早期年輕股骨頭壞死保髖治療常用方法及效果
2017-09-09 01:21:07劉先哲楊述華
臨床外科雜志 2017年8期
劉先哲 楊述華
·專家筆談·
早期年輕股骨頭壞死保髖治療常用方法及效果
劉先哲 楊述華
股骨頭壞死; 保髖治療; 方法
股骨頭壞死(osteonecrosis of the femoral head,ONFH)又稱缺血性壞死(avascular necrosis,AVN),是造成青壯年髖關節殘疾的最常見原因之一。病因并不明。由于生物力學作用可能引起股骨頭塌陷,因而難以治療。在股骨頭塌陷的前期采用非關節置換手術治療,對于保護關節及延緩病理進程非常重要[1-2]。尋找安全、有效、微創的方法一直是骨科研究的重要課題。保髖治療的目的是緩解疼痛、重建髖關節功能,避免或延遲行人工髖關節置換術。ONFH保髖治療的適應證是相對的,早期的ONFH 更適宜保髖治療,年輕的病人尤其是青少年更適宜保髖治療[3-8]。
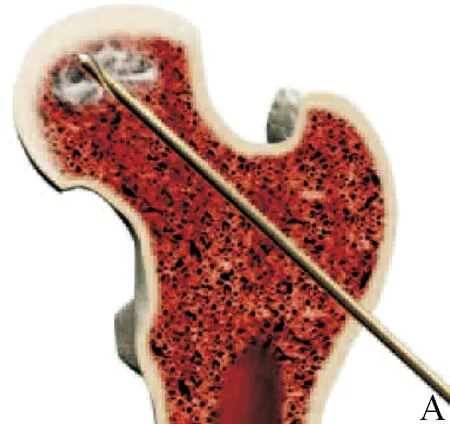
圖1 A:股骨頭髓芯減壓示意圖;B:股骨頭髓芯減壓 圖2 A:僅作髓芯減壓術;B :8個月后右側股骨頭明顯塌陷
一、股骨頭髓芯減壓
髓芯減壓術對減輕疼痛有效。透視下打入2 mm定位針確定手術位置(包括正位和側位),引入3.2 mm導針鉆入病變部位,股骨頭內多處鉆孔,操作簡單,一般能緩解疼痛,主要用于治療早期股骨頭壞死股骨頭塌陷前。但較弱的成骨能力,不能引導骨壞死的重構。組織學顯示在髓芯減壓區域有纖維肉芽組織增生,髓芯減壓術后3個月,髓芯減壓的隧道中,壞死的骨松質中充滿了纖維組織。目前,各學者對髓芯減壓的效果報道不一。髓芯減壓的原則是用10 mm規格的環鉆通過經皮穿孔減輕骨內壓。無癥狀、未塌陷、小范圍的病變可以獲得良好手術效果,但不能防止股骨頭塌陷。治療效果存在爭議(圖1)。但僅行髓芯減壓效果不佳(圖2)。
二、 髓芯減壓加骨移植
髓芯減壓加骨移植適用于Ⅰ~Ⅲ期股骨頭壞死患者。常用的人工骨誘導替代材料為添加了骨形態發生蛋白(BMP)及血小板濃縮生長因子(TGF-β,IG-F,VEG-F)的脫鈣骨基質(DBM)。使用脫鈣骨基質DBM的條件是骨頭經過脫鈣處理后生長因子才具備活性(骨形態發生蛋白是一種源于皮質骨及活性骨形成蛋白質)。合適的混合比例對于骨愈合,重構,皮質化有促進作用。有文獻報道植入上述骨材料治療早期股骨頭壞死其成功率可以達到87%(圖3)[9-13]。
三、干細胞治療
自體骨髓單個核細胞植入,應取髂骨骨髓血200 ml以上,體外分離出單個核細胞(不加培養基),單純注入或由載體植入。骨壞死的病理生理學研究發現,股骨頭壞死成骨細胞的增殖活性降低,骨髓造血間室和基質部分基質干細胞的活性降低、數量減少,可能是一種骨細胞和基質細胞相關性疾病。因此,骨髓干細胞移植可能是治療骨壞死的一種有效方法。有報道回顧性分析了116例(189髖)病人行髓芯減壓及骨髓移植術的療效。病人獲得5~11年隨訪,平均隨訪7年。提示骨髓移植對早期骨壞死的治療是有效的,但其療效及安全性還需要大規模的臨床實驗進一步驗證[14-16]。
手術期細胞培養、手術條件、手術技術等均是影響療效的重要因素。目前尚在試驗階段,謹慎采用[17-20]。
四、帶或不帶血管自體腓骨移植
吻合血管的游離腓骨術(free vascularized fibular grafting,FVFG)可改善股骨頭內循環,提供有活力的骨形成細胞,起到骨誘導和骨發生的作用。對于Steinberg Ⅰ/Ⅱ/Ⅲ期股骨頭尚未塌陷可嘗試采用。但手術較復雜且損傷大,不主張施行該手術(圖4)。
已有的研究多為不帶血管的腓骨移植術,不帶血管的腓骨獲取簡易,通過建立骨隧道,在壞死病灶清除后,腓骨可以對壞死部位提供有力的支撐,恢復其力學穩定性[21-22]。但由于腓骨無血運,與受區的相互愈合存在風險(圖5)。
