超低出生體質量兒支氣管肺發育不良的危險因素分析
2017-10-12 10:24:07劉兆娥
重慶醫學 2017年26期
廖 靜,劉兆娥
(1.四川省人民醫院兒科,成都 610072;2.山東大學附屬省立醫院新生兒科,濟南 250021)
論著·臨床研究
超低出生體質量兒支氣管肺發育不良的危險因素分析
廖 靜1,劉兆娥2
(1.四川省人民醫院兒科,成都 610072;2.山東大學附屬省立醫院新生兒科,濟南 250021)
目的探討超低出生體質量兒(ELBWI)支氣管肺發育不良(BPD)的危險因素。方法對2010年1月至2015年12月入住山東大學附屬省立醫院及四川省人民醫院新生兒重癥監護病房(NICU),出生后24 h內入院且存活至生后28 d以上的151例ELBWI的臨床資料進行調查分析。BPD組納入任何氧依賴[吸入氧濃度(FiO2)>21%]超過28 d的新生兒,反之為非BPD組。比較兩組間母親孕期因素、新生兒因素及疾病治療因素。結果(1)151例ELBWI,發生BPD 57例,發生率為37.7%。(2)單因素分析結果顯示,母親是否患有絨毛膜羊膜炎、胎膜早破時間、出生體質量、胎齡、敗血癥、動脈導管未閉(PDA)、新生兒呼吸窘迫綜合征(NRDS)、機械通氣(MV)、MV時間、靜脈營養時間、輸血次數與ELBWI發生BPD相關,應用咖啡因是保護因素。(3)多元Logistic回歸顯示MV(OR=6.975,95%CI:1.464~33.219),母親患有絨毛膜羊膜炎(OR=3.890,95%CI:1.656~9.140)是ELBWI發生BPD的獨立危險因素。結論盡可能減少宮內感染及早產,產后合理進行呼吸支持,可有效降低ELBWI的BPD發生率。
支氣管肺發育不良;肺疾病;危險因素;超低出生體質量兒
隨著圍產醫學的發展,產前糖皮質激素、肺泡表面活性物質(pulmonary surfactant,PS)的應用及肺保護性通氣策略的實施,超低出生體質量兒(extremely low birth weight infant,ELBWI)存活率明顯增加,但支氣管肺發育不良(bronchopulmonary dysplasia,BPD)的發生率卻有升高趨勢,嚴重威脅患兒存活及預后。目前對于早產兒發生BPD的危險因素研究較多,但針對ELBWI這個特殊群體的研究尚未見報道。本研究通過回顧性研究方法,對ELBWI發生BPD的危險因素進行探討,為綜合防治BPD提供依據。
1 資料與方法
1.1一般資料 選取2010年1月至2015年12月山東大學附屬省立醫院及四川省人民醫院新生兒重癥監護病房(NICU)住院ELBWI(出生體質量小于1 000 g)且存活至生后28 d以上者151例。排除標準:有遺傳代謝病;染色體異常;先天性肺發育不良;先天畸形。采用美國國家兒童健康和人類發展研究所(NICHD)制訂的BPD的診斷標準[1],BPD組納入任何氧依賴[吸入氧濃度(FiO2)>21%]超過28 d的新生兒,反之為非BPD組。若胎齡小于32周,根據校正胎齡36周或出院時需的FiO2分為:(1)輕度,未吸氧;(2)中度,FiO2<30%;(3)重度,FiO2>30%或需機械通氣(MV);若胎齡大于或等于32周,根據生后56 d或出院時需FiO2分為上述輕、中、重度。母親絨毛膜羊膜炎主要臨床表現為孕婦體溫升高(體溫大于或等于37.8 ℃),脈搏增快(大于或等于100次/分鐘),胎心率增快(≥160次/分鐘),宮底有壓痛,陰道分泌物異味,外周血白細胞計數升高(≥15×109/L或核左移)。孕婦體溫升高的同時伴有上述2個或以上的癥狀或體征可以臨床診斷為絨毛膜羊膜炎[2-3]。
