 teams in charge of service for 22036 inhabitants; 2) Community team established health records for all chronic patients; 3) GP provided outpatient service, one on one consultation, and referral,e.g. diabetic eye check once diabetes was diagnosed, in CHC; 4) Community team paid home visit on yearly basis measuring blood pressure and blood sugar, communicating health information including diet, exercise, medication, and complication prevention including DR; 5) Community team made phone made phone calls to patients and appointments for them to visit back to CHC on quarterly basis, and health lectures was some time given in education room in CHC; 6) Irregular community based educational and screening activities were organized normally on the Theme Day, such as World Diabetes Day, and the theme in 2017 was lectured by expertise from higher level hospital on renal damage of diabetes.
StudygroupThis group was managed by comprehensive intervention with community participation initiative as follows: 1) Community partnership: through this project CHC collaborated with one local community health promotion NGO called Xintu as community partner. Xintu provides social service purchased by government and other foundations in community disability rehabilitation, preventing dementia and home care, and fall of elders in community; 2) There were 7455 households in the community with inhabitants of 22036. Community team members included 1 professional social worker as community manager in charge, 1 head of community activity center (CAC) responsible for the running of the CAC, 30 community health ambassadors (CHA) who were the main social service providers, 1 intern with social work or public health background, 1-2 volunteers. There were 3 such teams in this community. These CHAs were with multiple background such as ordinary people, opinion leader, retired officials, retired medical staff, chronic disease patients, DM/DR patients, family members of patients, but something in common was that they were right from local community, well trained, interested in health promotion and dedicated to help. CAC was a building provided by local government where local people can get open access to it and make use of the infrastructure and facilities to enrich their spare time. It was also a place for community members to communicate with, learn from and support each other; 3) Training: Xintu provided community team with training on social work methods and tools such as enquiry and communication skills, needs assessing technique, and how to organize community activities. As technical support CHC trained community team on the very basic knowledge of chronic diseases and behavioral factors in controlling chronic conditions and complications including diabetic blindness by making the resources of GP, public health expertise and other specialists such as endocrinologists and ophthalmologists. And guideline and tool-kits on managing diabetic health including eye health was produced; 4) Based on the patient record provided by CHC, community team conducted household visit twice a month to evaluate the progress in managing diabetes and its complications by tool-kits. Recorded needs such as requesting GP or referral; timely reminded patients for follow up on quarterly basis and eye check (at the beginning and by the end of this project with one year interval) by phone calls, and new media platform such as Wechat; 5) Reports and feedback from home visit were discussed on the meeting with GP on the following weeks of home visit, further advice will be returned to patients; 6) Regular diabetic care activities were held in local CAC 1-3 times a week. Activities were in different forms such as peer group support, diabetes club, lectures by GP, and community screening activities, and other healthy cooking contest, walking contest, and drama show experiencing the experience of blindnessetc. CHA called for participation of diabetes patients, and the head of CAC responsible for preparing and organizing each activity; 7) Health information was communicated and updated by social media including new media platform; 8) Community team organized “Theme Day” activity such as on “International eye care day” “International diabetes day”, “project kick off meeting or workshop” by inviting local government officials and public to attend to increase the awareness of public and get the support of government; 9) Newsletters were delivered to local health bureau on quarterly basis to inform the performance and achievements of community health promotion efforts, which was helpful in turn to win the support of local government. The principles outlined in the Declaration of Helsinki was followed when the study was conducted in local community.
StatisticMethodEpi Data 3.1 was applied for data double entry, and SPSS 17.0 was applied for data description and analysis. Categorical data is expressed by frequency (N) and constituent rate (%), and the difference is compared within and between groups byχ2test. Numerical data is expressed by mean±SD, and the difference is compared by matched pairt-test and independent samplet-test. Multiple linear regression analysis was applied in analyzing influencing factors of KAP.Pvalue of <0.05 was considered statistically significant.
RESULTS
GeneralInformationStudy population 470 cases of type II diabetic patients diagnosed based on WHO standard in 1999[18]who have registered in Baogang 4thcommunity health center from October 2014-September 2015 were enrolled in this study. With 235 patients in the control group, the other 235 patients in the study group. All 470 cases were investigated in baseline survey, and 424 cases were investigated in final survey in one year with 208 cases in the control group and 216 cases in study group. A total of 216 questionnaires were collected in the study group with an effective response rate of 91.9%, while 208 were collected in the control group with a response rate of 88.5%. General information of study population is shown as below, and there is no statistic difference between the study groups in characteristics (Table 1).