五、經股骨轉子間截骨術
通過在髖部截骨,將健康的股骨頭旋轉至髖關節負重區,同時將壞死區移出負重區(圖6),但故該技術并未改變ONFH 的病理過程,其原理為將壞死區旋轉至關節前方,使正常骨作為新負重區,目的是減輕疼痛,主要用于股骨頭壞死繼發骨性關節炎病人[23-24]。

圖3 A:雙側股骨頭壞死X線片;B:雙側股骨頭壞死MRI片;C 髓芯減壓加骨移植 圖4 帶血管腓骨移植


我們使用的經股骨轉子間內翻截骨術,對于年輕病人有一定效果。見圖7。
六、多孔鉭棒植入多孔鉭棒支撐技術
該技術是在髓芯減壓和腓骨移植的基礎上發展形成的,其手術適應證為早期的股骨頭壞死。美國食品藥品管理局(FDA)于2000年6月開始評價多孔鉭假體治療早期股骨頭壞死的安全性和有效性。起初在美國境內進行臨床試驗,然后在歐洲及其他地區應用,后進入中國大陸臨床使用[25]。由于對ONFH的認識不足、對鉭棒生物功能的過度認可以及適應證的過度放大,隨著時間的推移,臨床治療失敗病例逐漸增多[25-26]。目前仍有醫生采用此方法,我們認為該方法應該淘汰(圖8)。
七、股骨頭減壓加頭下支撐
該技術為楊述華等[27-29]創新,先后采用鈦網(圖9)、同種異體骨(圖10)和有人體松質骨的成分和多級結構人工骨支撐加骨移植(圖11),可以完全成骨的新一代人工骨修復,操作簡單,效果明顯。
患側髖部墊高30°,患肢維持外展內旋位固定,常規消毒鋪巾;于大轉子下1 cm處向下作長約3 cm的外側中線縱行切口,切開外側筋膜,沿肌纖維方向鈍性分離股外側肌,暴露股骨近端外側皮質;在C臂X線機監視下將1枚導針經股骨頸鉆入到軟骨下骨的骨壞死區中央,用直徑9~13 mm的空心鉆頭沿導針鉆開股骨外側骨皮質,達到骨壞死區,采用特制的器械,經股骨頸刮除骨壞死區死骨,繼續沿導針鉆入至軟骨下骨約5 mm處,用外徑11~16 mm螺紋深1.5 mm的配套攻絲小心攻出至軟骨下骨約5 mm處;取鉆孔時收集的自體松質骨,在X線透視下用植骨器植入骨壞死區域,用植骨打壓器盡可能填塞壓實。將填塞緊密骨顆粒置于支撐架擰入攻絲好的隧道內。此方法為楊述華等為防止股骨頭塌陷而設計,此方法為壞死股骨頭軟骨下骨板提供足夠的力學支撐,生物力學支撐對負重區的軟骨下骨提供足夠的力學支撐,防止其塌陷。盡可能減少手術對股骨頭血供的破壞的微創手術。臨床隨訪結果表明,該手術用改良的髓芯減壓術減輕股骨頭骨內壓力,以增加其血供和減輕病人疼痛,同時可起到有力的持續支撐,植入骨加強其成骨過程,使骨吸收和新骨形成過程達到平衡,加強骨愈合,為關節軟骨提供足夠的力學支撐[29-31]。臨床證實有效率為95.8%,無并發癥發生。本方法創傷小,操作簡單,巧妙地解決了股骨頭內減壓同時支撐軟骨及成骨修復這一難題,是治療股骨頭壞死的新方法。




八、股骨頭壞死治療方法及方案選擇(圖12)
專家共識認為,股骨頭壞死的治療不管采用何種方法,對于塌陷前的治療,必須在修復塌陷的同時進行,防止發生新的塌陷。對于已發生塌陷的股骨頭壞死,在恢復形態的同時,要徹底修復壞死,恢復頭內、關節穩定,改善頭臼關系。因此,正確認識ONFH的發病特點,把握治療時機,合理選擇適應證,對提高保髖療效具有重要意義。

圖12 股骨頭壞死的治療方案選擇
[1] Kim SM,Lim SJ,Moon YW,et al.Cementless modular totalhiparthroplasty in patients younger than fifty with femoral head osteonecrosis:minimumfifteen-year follow-up[J].J Arthroplasty,2013,28(3):504-509.
