內鏡下組織結構分離技術在腹壁切口疝治療中的應用
2017-09-03 10:21:50任雁劉娟嚴鳳彭敏
現代儀器與醫療 2017年4期
任雁 劉娟 嚴鳳 彭敏
(成都醫學院第一附屬醫院胃腸外科,成都 610500)
內鏡下組織結構分離技術在腹壁切口疝治療中的應用
任雁 劉娟 嚴鳳 彭敏
(成都醫學院第一附屬醫院胃腸外科,成都 610500)
目的:探討腹腔鏡下組織結構分離術與傳統開放疝修補術的臨床療效差異。方法:擇期在全麻下行腹壁切口疝手術治療患者96例,隨機分為A、B組,每組各48例,A組采用傳統開放疝修補術,B組采用腹腔鏡下組織結構分離術。比較兩組患者錄患者手術時間、術中出血量、術后進食時間、住院時間、住院費用、術后復發率及并發癥發生情況。結果:兩組患者手術時間及住院費用差異沒有統計學意義(P>0.05),B組患者術中出血量、術后進食時間及住院時間較A組顯著減少,差異有統計學意義(P<0.05),B組患者術后腹壁切口疝復發率及術后并發癥較A組均顯著降低,差異有統計學意義(P<0.05)。結論:腹腔鏡下組織結構分離術與傳統開放疝修補術相比,不增加手術時間和手術費用,同時可以有效地減少術中出血量,縮短術后進食時間,降低術后住院時間、術后復發率及并發癥發生率。
腹腔鏡;組織結構分離;腹壁切口疝
腹壁切口疝是由于腹部手術后,腹壁肌腱膜層愈合不良使得腹壁薄弱、抗張力下降而引起的一種術后并發癥,發生率為2.0%~11.0%[1-2]。該疾病可導致胃腸道狹窄、黏連,甚至腸道梗阻壞死等嚴重并發癥,無法自行愈合,需要手術治療。然而傳統開放式疝修補手術具有較高的復發率[3-4]。近年來隨著腹腔鏡技術的不斷革新及相對應手術技巧的完善,腹腔鏡下組織結構分離術在腹壁切口疝手術中的運用越來越廣泛[5-6]。本研究通過比較腹腔鏡下組織結構分離術與傳統開放疝修補術的臨床療效差異,探討腹腔鏡在腹壁切口疝治療中的安全性及有效性。
1 資料與方法
1.1 一般資料
選擇2015年8月至2016年8月于我院在全麻下行腹壁切口疝手術治療的成年患者96例,隨機分為兩組,分別采用傳統開放疝修補術(A組)及腹腔鏡組織結構分離手術組(B組)。排除有嚴重心、肺疾病、嚴重肝腎功能不全、糖尿病患者或嚴重低蛋白血癥患者。本研究經我院倫理委員會批準,且所有患者均簽署知情同意書。
1.2 方法
A組采用傳統開放式疝修補術,患者平臥位,取原手術切口,切除部分癱痕后逐層分離表皮、皮下脂肪及肌肉組織,直至找到腹直肌后筋膜前間隙,依據張力大小,確定游離范圍,對術中易破的后鞘及腹膜均應修補縫合,在腹直肌后鞘前放置輕量型補片,可吸收線固定,將腹直肌及前鞘對攏縫合,關閉皮下皮膚。B組采用腹腔鏡組織結構分離手術,患者側臥位,在腋前線第11肋骨下緣與髂棘連線中點處做一切口,切開皮膚與皮下組織后顯露腹外斜肌或其腱膜,將其切開進入腹外斜肌與腹內斜肌的間隙,置入10 mm Trocar,由此Trocar注入1.6 kPa CO2建立氣腹,直視下在臍水平腋中或腋后線置入5 mm Trocar,在下腹部經已松解的腹外斜肌腱膜處再置入第3個Trocar,直視下由肛側至頭側分離腹外斜肌及腱膜,在半月線處切開,必要時可切開腹直肌后鞘,對于寬度<6 cm 的缺損無須進行補片修補,對于寬帶≥10 cm 的缺損在腹直肌后鞘前放置輕量型補片。兩組患者均由同一組經驗豐富的外科醫生施行手術,術中順利。術后患者至少避免負重4周,術后根據患者恢復情況進食流質飲食,并逐漸過渡到普通飲食。兩組患者術后常規電話隨訪6個月。
1.3 觀察指標分析
由一位不參與手術的臨床醫師負責采集數據,記錄兩組患者的手術時間、術中出血量、術后進食時間、住院時間、住院總費用、術后切口疝復發率及術后并發癥(切口感染、切口周圍皮膚缺血壞死、切口局部血腫、切口脂肪液化及術后切口疼痛)發生情況。采用SPSS19.0統計學軟件進行統計學分析。
