癲癇患兒發病的危險因素的分析
2017-07-25 07:58:52章素芳程鵬
中國當代醫藥 2017年17期
章素芳++程鵬

[摘要]目的 探討癲癇患兒發病的危險因素。方法 選取2013年1月~2015年1月我院120例癲癇患兒作為癲癇組,選取同期健康體檢者100例作為對照組。比較兩組研究對象一般特征、癲癇家族史、出生狀況、既往病史等,采用多因素非條件Logistic回歸觀察癲癇的危險因素。結果 癲癇組患兒發病年齡0~1歲者占比高于對照組,>5~6歲者占比低于對照組(P<0.05);癲癇家族史、母親適齡懷孕、產傷、高熱驚厥、顱腦感染、顱腦損傷患者發生癲癇的比例較高,差異均有統計學意義(P<0.05);多因素非條件Logistic回歸分析結果顯示,產傷、母親適齡懷孕、高熱驚厥史、顱腦損傷史、癲癇家族史是癲癇發作的危險因素(P<0.05)。結論 分析癲癇患兒發病的危險因素,產傷、母親適齡懷孕、高熱驚厥史、顱腦損傷史、癲癇家族史是癲癇發作的危險因素,可以為指導臨床治療癲癇提供可靠的理論依據。
[關鍵詞]癲癇;發病;一般特征;癲癇家族史;出生狀況;既往病史;危險因素
[中圖分類號] R742.1 [文獻標識碼] A [文章編號] 1674-4721(2017)06(b)-0083-03
[Abstract]Objective To approach hazards of epilepsy children morbidity.Methods The 120 children with epilepsy in our hospital from January 2013 to January 2015 were selected as epilepsy group,then 100 healthy children check-up in our hospital in the same period were selected as control group.The general features,epilepsy family history,born,anamnesis and epilepsy were compared between the two groups.The multiple-factor non-conditional Logistic regression analysis was used to analyzed the epilepsy hazards.Results The proportion of children whose epilepsy onset at 0-1 age in the epilepsy group was higher than the control group,proportion of children whose epilepsy onset at >5-6 age was lower than the control group (P<0.05);the proportion of epileptic seizure in children with epilepsy family history,mother age pregnancy,birth injury,hyperpyretic convulsion,brain infection,craniocerebral injury was higher,the differences were statistical significance (P<0.05).The multiple-factor non-conditional Logistic regression analysis showed that,birth injury,mother age pregnancy,hyperpyretic convulsion,craniocerebral injury,epilepsy family history were hazards of epileptic seizure (P<0.05).Conclusion Analyzing of the risk factors of the epilepsy,the birth injury,mother age pregnancy,hyperpyretic convulsion,craniocerebral injury,epilepsy family history are hazards of epileptic seizure,which can guide clinical treatment epilepsy for providing reliable theory basis.