1.2方法 回顧性分析ELBWI臨床資料,包括母親孕期因素:母親年齡,妊娠并發癥,分娩方式,是否多胎及試管嬰兒,產前是否使用糖皮質激素,有無胎盤早剝及胎膜早破等;新生兒因素:性別,胎齡,出生體質量,有無窒息,是否小于胎齡兒,是否存在重要疾病如新生兒呼吸窘迫綜合征(NRDS),有無呼吸暫停,是否有壞死性小腸結腸炎、敗血癥、動脈導管未閉(PDA);治療措施:咖啡因的使用,MV,MV時間,靜脈營養使用時間,輸血大于3次,治療用PS,經鼻持續氣道正壓通氣(NCPAP)/經鼻間歇正壓通氣(NIPPV)使用時間等。

2 結 果
2.1一般資料 納入研究的151例患兒中,男63例,女88例。確診BPD患兒57例,其中輕度28例,中度12例,重度17例,BPD發生率37.7%。BPD組胎齡(27.88±1.66)周,出生體質量(786.60±144.27)g;非BPD組胎齡(28.08±1.02)周,出生體質量(857.10±105.39)g。胎齡小于28周、28~<30周、30~33周的患兒的BPD發生率分別為44.64%、42.19%、21.21%。出生體質量小于750 g、750~1 000 g的患兒的BPD發生率分別為60.98%、29.09%。
2.2單因素分析 單因素分析示母親是否患有絨毛膜羊膜炎,胎膜早破時間,出生體質量,胎齡,敗血癥,PDA,NRDS,MV,MV時間,靜脈營養時間,輸血次數與ELBWI的BPD發生率相關,見表1、2。
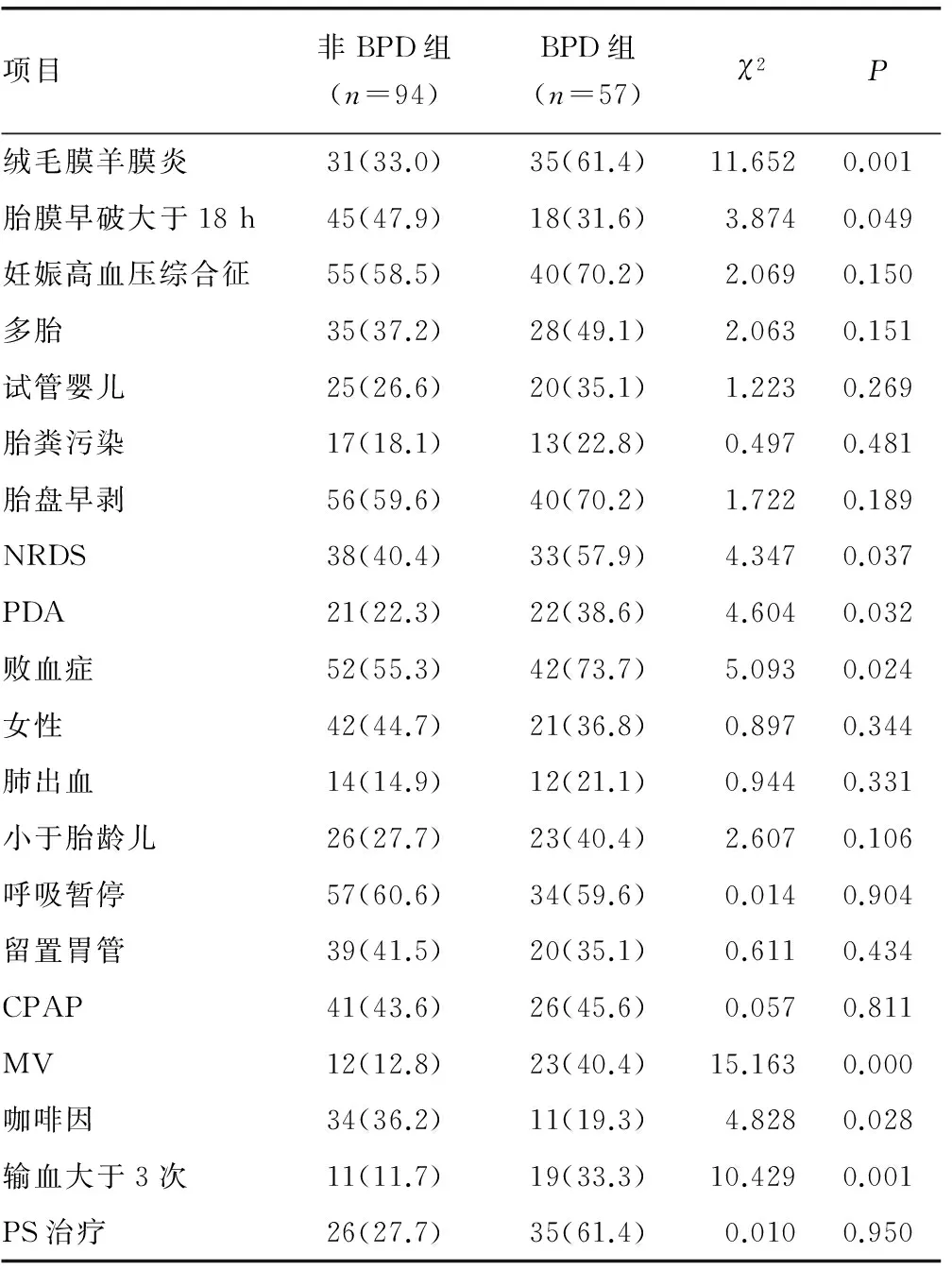
表1 兩組的ELBWI有關計數資料的單因素比較[n(%)]
2.3多因素分析 將單因素分析篩選出的有意義變量進行成組資料的多元Logistic回歸分析,共有2個變量進入最佳回歸方程,結果顯示母親患有絨毛膜羊膜炎、MV是ELBWI發生BPD的獨立危險因素,見表3。
表2 兩組的ELBWI有關計量資料的單因素比較

表3 多因素逐步Logistic回歸分析結果
3 討 論
隨著近年來ELBWI存活率升高,BPD患兒逐漸增多,存活者常遺留氣道高反應性疾病、反復呼吸道感染及喂養困難、生長發育遲緩等后遺癥。此外,嚴重BPD患兒常伴有認知損害、腦性癱瘓和神經發育損害等,嚴重影響患兒生活質量,增加家庭和社會負擔[4-5]。由于該病目前無有效治療方法,故探討BDP發生的危險因素具有重要意義。
BPD的發生率與胎齡和出生體質量有關,胎齡和出生體質量越小的早產兒BPD發生率越高[6-8]。由浙江醫科大學附屬兒童醫院牽頭的另一項多中心研究顯示,2011年部分城市ELBWI的BPD發生率為48.1%[9]。本研究中BPD發生率為37.7%,同時亦與胎齡及出生體質量呈負相關,胎齡小于28周、28~<30周、30~33周的BPD發生率分別為44.64%、42.19%、21.21%;出生體質量小于750 g、750~1 000 g BPD發生率分別為60.98%、29.09%。本研究中共有49例小于胎齡兒,其中BPD發生率為46.9%,高于適于胎齡兒BPD發生率33.3%,這與中國臺灣早產兒發育協作研究組的結果一致[10]。推測原因可能與小于胎齡兒常合并宮內感染或母親妊娠并發癥有關。