Table1Generalinformation(n/%)
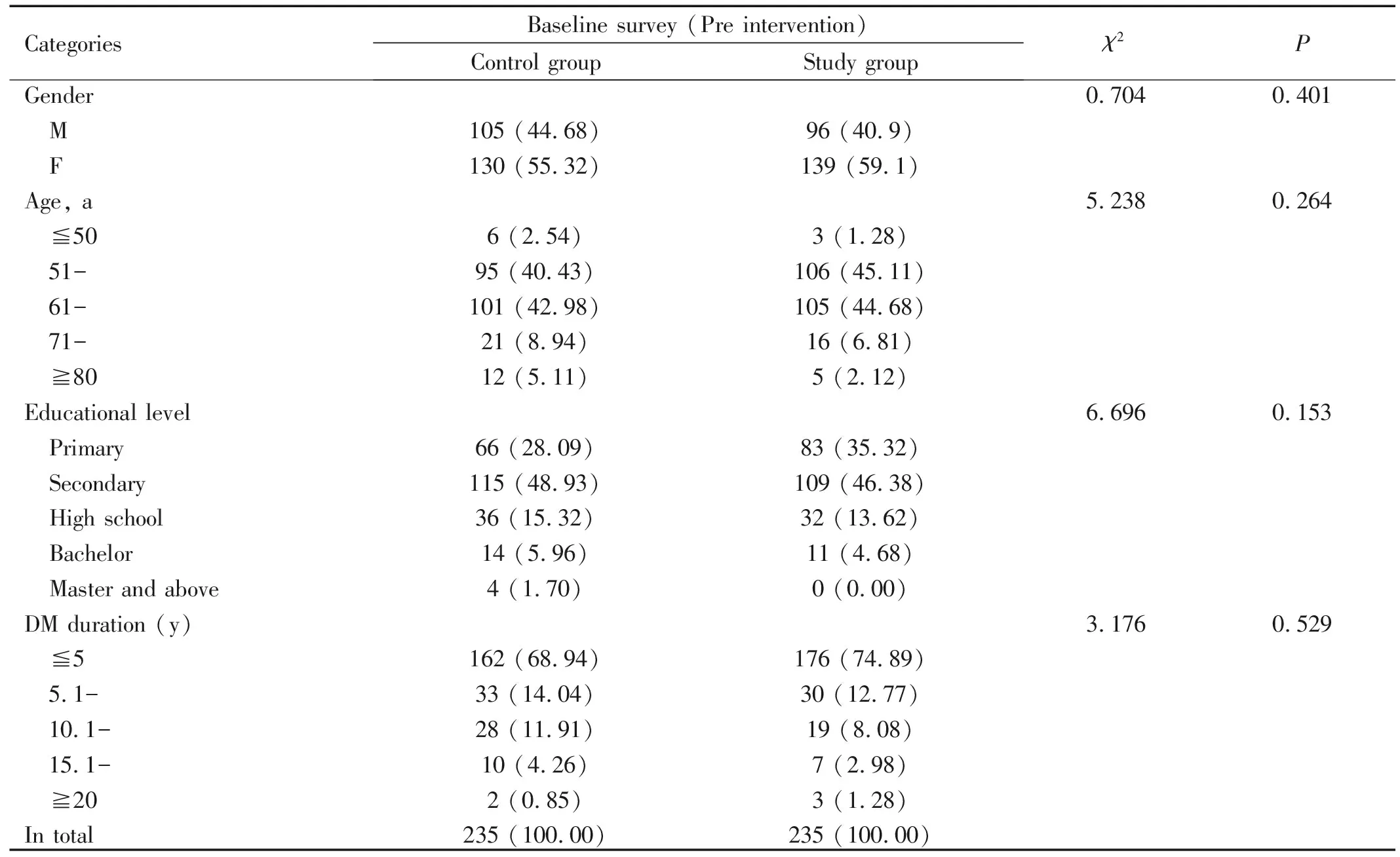
CategoriesBaseline survey (Pre intervention)Control groupStudy groupχ2PGender M FAge, a ≦50 51- 61- 71- ≧80Educational level Primary Secondary High school Bachelor Master and aboveDM duration (y) ≦5 5.1- 10.1- 15.1- ≧20In total105 (44.68)130 (55.32)6 (2.54)95 (40.43)101 (42.98)21 (8.94)12 (5.11)66 (28.09)115 (48.93)36 (15.32)14 (5.96)4 (1.70)162 (68.94)33 (14.04)28 (11.91)10 (4.26)2 (0.85)235 (100.00)96 (40.9)139 (59.1)3 (1.28)106 (45.11)105 (44.68)16 (6.81)5 (2.12)83 (35.32)109 (46.38)32 (13.62)11 (4.68)0 (0.00)176 (74.89)30 (12.77)19 (8.08)7 (2.98)3 (1.28)235 (100.00)0.7045.2386.6963.1760.4010.2640.1530.529
InformativeKnowledgeBeforeandAfterDifferentApproachesofInterventionStrategyFor control group under intervention of conventional medical organization initiative, accurate informative rate in the final survey (20.71%, 64.90%, 64.90%, 29.33%, 24.52% respectively) in the items of “Diabetes can cause irreversible blindness”, “The relation between duration of diabetes and DR”, “The relation between blood sugar and DR”, “Laser treatment won’t cause pain” and “Laser treatment is not a big surgery” were significant higher than that of baseline survey (14.04, 50.64, 47.66, 17.87, 10.64 respectively;P<0.05). There was no significant difference in other items before and after intervention. For study group under intervention of comprehensive intervention with community participation initiative