[Key words]Epilepsy;Morbidity;General features;Epilepsy family history;Born status;Anamnesis;Hazards
癲癇是一種慢性腦疾患,其病因復雜多樣,是目前僅次于腦血管病、老年癡呆的第三類常見性神經疾病[1-2]。近年來,隨著癲癇發生率明顯升高,國內外關于癲癇發病危險因素的研究也逐漸增多[3-4]。目前多項研究報道顯示癲癇的年發病率為(20~70)/10萬,患病率達到4‰~10‰[5-6]。癲癇作為兒科一種常見的急癥,其發病急、病因復雜、發展迅速、預后較差、死亡率高,需要給予有效的治療措施,才可以預防神經系統后遺癥的發生。我國癲癇發生率遠高于世界平均水平,因而針對癲癇發病危險因素研究應該引起臨床廣泛重視,從而更好地為臨床預防和治療癲癇提供可靠的理論依據[7-8]。
1資料與方法
1.1一般資料
回顧性分析2013年1月~2015年1月我院收治的120例癲癇患兒的臨床資料,其中男62例,女58例;年齡7個月~6歲,平均年齡(2.5±1.0)歲;均為原發性癲癇,癲癇發作類型:單純部分發作持續狀態15例,肌陣攣持續狀態15例,復雜部分發作持續狀態20例,全面強直陣攣發作持續狀態70例。選取同期健康體檢嬰幼兒100例作為對照組,其中男43例,女57例;年齡1~7歲,平均年齡(2.8±1.1)歲。本研究經我院醫學倫理委員會批準。
1.2方法
采用問卷調查的方式分別對患兒的性別、年齡、既往疾病史、健康狀況、癲癇患病情況、癲癇遺傳史進行調查。
1.3觀察指標
觀察兩組研究對象一般特征、癲癇家族史、出生狀況、既往病史和癲癇發作的關系情況及癲癇發作多因素非條件Logistic回歸情況。一般特征主要包括性別、年齡情況;既往疾病史主要包括高熱驚厥、顱腦感染、顱腦損傷、顱腦腫瘤;出生狀況主要包括母親適齡懷孕、母親孕前2年患病、母親孕期嚴重反應、產傷。
1.4統計學方法
采用SPSS 19.0統計學軟件進行數據分析,計數資料用率表示,組間比較采用χ2檢驗,多因素非條件Logistic回歸分析,以P<0.05為差異有統計學意義。
2結果
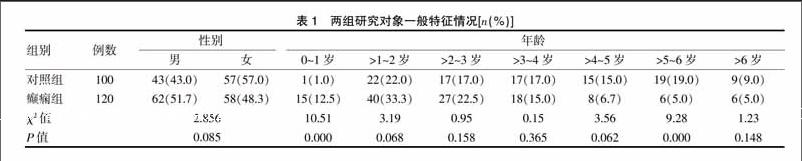
2.1兩組研究對象一般特征情況
癲癇組患兒發病年齡0~1歲者比例高于對照組,>5~6歲的比例低于對照組,差異有統計學意義(P<0.05)(表1)。
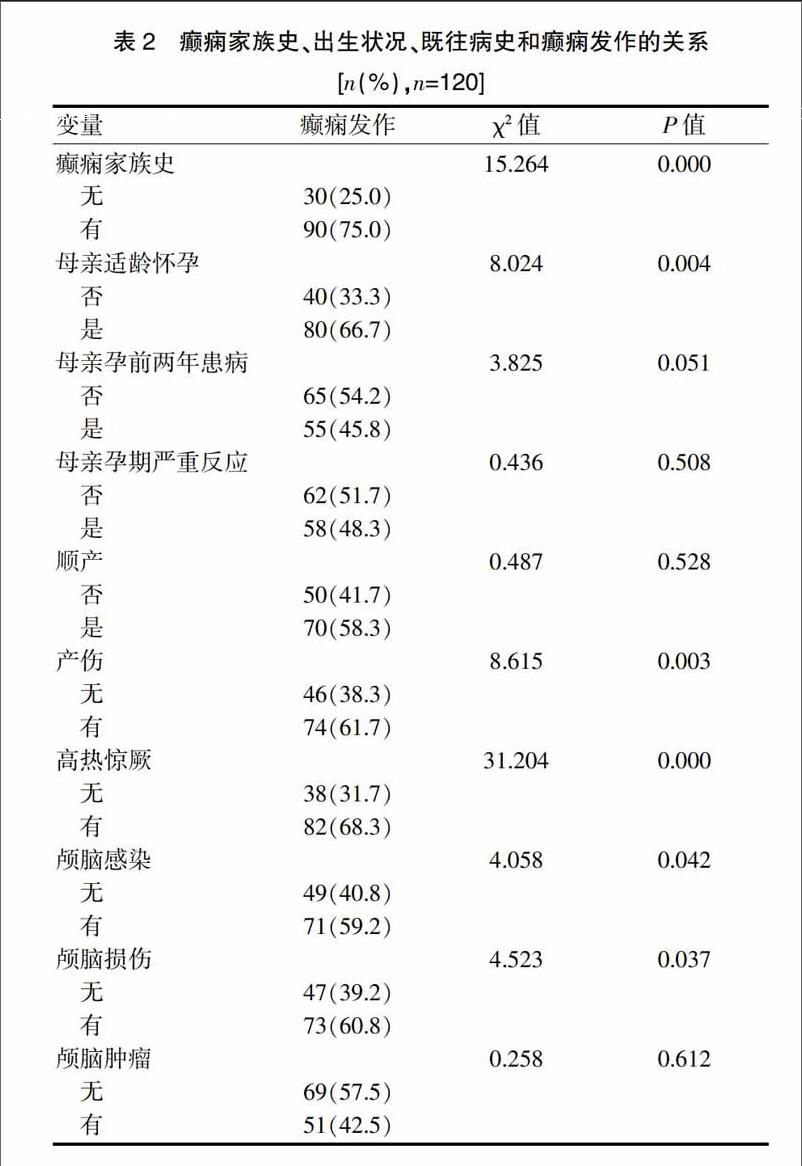
2.2癲癇家族史、出生狀況、既往病史和癲癇發作的關系
有癲癇家族史、母親適齡懷孕、產傷、高熱驚厥、顱腦感染、顱腦損傷患者發生癲癇的比例較高,差異均有統計學意義(P<0.05)(表2)。
2.3癲癇危險因素的多因素非條件Logistic回歸分析情況