雖然目前BPD被認為是一種多因素疾病,MV仍是一個重要的危險因素[11]。MV時高氣道壓可導致肺機械性損傷,觸發炎性反應及促炎因子釋放,引起呼吸道、肺血管及間質損傷,導致BPD。本研究亦提示MV是ELBWI發生BPD的獨立危險因素。因此預防BPD發生潛在的方法就是避免MV,例如使用NCPAP及SNIPPV等無創的通氣方式[12]。研究已證實對小于28周早產兒生后即使用NCPAP的有效性和安全性,亦表明ELBWI生后即插管注入PS后拔管并予NCPAP可減少呼吸機使用[13]。亦有研究證實,對NRDS患兒不插管應用PS,避免氣管插管所致的肺損傷可進一步減少BPD的發生率[14-15]。
BPD是炎癥介導的肺損傷結果,是基因易感性患兒在易感窗期間受到宮內或出生后感染而改變肺發育的結果[16]。感染和炎性反應是 BPD 發病過程中的關鍵環節。據調查,胎齡小于28周的早產兒宮內感染和(或)炎癥發生率高達90%;體質量小于1 000 g的早產兒中1/3以上母親都有絨毛膜羊膜炎[17]。產前感染和炎癥可能使胎肺暴露于多種炎癥因子和異常生長因子中,從而擾亂肺泡分隔和血管發育過程。此外,在炎癥損傷的修復期,調控正常肺生長和修復的一些生長因子和其他物質也會影響其后的肺結構,這些都將最終導致BPD的發生[18]。本研究顯示母親患有絨毛膜羊膜炎及胎膜早破大于18 h是發生BPD的危險因素。經Logistic回歸分析提示母親患有絨毛膜羊膜炎是發生BPD的獨立危險因素,與Li等[5]研究一致。
大量研究顯示咖啡因可有效預防BPD的發生[19]。Lodha 等[20]將5 517名新生兒分為咖啡因治療組及對照組,治療組進一步分為早治療組(2 d內接受咖啡因治療)及晚治療組(3 d后接受咖啡因治療),結果顯示,早治療組可顯著降低BPD的發生,而病死率無明顯差異,說明2 d內應用咖啡因可預防BPD的發生,且安全有效。本研究顯示咖啡因是BPD發生的保護因素。因此目前推薦在極不成熟早產兒發生RDS需要進行MV時,常規應用咖啡因,以促進早期拔管撤離呼吸機并預防BPD的發生[21]。
ELBWI發生BPD的因素眾多,母親患有絨毛膜羊膜炎及MV是最危險的因素,臨床需要綜合多種防治措施才能有效控制BPD的發生及病情程度。應加強產前保健,盡可能減少宮內感染及早產,產后合理進行呼吸支持,應用肺保護性通氣策略以避免肺損傷發生,應用咖啡因可達到有效的預防效果。
[1]Jobe AH,Bancalari E.Bronchopulmonary dysplasia[J].Am J Respir Crit Care Med,2001,163(7):1723-1729.
[2]Tita AT,Andrews WW.Diagnosis and management of clinical chorioamnionitis[J].Clin Perinatol,2010,37(2):339-354.
[3]Xie A,Zhang W,Chen M,et al.Related factors and adverse neonatal outcomes in women with preterm premature rupture of membranes complicated by histologic chorioamnionitis[J].Med Sci Monit,2015,21(3):390-395.
[4]Neubauer V,Junker D,Griesmaier E,et al.Bronchopulmonary dysplasia is associated with delayed structural brain maturation in preterm infants[J].Neonatology,2015,107(3):179-184.