[2] Peled E,Davis M,Axelman E,et al.Heparanase role in thetreatment of avascular necrosis of femur head[J].Thromb Res,2013,131(1):94-98.
[3] Win HL,Yang SH,Wimalaratne HK,et al.Chinese experience with metal-on-metal hip resurfacing[J].J Arthroplasty,2012,27(6):968-975.
[4] Mont MA,Jones LC,Hungerford DS.Nontraumatic osteonecrosis of the femoral head:ten years later[J].J Bone Joint Surg Am,2006,88(5):1117-1132.
[5] Beckmann J,Schmidt T,Schaumburger J,et al.Core decompression,or infusion following core decompression in thetreatment of bone edema syndrome and early avascular osteonecrosis of thefemoral head[J].Rheumatol Int,2013,33(6):1561-1565.
[6] Yang S,Wu X,Xu W.Structural augmentation with biomaterial- loaded allograft threaded cage for the treatment of femoral head osteonecrosis[J].J Arthroplasty,2010,25(8):1223-1230.
[7] Zalavras CG,Lieberman JR.Osteonecrosis of the femoral head:evaluation and treatment[J].J Am AcadOrthop Surg,2014,22(7):455-464.
[8] Rajagopal M,Balch Samora J,Ellis TJ.Efficacy of core decompression as treatment for osteonecrosis of the hip:a systematic review[J].Hip Int,2012,22(5):489-493.
[9] Martin JR,Houdek MT,Sierra RJ.Use of concentrated bone marrow aspirate and platelet rich plasma during minimally invasive decompression of the femoral head in the treatment of osteonecrosis[J].Croat Med J,2013,54(3):219-224.
[10]Sen RK,Tripathy SK,Aggarwal S,et al.Early results of core decompression and autologous bone marrow mononuclear cells instillation in femoral head osteonecrosis:a randomized control study[J].?J Arthroplasty,2012,27(5):679-686.
[11]Yamasaki T,Yasunaga Y,Ishikawa M,et al.Bone-marrow-derived mononuclear cells with a porous hydroxyapatite scaffold for the treatment of osteonecrosis of the femoral head:a preliminary study[J].J Bone Joint Surg,2010,92(3):337-341.
[12]Gangji V,De Maertelaer V,Hauzeur JP.Autologous bone marrow cell implantation in the treatment of non-traumatic osteonecrosis of the femoral head:five year follow-up of a prospective controlled study[J].Bone,2011,49(5):1005-1009.
[13]Wu XH,Yang SH,Duan DY,et al.A combination of granulocyte colony-stimulating factor and stem cell factor ameliorates steroid-associated osteonecrosis in rabbits[J].J Rheumatol,2008,35(11):2241-2248.
[14]L.Helbig,H.G.Simank,M.Kroeber.Core decompression combined with implantation of a demineralised bone matrix for non-traumatic osteonecrosis of the femoral head[J].Arch Orthop Trauma Surg,2012,132(8):1095-1103.
[15]Agarwala S,Shah S,Joshi VR.The use of alendronate in the treatment ofavascular necrosis of the femoral head:follow-up to eight years[J].J Bone Joint Surg Br,2009,91(8):1013-1018.