2 結果
2.1 兩組患者一般情況比較
兩組患者一般情況(年齡、性別、體重指數、切口疝位置、切口疝面積)差異無統計學意義,P>0.05,見表1。
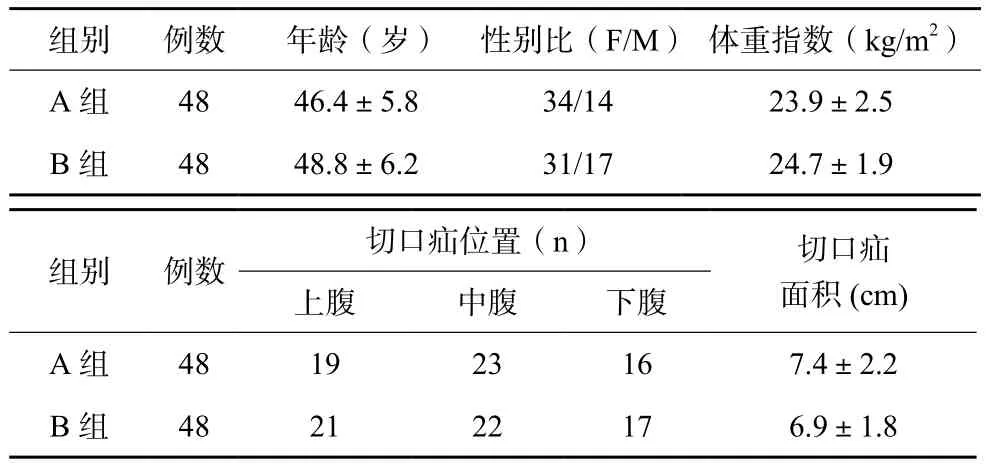
表1 三組患者一般情況比較
2.2 圍術期指標比較
B組患者的術中失血量與A組相比顯著下降,B組患者術后進食時間、住院時間及術后復發率與A組患者相比均顯著減少,差異均有統計學意義(P<0.05),見表2。
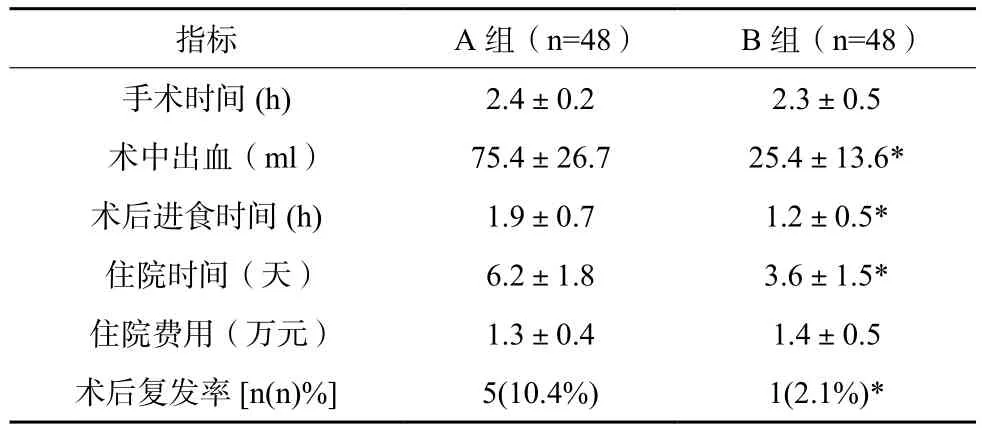
表2 兩組患者指標比較(x±s)
2.3 兩組患者術后并發癥發生情況比較
B組術后切口感染1例、切口脂肪液化1例、術后切口疼痛2例,除切開感染等并發癥外A組切口周圍皮膚缺血壞死、切口局部血腫各3例,B組術后并發癥發生率6.25%,遠低于A組的26.56%,差異有統計學意義,P<0.05。
3 討論
腹壁切口疝治療效果的優劣主要取決于手術能否夠實現真正意義上的腹壁功能重建,而如何有效地修復腹壁缺損以及重建腹壁功能一直是普外科醫師的研究熱點[7-8]。組織結構分離技術(component separation technique,CST)自上世紀90年代首次使用之后得到越來越多外科醫生的青睞,隨著腹腔鏡技術的進步與革新,腹腔鏡下組織結構分離術在腹壁切口疝手術中的運用越來越廣泛[9-11]。
本研究中傳統開放式疝修補術與腹腔鏡組織結構分離手術組的手術時間差異沒有統計學意義,腹腔鏡組織結構分離手術組患者的術中失血量與A組相比顯著下降,且差異有統計學意義。Carter[12]等研究表明腹腔鏡腹腔鏡組織結構分離手術用于腹部術后疝與傳統開放式疝修補相比會增加手術時間,與本研究結果不符,可能原因是Carter研究中納入患者種類更多,包括了術后切口疝、造瘺口旁疝、復發性斜疝、術后膈疝等,手術難度較大,會在一定程度上增加手術時間,而本研究所納入患者更為單一,均為術后切口疝,手術難度相對下降,與此同時近年來腹腔鏡技術不斷革新也在一定程度上縮短了此類手術的時間[12-14]。腹腔鏡組織結構分離手術切口較小,在手術過程中不需要廣泛分離病環周圍組織,一定程度地減少了手術過程中局部切口的滲血。表明腹腔鏡組織結構分離術在減小術中創傷及術中出血量方面與傳統開放疝修補術相比具有一定的優越性。患者術后進食時間與術后胃腸功能的恢復情況密切相關,是評價患者術后恢復情況的重要指標之一。有研究表明,腹腔鏡手術與傳統開放手術相比減少了暴力操作對胃腸道的影響,對胃腸道生理功能影響較小,一般術后第二天便可恢復胃腸蠕動,并且進食流質[15]。本組腹腔鏡下組織結構分離方法在腹外斜肌與腹內斜肌的間隙內進行操作[16],避免了開放式疝修補手術所需要的廣泛組織分離,減少穿支血管的損傷,術中滲血少,內鏡鏡下解剖結構更清晰,同時能夠發現隱匿性疝并作積極的處理,這些在傳統手術中往往很難做到,腹腔鏡下操作降低對腹壁的二次損傷,避免腹壁原有解剖結構的改變,因此,B組患者住院時間、術后復發率及并發癥發生率均得以降低。本研究指標包括住院費用比較,盡管腹腔鏡及配套器械的使用費用高于開放式手術,但腹腔鏡組患者的住院時間縮短、術后用藥減少使得兩組間費用差異沒有統計學意義。
綜上所述,腹腔鏡下組織結構分離術與傳統開放疝修補術相比,不增加手術時間和手術費用,同時可以有效地減少術中出血量,縮短術后進食時間,降低術后住院時間、術后復發率及并發癥發生率。
[1] LEBLANC K. Proper mesh overlap is a key determinant in hernia recurrence following laparoscopic ventral and incisional hernia repair[J]. Hernia, 2016, 20(1): 85-99.