[5]Li Y,Cui Y,Wang C,et al.A risk factor analysis on disease severity in 47 premature infants with bronchopulmonary dysplasia[J].Intra Rare Dis Res,2015,4(2):82-86.
[6]Ruiz-Peláez JG,Charpak N.Bronchopulmonary dysplasia epidemic:incidence and associated factors in a cohort of premature infants in Bogotá,Colombia[J].Biomedica,2014,34(1):29-39.
[7]Viscardi RM.Perinatal inflammation and lung injury[J].Sem Fet Neon Med,2012,17(1):30-35.
[8]早產兒支氣管肺發育不良調查協作組.早產兒支氣管肺發育不良發生率及高危因素的多中心回顧調查分析[J].中華兒科雜志,2011,49(9):655-662.
[9]Lin HJ,Du LZ,Ma XL,et al.Mortality and morbidity of extremely low birth weight infants in the mainland of China:a multi-center study[J].Chin Med J(Engl),2015,128(20):2743-2750.
[10]Tsai LY,Chen YL,Tsou KI,et al.The impact of small-for-gestational-age on neonatal outcome among very-low-birth-weight infants[J].Pediatr Neonatol,2015,56(2):101-107.
[11]Popova AP.Mechanisms of bronchopulmonary dysplasia[J].J Cell Commun Signal,2013,7(2):119-127.
[12]Guaman MC,Gien J,Baker CD,et al.Point prevalence,clinical characteristics,and treatment variation for infants with severe bronchopulmonary dysplasia[J].Am J Perinatol,2015,32(10):960-967.
[13]Committee on Fetus and Newborn,American Academy of Pediatrics.Respiratory support in preterm infants at birth[J].Pediatrics,2014,133(1):171-174.
[14]Krajewski P,Chudzik A,Strza?ko-G?oskowska B,et al.Surfactant administration without intubation in preterm infants with respiratory distress syndrome:our experiences[J].J Matern Fetal Neonatal Med,2015,28(10):1161-1164.