accurate knowledge informative rate in the final survey in all the items were significant higher than the ones in baseline survey. There was no significant difference in accurate knowledge response for control group and study group before intervention. After intervention in the final survey the informative rate in all items in study group were significant higher than that in control group.
For control group the average score of informative knowledge in final survey (4.16±0.41) was significant higher than that in baseline survey (3.71±0.34) (t= -2.561,P=0.03). In study group the average score in final survey (10.12±1.42) was significant higher that in baseline survey (3.65±0.33) (t=-28.53,P=0.000). There was no significant difference in average score for control group and study group before intervention. After intervention the average score in study group (10.12±1.42) was significant higher than that in control group (4.16±0.41) (t= -19.7,P=0.000). (Table 2).
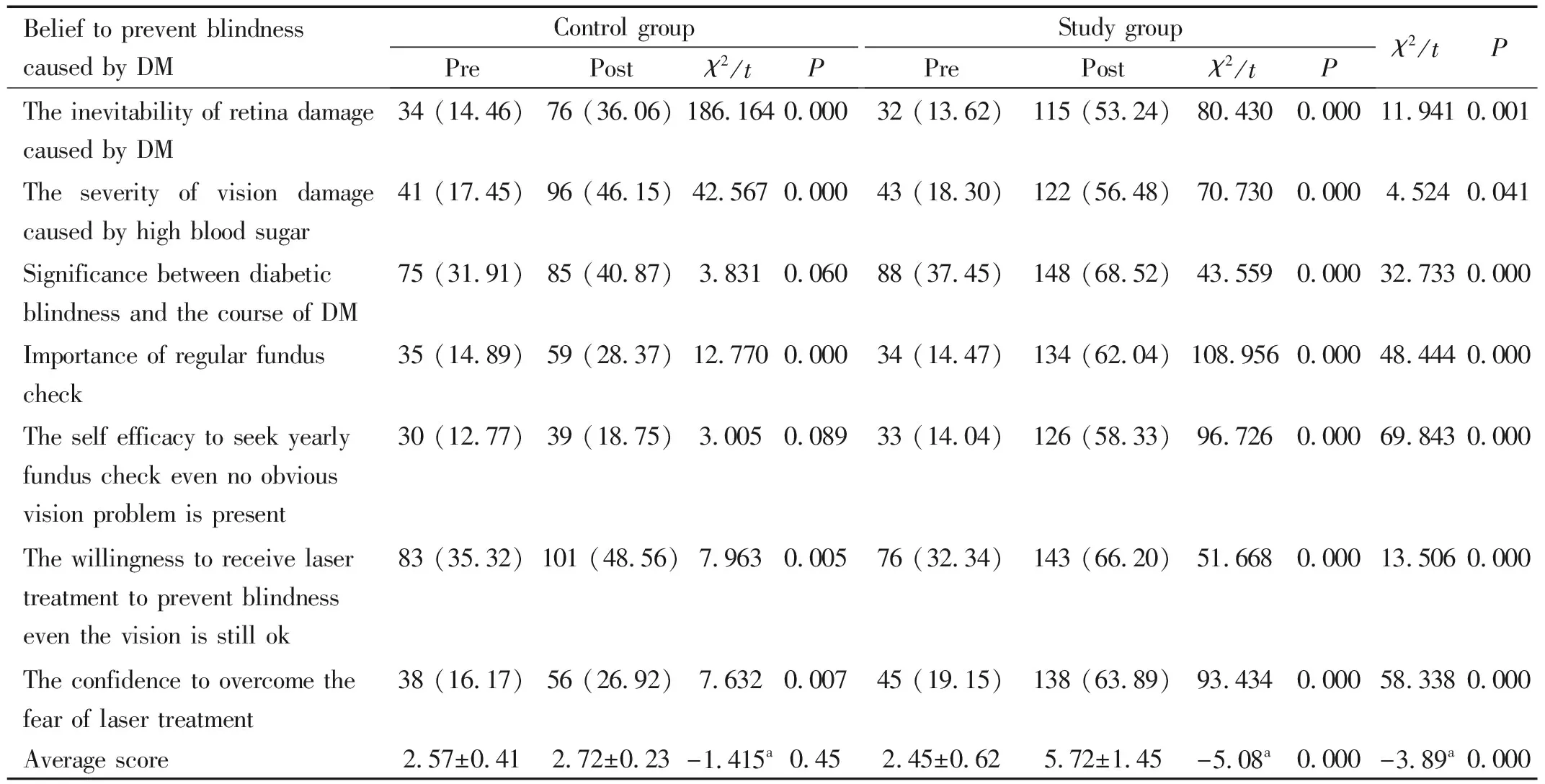
BeheldBeliefBeforeandAfterDifferentApproachesofInterventionStrategyFor control group under intervention of conventional medical organization initiative, the accurate belief rate in the final survey (36.06%, 46.15%, 28.37%, 48.56%, 26.92% respectively) in the items of “The inevitability of retina damage caused by DM”, “The severity of vision damage caused by high blood sugar”, “Importance of regular fundus check”, “The willingness to receive laser treatment to prevent blindness even the vision is still ok” and “The confidence to overcome the fear of laser treatment” were significant higher than that of baseline survey (14.46, 17.45, 14.89, 35.32, 16.17 respectively;P<0.05). There was no significant difference in other items before and after intervention. For study group under intervention of comprehensive intervention with community participation initiative the accurate belief rate in the final survey in all the items were significant higher than the ones in baseline survey. There was no significant difference in accurate belief response for control group and study group before intervention. After intervention in the final survey the accurate belief rate in all items in study group were significant higher than that in control group.
For control group there was no significant difference in the average score of accurate beheld belief in final survey comparing to that in baseline survey (t= -1.415,P=0.45). In study group the average score in final survey (5.72±1.45)
Table2Comparisonofinformativeknowledgeinpreventingdiabeticblindnesswithdifferentapproachesofmanagementstrategyn(%)was significant higher that in baseline survey (2.45±0.62) (t=-5.08,P=0.000). There was no significant difference in average score for control group and study group before intervention. After intervention the average score in study group (5.72±1.45) was significantly higher than that in control group (2.72±0.23) (t= -3.89,P=0.000) (Table 3).