[2] BRADY R R W, VENTHAM N T, ANDREW C, et al. Laparoscopic partially extraperitoneal (PEP) mesh repair for laterally placed ventral and incisional hernias[J]. Surg Laparosc Endosc Percutan Tech, 2014, 24(3): 99-100.
[3] ROGMARK P, PETERSSON U, BRINGMAN S, et al. Quality of life and surgical outcome 1 Year after open and laparoscopic incisional hernia repair: PROLOVE: a randomized controlled trial[J]. Ann Surg, 2016, 263(2): 244-250.
[4] COMAJUNCOSAS J, HERMOSO J, GRIS P, et al. Risk factors for umbilical trocar site incisional hernia in laparoscopic cholecystectomy: a prospective 3-year follow-up study[J]. Am J Surg, 2014, 207(1): 441-446.
[5] ROGMARK P, PETERSSON U, BRINGMAN S, et al. Shortterm outcomes for open and laparoscopic midline incisional hernia repair: a randomized multicenter controlled trial: the ProLOVE (prospective randomized trial on open versus laparoscopic operation of ventral eventrations) trial[J]. Am J Surg, 2013, 258(1): 37-45.
[6] NGUYEN D H, NGUYEN M T, ASKENASY E P, et al. Primary fascial closure with laparoscopic ventral hernia repair: systematic review[J]. World J Surg, 2014, 38(12): 3097-3104.
[7] COBB W S, WARREN J A, EWING J A, et al. Open retromuscular mesh repair of complex incisional hernia: predictors of wound events and recurrence[J]. J Am Coll Surg, 2015, 220(4): 606-613.
[8] ZHANG Y, ZHOU H, CHAI Y, et al. Laparoscopic versus open incisional and ventral hernia repair: a systematic review and meta-analysis[J]. World J Surg, 2014, 38(9): 2233-2240.