[15]G?pel W,Kribs A,H?rtel C,et al.Less invasive surfactant administration is associated with improved pulmonary outcomes in spontaneously breathing preterm infants[J].Acta Paediatr,2015,104(3):241-246.
[16]常立文,李文斌.關注早產兒支氣管肺發育不良[J].中國新生兒科雜志,2011,26(1):2-4.
[17]Denney JM,Cuihane JF,Gogenberg RL.Prevention of preterm birth[J].Womens Health(Lond Engl),2008,4(6):625-638.
[18]王海霞.產前感染和炎癥與早產兒支氣管肺發育不良的關系[J].國際兒科學雜志,2012,39(4):337-341.
[19]Nobile S,Carnielli VP.Caffeine for preterm infants:current indications and uncertainties[J].Acta Biomed,2015,86 Suppl 1:S32-35.
[20]Lodha A,Seshia M,Mcmillan DD,et al.Association of early caffeine administration and neonatal outcomes in very preterm neonates[J].JAMA Pediatr,2015,169(1):33-38.
[21]Sweet DG,Carnielli V,Greisen G,et al.European consensus guidelines on the management of neonatal respiratory distress syndrome in preterm infants-2013 update[J].Neonatology,2013,103(4):353-368.
Analysisofriskfactorsforextremelylowbirthweightinfantswithbronchopulmonarydysplasia
LiaoJing1,LiuZhaoe2
(1.DepartmentofPediatrics,SichuanProvincialPeople′sHospital,Chengdu,Sichuan610072,China;2.DepartmentofNeonatology,AffiliatedProvincialHospital,ShandongUniversity,Jinan,Shandong250021,China)
ObjectiveTo explore the risk factors of extremely low birth weight infants(ELBWI) with bronchopulmonary dysplasia(BPD).MethodsThe clinical data in 151 ELBWI in NICU of the Provincial Hospital Affiliated to Shandong University and Sichuan Provincial People′s Hospital from 2010 to 2015,admitted at 24 after birth and survived until to 28 h after birth,were performed the survey analysis.The newborns of oxygen dependency(FiO2>21%) more than 28 d were included into the BPD group,on the contrary,the newborns were included into the non-BPD group.The maternal pregnant factors,neonatal factors and disease treatment factors were compared between the two groups.Results(1) Among 151 ELBWI,57 cases developed BPD with incidence rate of 37.7%.(2) The univariate analysis results showed that maternal chorioamnionitis,premature rupture of membrane more than 18 h,birth weight,gestational age,sepsis,patent ductus arteriosus(PDA),neonatal respiratory distress syndrome(NRDS),mechanical ventilation(MV),MV time,parenteral nutrition time,frequency of blood transfusion were associated with the BPD occurrence in ELBWI.Caffeine use was a protective factor.(3)The multivariate Logistic regression analysis displayed that MV(OR=6.975,95%CI:1.464-33.219) and maternal chorioamnionitis(OR=3.890,95%CI:1.656-9.140) were the independent factors of BPD occurrence in ELBWI.ConclusionReducing intrauterine infection and preterm birth as far as possible and reasonable respiratory support after birth can effectively reduce the incidence rate of BPD in ELBWI.
bronchopulmonary dysplasia;lung diseases;risk factors;extremely low birth weight infants
R722.6
A
1671-8348(2017)26-3658-03
2017-02-22
2017-06-16)
廖靜(1981-),主治醫師,碩士,主要從事兒科疾病方面研究。
10.3969/j.issn.1671-8348.2017.26.020
猜你喜歡
中學生數理化·八年級物理人教版(2021年12期)2021-12-31 03:23:08
中學生數理化·中考版(2020年10期)2020-11-27 01:59:48
家庭醫學(下半月)(2019年9期)2019-10-12 08:04:06
家庭醫學(下半月)(2019年8期)2019-09-25 09:02:00
中國生殖健康(2019年2期)2019-08-23 08:12:08
產品可靠性報告(2017年7期)2017-09-05 09:49:12
媽媽寶寶(2017年3期)2017-02-21 01:22:12
罕少疾病雜志(2016年4期)2016-03-11 16:34:39
汽車觀察(2016年3期)2016-02-28 13:16:26
中國衛生標準管理(2015年8期)2015-01-26 18:08:35