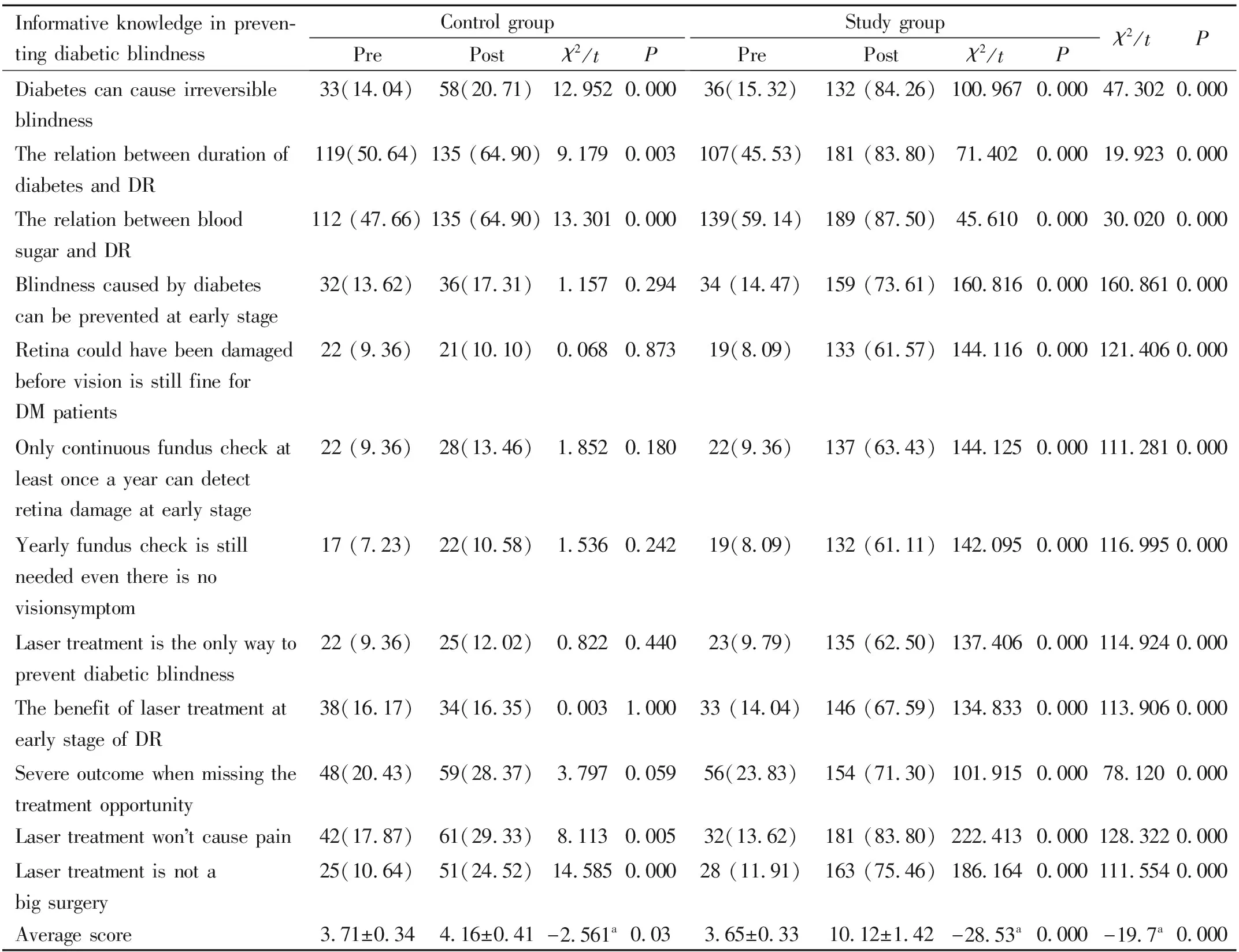
Informative knowledge in preven-ting diabetic blindnessControl groupPrePostχ2/tPStudy groupPrePostχ2/tPχ2/tPDiabetes can cause irreversible blindness33(14.04)58(20.71)12.9520.00036(15.32)132 (84.26)100.9670.00047.3020.000The relation between duration of diabetes and DR119(50.64)135 (64.90)9.1790.003107(45.53)181 (83.80)71.4020.00019.9230.000The relation between blood sugar and DR112 (47.66)135 (64.90)13.3010.000139(59.14)189 (87.50)45.6100.00030.0200.000Blindness caused by diabetes can be prevented at early stage32(13.62)36(17.31)1.1570.29434 (14.47)159 (73.61)160.8160.000160.8610.000Retina could have been damaged before vision is still fine for DM patients22 (9.36)21(10.10)0.0680.87319(8.09)133 (61.57)144.1160.000121.4060.000Only continuous fundus check at least once a year can detect retina damage at early stage22 (9.36)28(13.46)1.8520.18022(9.36)137 (63.43)144.1250.000111.2810.000Yearly fundus check is still needed even there is no visionsymptom17 (7.23)22(10.58)1.5360.24219(8.09)132 (61.11)142.0950.000116.9950.000Laser treatment is the only way to prevent diabetic blindness22 (9.36)25(12.02)0.8220.44023(9.79)135 (62.50)137.4060.000114.9240.000The benefit of laser treatment at early stage of DR38(16.17)34(16.35)0.0031.00033 (14.04)146 (67.59)134.8330.000113.9060.000Severe outcome when missing the treatment opportunity48(20.43)59(28.37)3.7970.05956(23.83)154 (71.30)101.9150.00078.1200.000Laser treatment wont cause pain42(17.87)61(29.33)8.1130.00532(13.62)181 (83.80)222.4130.000128.3220.000Laser treatment is not a big surgery25(10.64)51(24.52)14.5850.00028 (11.91)163 (75.46)186.1640.000111.5540.000Average score3.71±0.344.16±0.41-2.561a0.033.65±0.3310.12±1.42-28.53a0.000-19.7a0.000
atvalue.
ActingBehaviorBeforeandAfterDifferentApproachesofInterventionStrategyFor control group under intervention of conventional medical organization initiative, desired acting rate in the final survey (70.19%) in the items of “Adherence to doctor’s advice to take medication” was significantly higher than that of baseline survey (48.51%;P<0.05). There was no significant difference in other items before and after intervention. For study group under intervention of comprehensive intervention with community participation initiative desired acting rate in all the items were significant higher in the final survey than the ones in baseline survey. There was no significant difference in desired acting rate for control group and study group before intervention. After intervention in the final survey the desired acting rate in all items in study group were significantly higher than that in control group.