多因素非條件Logistic回歸分析結果顯示,產傷、母親適齡懷孕、高熱驚厥史、顱腦損傷史、癲癇家族史是癲癇發作的危險因素(P<0.05)(表3)。
3討論
目前關于癲癇的病因和發病機制研究較多,主要包括細胞學說、神經遞質學說、離子通道和免疫學說[9-10]。癲癇作為腦部疾病,其具有反復性發作,易感性較強等特點,容易引起患兒神經生化、認知功能、心理情緒等不良反應[11-12]。癲癇發病的主要危險因素有家族史、先天及圍生期異常、顱腦外傷、中樞神經系統感染、腦血管疾病等。
本研究選取我院2013年1月~2015年1月120例癲癇患兒作為癲癇組,選取同期健康體檢者100例作為對照組,觀察兩組的一般特征、癲癇家族史、出生狀況、既往病史與癲癇的關系情況,結果顯示,癲癇組患兒發病年齡0~1歲比例高于對照組,>5~6歲的比例低于對照組,提示癲癇患兒發病的危險因素在0~1歲表現的更加明顯。母親適齡懷孕、產傷和癲癇發作有關系,母親適齡懷孕、產傷均和癲癇有密切的關系,母親適齡懷孕均是癲癇的保護因素,而產傷作為母親妊娠期病理性因素,和癲癇的發作有密切的關系,是癲癇發作的危險性因素之一。本研究中,高熱驚厥、顱腦感染、顱腦損傷和癲癇發作有相關性,年齡、產傷、母親適齡懷孕、高熱驚厥史、顱腦損傷史、癲癇家族史是癲癇發作的危險因素,高熱驚厥史嬰幼兒常見的神經系統疾病。有資料顯示[13-15],癲癇患兒中有近20%具有高熱驚厥史,高熱驚厥又可以激發癲癇。顱腦感染、顱腦損傷會導致大腦組織受到傷害,無法痊愈時,可能誘發癲癇的發作,被稱為外傷性癲癇,屬于腦外傷常見的、嚴重的并發癥。腦損傷越嚴重發生癲癇的概率越大。針對上述癲癇危險因素的分析,有效地做好癲癇預防工作顯得尤為重要:①母親孕期保健、定期產檢、圍生期保健、降低產前因素的發生率、減少癲癇發生的母親病理性因素的出現。②兒童注意按時預防接種各類腦炎疫苗,降低顱內感染的發生率。③針對小兒高熱要提高重視程度,及早進行治療,避免高熱驚厥發生,減少因缺氧性腦損傷引起的癲癇。④加強安全教育,注意做好腦外傷意外性傷害的防護,積極治療腦血管疾病,加強生產、工作安全,降低因意外性腦損傷、腦缺氧和中毒引起的癲癇的發生。
綜上所述,分析癲癇患兒發病的危險因素,可以為指導臨床治療癲癇提供可靠的理論依據。
[參考文獻]
[1]Ochoa-Gomez L,Lopez-Pison J,Fernando-Martinez R,et al.A descriptive study of non-symptomatic epilepsy according to age at onset at a Neuropediatric Section of regional reference[J].Rev Neurol,2016,63(10):447-454.