[9] LEONARD J, HIEKEN T J, HUSSEIN M, et al. Delineation of factors associated with prolonged length of stay after laparoscopic ventral hernia repair leads to a clinical pathway and improves quality of care[J]. Surg Endosc, 2016, 30(4): 1614-1618.
[10] SILECCHIA G, CAMPANILE F C, SANCHEZ L, et al. Laparoscopic ventral/incisional hernia repair: updated Consensus Development Conference based guidelines [corrected][J]. Surg Endosc, 2015, 29(9): 2463-2484.
[11] ARMA?ANZAS L, RUIZ-TOVAR J, ARROYO A, et al. Prophylactic mesh vs suture in the closure of the umbilical trocar site after laparoscopic cholecystectomy in high-risk patients for incisional hernia. A randomized clinical trial[J]. J Am Coll Surg., 2014, 218(5): 960-968.
[12] CARTER S A, HICKS S C, BRAHMBHATT R, et al. Recurrence and pseudorecurrence after laparoscopic ventral hernia repair: predictors and patient-focused outcomes[J]. Am Surg, 2014, 80(2): 138-148.
[13] GOODENOUGH C J, KO T C, KAO L S, et al. Development and validation of a risk stratification score for ventral incisional hernia after abdominal surgery: hernia expectation rates in intra-abdominal surgery (the HERNIA Project)[J]. J Am Coll Surg, 2015, 220(4): 405-413.
[14] AL CHALABI H, LARKIN J, MEHIGAN B, et al. A systematic review of laparoscopic versus open abdominal incisional hernia repair, with meta-analysis of randomized controlled trials[J]. Int J Surg, 2015, 20: 65-74.
[15] DE SILVA G S, KRPATA D M, HICKS C W, et al. Comparative radiographic analysis of changes in the abdominal wall musculature morphology after open posterior component separation or bridging laparoscopic ventral hernia repair[J]. J Am Coll Surg, 2014, 218(3): 353-357.
[16] SILECCHIA G, CAMPANILE F C, SANCHEZ L, et al. Laparoscopic ventral/incisional hernia repair: updated guidelines from the EAES and EHS endorsed Consensus Development Conference[J]. Surg Endosc, 2015, 29(9): 2463-2484.
The application of organizational separation technology under endoscopic on the treatment of abdominal incisional hernia
REN Yan, LIU Juan, YAN Feng, PENG Min.
(Department of Gastrointestinal Surgery, The First Affiliated Hospital of Chengdu Medical College,Chengdu 610500 China)
Objective: The objective of this study was to explore the difference of organizational separation technology under endoscopic and traditional open hernia repair on the treatment of abdominal incisional hernia. Methods: A total of 96 abdominal incisional hernia patients under general anesthesia were randomly divided into A and B group, with each group 48 cases. A group was given traditional treatment while B group was provided with organizational separation technology under endoscopic. The operative time, bleeding volume, postoperative feeding time, length of stay, hospitalizing fee, recurrence rate and complication incidence were compared between two groups. Results: The difference of operative time and hospitalizing fee of two groups was not statistically signif i cant(P>0.05). the bleeding volume, postoperative feeding time, and length of stay of B group were less than that of A group and the difference was statistically signif i cant(P<0.05). The recurrence rate and complication incidence of B group were signif i cantly lower than that of A group and the difference was statistically signif i cant(P<0.05). Conclusions: Comparing to the traditional treatment, the treatment of organizational separation technology under endoscopic is capable of decreasing the bleeding volume, shortening the postoperative feeding time, cutting down the length of stay, recurrence rate and complication incidence without increasing the hospitalizing time and operation fee.
endoscopic; organizational separation; abdominal incisional hernia
R656.3
A
2095-5200(2017)04-113-03
10.11876/mimt201704046
任雁,本科,主治醫師,研究方向:胃腸外科臨床,Email:2477837621@qq.com。
猜你喜歡
腹腔鏡外科雜志(2022年7期)2022-08-16 04:31:06
哲學評論(2021年2期)2021-08-22 01:53:34
河北畫報(2020年10期)2020-11-26 07:20:50
中華詩詞(2019年7期)2019-11-25 01:43:04
中國內鏡雜志(2017年2期)2017-03-20 16:18:12
影視與戲劇評論(2016年0期)2016-11-23 05:26:01
腹腔鏡外科雜志(2016年11期)2016-06-01 12:10:09
腹腔鏡外科雜志(2016年9期)2016-06-01 12:10:07
中國衛生標準管理(2015年3期)2016-01-14 03:41:47
現代企業(2015年9期)2015-02-28 18:56:50