For control group there was no significant difference in the average score in desired acting behavior in final survey comparing to that in baseline survey (t= -2.65,P=0.22). In study group the average score in final survey (6.05±0.67) was significant higher that in baseline survey (4.36±0.49) (t=-29.45,P=0.000). There was no significant difference in average score for control group and study group before intervention. After intervention the average score in study group (6.05±0.67) was significantly higher than that in control group (4.41±0.73) (t=-18.78,P=0.000). (Table 4).
AssociatedFactorsInfluencingRelatedKnowledge,BeliefandActingBehaviorsinPreventingDiabeticBlindnessMultiple linear regression analysis was conducted respectively by taking group type (1=medical initiative intervention as control group, 2=community initiative intervention as study group), gender (1=male, 2=female), age (a), DM duration and educational level as independent variables, and final survey scores in related knowledge, beliefs and acting behaviors as dependent variables. The results showed that there was a positive linear regression relationship between the group type, educational level, DM duration and the level of knowledge in preventing diabetic blindness. Group type, educational level and DM duration were the influencing factors on the level of the knowledge in preventing diabetic blindness. Group type (study group with community initiative intervention strategy) influenced most on the level of the knowledge in preventing diabetic blindness. The average point in study group with community initiative intervention strategy scored 5.121 points more than that in the control group with medical initiative intervention strategy. There was a positive linear regression relationship between the group type, educational level, gender and the level of beheld beliefs in preventing diabetic blindness. Group type, educational level and gender were the influencing factors on the level of the beheld belief in preventing diabetic blindness. Group type (study group with community initiative intervention strategy) influenced most on the level of beheld beliefs in preventing diabetic blindness. The average point in study group with community initiative intervention strategy scored 2.466 points more than that in the control group with medical initiative intervention strategy. There was a positive linear regression relationship between the group type, educational level and the level of acting behaviors in preventing diabetic blindness. Group type and educational level were the influencing factors on the level of acting behaviors in preventing diabetic blindness. Group type (study group with community initiative intervention strategy) influenced most on the level of acting behaviors in preventing diabetic blindness. The average point in study group with community initiative intervention strategy scored 2.466 points more than that in the control group with medical initiative intervention strategy (Table 5).
Table3Comparisonofbeheldbeliefinpreventingdiabeticblindnesswithdifferentapproachofmanagementstrategy
n (%)
atvalue. DM: Diabetes mellitus.