[2]Lee YK,Ah YM,Choi YJ,et al.Antiepileptic drug adherence and persistence in children with epilepsy attending a large tertiary care children's hospital[J].Epileptic Disord,2016,53(10):448-449.
[3]Podkorytova I,Gupta A,Wyllie E,et al.Aicardi syndrome:epilepsy surgery as a palliative treatment option for selected children and pathological findings[J].Epileptic Disord,2016, 53(10):39-41.
[4]Haegelen C,Perucca P,Chaillon CE,et al.High-frequency oscillations,extent of surgical resection,and surgical outcome in drug-resistant focal epilepsy[J].Epilepsia,2013,54(5):848-857.
[5]Miserocchi A,Cascardo B,Piroddi C,et al.Surgery for temporal lobe epilepsy in children:relevance of presurgical evaluation and analysis of outcome[J].J Neurosurg Pediatr,2013,11(3):256-267.
[6]郝美美,秦娜,張彥,等.216例癥狀性癲癇臨床特點及預后危險因素分析[J].中華神經外科疾病研究雜志,2016,4(9):301-304.
[7]Deling L,Nan J,Yongji T,et al.Intraventricular ganglioglioma prognosis and hydrocephalus:the largest case series and systematic literature review[J].Acta Neurochir(Wien),2013,155(7):1253-1260.
[8]Caboclo LO,Neves RS,Jardim AP,et al.Surgical and postmortem pathology studies:contribution for the investigation of temporal lobe epilepsy[J].Arq Neuropsiquiatr,2012,70(12):945-952.
[9]Bulteau C,Otsuki T,Delalande O.Epilepsy surgery for hemispheric syndromes in infants:hemimegalencepahly and hemispheric cortical dysplasia[J].Brain Dev,2013,7604(13):167-168.
[10]Hauptman JS,Dadout A,Oh T,et al.Sociodemographic changes over 25 years of pediatric epilepsy surgery at UCLA[J].J Neurosurg Pediatr,2013,11(3):250-255.
[11]Yasuda CL,Cendes F.Neuroimaging for prediction of response to medical and surgical treatment in epilepsy[J].Expery Opin Med Diagn,2012,6(4):295-308.
[12]黃月艷,秦炯.兒童癲癇持續狀態56例臨床研究[J].實用醫學雜志,2011,27(13):2402-2404.
[13]鄭華成.小兒癲癇持續狀態的幾點認識[J].中華臨床醫師雜志,2013,7(13):5741-5742.
[14]中華醫學會神經病學分會腦電圖與癲癇分組.非驚厥性癲癇持續狀態的治療專家共識[J].中華神經科雜志,2013, 46(2):133-137.
[15]申浩,常亮,管軍,等.昏迷患者非驚厥性癲癇持續狀態的臨床特點[J].臨床神經病學雜志,2013,26(3):228-230.
(收稿日期:2017-04-06 本文編輯:任 念)
猜你喜歡
中國民間療法(2021年5期)2021-06-09 09:21:04
飲食科學(2017年5期)2017-05-20 17:11:53
今日健康(2016年12期)2016-11-17 14:41:50
今日健康(2016年12期)2016-11-17 13:12:34
今日健康(2016年12期)2016-11-17 12:29:29
科技資訊(2016年19期)2016-11-15 10:33:36
中國實用醫藥(2016年24期)2016-10-17 05:32:48
養生保健指南(2016年4期)2016-03-22 12:25:57
安徽醫科大學學報(2015年9期)2015-12-16 11:09:44
西南軍醫(2015年4期)2015-01-23 01:19:30