[16]Bednarek A,Atras A,Gaga1a J,et al.Operative technique and results of core decompression and filling with bone grafts in the treatment of osteonecrosis of the femoral head[J].Joint Bone Spine,2013,80(2):188-194.
[17]Chen C,Yang SH,Feng Y,et al.Impairment of two types of circulating endothelial progenitor cells in patients with glucocorticoidinduced avascular osteonecrosis of the femoral head[J].Joint Bone Spine,2013,80(1):70-76.
[18]Gangji V,Hauzeur JP.Treating osteonecrosis with autologous bone marrow cells[J].Skeletal Radiol,2010,39(3):209-211.
[19]Gangji V,De Maertelaer V,Hauzer JP.Autologous bone marrow cell implantation in the treatment of non-traumatic osteonecrosis of the femoral head:five year follow-up of a prospective controlled study[J].Bone,2011,49(5):1005-1009.
[20]Houdek MT,Wyles CC,Martin JR,et al.Stem cell treatment for avascularnecrosis of the femoral head:current perspectives[J].Stem Cells Cloning,2014,7:65-70.
[21]Urbaniak JR,Coogan PG,Gunneson EB,et al.Treatment of osteonecrosis of the femoral head with free vascularized fibular grafting.A long-term follow-up study of one hundred and three hips[J].J Bone Joint Surg Am,1995,77(5):681-694.
[22]楊述華.強化力學結構空心骨螺釘結合自體骨移植治療股骨頭壞死[J].中華骨科雜志,2006,26(5):313-315.
[23]Amanatullah DF,Farac R,McDonald TJ,et al.Subtrochantericfracture following removal of a porous tantalum implant[J].Case Rep Orthop,2013,2013:946745.
[24]Ha YC,Nho JH,Koo KH.Transtrochanteric rotational osteotomy for femoralhead osteonecrosis.In:Koo K-H,Mont MA,Jones LC,editors.Osteonecrosis[J].Springer,2014:325-330.
[25]Zhao D,Zhang Y,Wang W,et al.Tantalum rod implantation and vascularized iliac grafting for osteonecrosis of the femoral head[J].Orthopedics,2013,36(6):789-795.
[26]Veilette CJ,Mehdian H,Schemitsch EH,et al.Survivorship analysis and radiographic outcome following tantalum rod insertion for osteonecrosis of the femoral head[J].J Bone Joint Surg Am,2006,88(suppl 3):48-55.
[27]ShuhuaYang,Cao Yang,Baoxing Li,et al.?Strengthen the mechanical structure of the clinical treatment of femoral head necrosis[J].Spine,2006,26(5):313-316.
[28]Yang SH,Wu XH,Mei RC,et al.Biomaterial-loaded allograft threaded cage for the treatment of femoral head osteonecrosis in a goat model[J].Biotechnol Bioeng,2008,100(3):560-5664.
[29]Yang SH,Fu DH,Yang C,et al.Clinical result of structural augmentation with cannulated bone screws for the treatment of osteonecrosisof the femoral head[J].Orthop Surg,2009,1(1):42-46.
[30]Yang SH,Wu XH,Xu WH,et al.Structural augmentation with biomaterial-loaded allograft threaded cage for the treatment of femoral head osteonecrosis[J].J Arthroplasty,2010,25(8):1223-1230.
[31]楊述華,吳星火,楊操,等.異體骨籠結合脫鈣骨基質和自體骨植入治療股骨頭壞死的臨床觀察[J].中華關節外科雜志(電子版),2008,2(1):7-10.
(本文編輯:徐文聃)
10.3969/j.issn.1005-6483.2017.08.005
430022 武漢,華中科技大學同濟醫學院附屬協和醫院骨科
2017-05-08)
猜你喜歡
昆明醫科大學學報(2021年2期)2021-03-29 07:42:46
河北畫報(2020年10期)2020-11-26 07:20:50
兒童故事畫報(2019年5期)2019-05-26 14:26:14
Coco薇(2016年2期)2016-03-22 02:42:52
中國衛生標準管理(2015年3期)2016-01-14 03:41:47
Coco薇(2015年1期)2015-08-13 02:47:34
小雪花·成長指南(2015年7期)2015-08-11 15:03:12
小雪花·成長指南(2015年4期)2015-05-19 14:47:56
西南軍醫(2014年5期)2014-04-25 07:42:48
中國中醫藥現代遠程教育(2014年13期)2014-03-01 04:26:36