Table4Comparisonofactingbehaviorinpreventingdiabeticblindnesswithdifferentapproachofmanagementstrategyn(%)

Behaviors to prevent diabetic blindnessControl groupPrePostχ2/tPStudy groupPrePostχ2/tPχ2/tPAdherence to doctors advice to take regular exercise133 (56.60)121 (58.17)0.1120.773123 (52.34)159 (73.61)21.7330.00011.2600.001Adherence to doctors advice to take diet control135 (57.45)138 (66.34)3.6950.063131 (55.74)186 (86.11)49.6960.00022.9680.000Adherence to doctors advice to take medication114 (48.51)146 (70.19)21.3940.000111 (47.23)187 (86.57)77.7070.00016.8700.000Adherence to doctors advice to take regular fundus check38 (16.17)45 (21.63)2.1640.14634 (14.47)146 (67.59)132.4480.00090.4100.000Average score4.22±0.574.41±0.73-2.65a0.224.36±0.496.05±0.67-29.45a0.000-18.78a0.000
atvalue.
DISCUSSION
As part of the chronic disease management aim to promote diabetic eye health can be achieved through educational strategies. In our study educational intervention effect of different approaches of strategy were compared and it showed that the control group with traditional medical organization initiative was effective on improving part of the accurate informative knowledge, beheld belief and acting behaviors in preventing diabetic blindness, at the same time the study group with comprehensive intervention activities with community participation initiative improved all the items of related knowledge, belief and acting behaviors. And it also indicated that study group had better performance regarding the improvement of KAP.
Table5Multiplelinearregressionanalysisoninfluencingfactorsforthelevelofrelatedknowledge,beliefsandactingbehaviorsinpreventingdiabeticblindness

VariablesBSEβtPKnowledge Constant8.1410.5320.00019.2350.000 Group type5.1210.4800.31419.7560.000 Educational level1.2680.1320.2335.3610.000DM duration (y)0.6990.2210.1163.4370.017Beliefs Constant4.8900.2120.0003.630.001 Group type2.4660.1170.3343.8910.000 Gender0.5340.1530.0891.0370.042 Educational level1.0660.1870.2672.0840.005Acting behaviors Constant5.3440.4760.0008.9870.000 Group type1.350.1050.37518.7820.000 Educational level0.7890.1350.1473.5460.000
B:Regression coefficient; SE: Standard error;β: Standardized regression coefficient; DM Diabetes mellitus.
It is important and essential that educational strategy to help and facilitate the patients and families for effective management[19]in terms of uptaking the behavior of yearly fundus check through effective communication to improve the knowledge and perception in diabetic eye care. But effective management needs time, methods and techniques to reach out patients and communication closely and deeply with patients and public. And in general the staff in charge of chronic disease management are mainly clinical expertise, who are very busy with their clinical work and have very little time nor social work methodology to work on patients and convince patients to adopt expected behavior. Our study based on ICCC framework (Figure 1) rethinks the role of community empowerment and redesign[20-21]the chronic management approach in diabetic blindness prevention by strengthening the role of community partner, who plays an important role in reaching out targeting population, assessing their needs and barriers in preventing diabetic blindness in the first place, mobilising community participation in raising awareness of the society on diabetic eye care, communicating diabetic eye care information through multiple channels and uptaking regular diabetic retinopathy screening. Comparing to costly (valuable in time and service) medical team who is good at clinical service, the advantage of community initiative approach is to make full use of community resources who are good at social work methodology such as communicating skills and organizing community activities, together with the support of medical team of health organization, the management effect can be more cost effective. This comprehensive approach emphasizes mobilization of multiple resources including social, medical and governmental, has shown effectiveness in educating diabetic patients and preventing diabetic blindness.
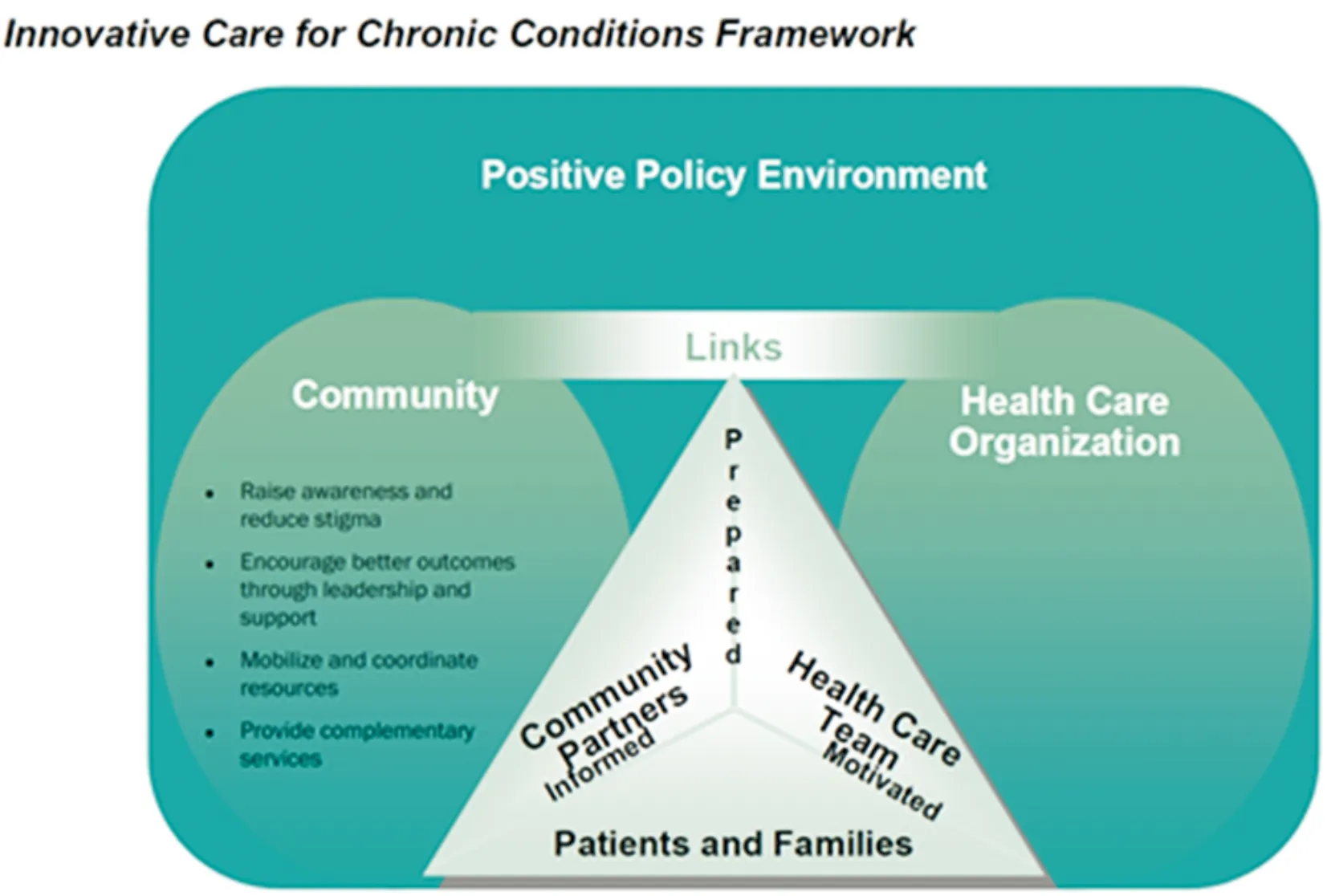
Figure1ICCCmodel.
More and more study and practice have been adopted for the exploration of innovation in chronic disease management[22-23]. In China chronic conditions including complications have been under management but it is still at early phase especially with regards to the application of evidence based guidelines and there is still lots of room for improvement[24]. Some internationally promoted chronic condition management theories and models have not been studied, applied or evaluated. In our study more research is needed to observe the impact of the strategy in the long run such as remaining vision function of DM patients. Additional research efforts should be also considered to study the cooperation mechanism among multiple sector cooperation[25]including clarifying responsibilities of related stakeholders, coordinating mechanism among all parties, cost sharing and benefit allocation mechanism for each party, thus to provide scientific evidence to policy making within the background of new medical reform in China on the basis of the research of international chronic disease management model[26].
