手足口病重癥患兒營養素水平與病情的相關性分析
2016-04-15 01:37:20王曉波杜潘艷趙玉萍王寶林高翠紅
中國免疫學雜志 2016年3期
關鍵詞:相關性
王曉波 杜潘艷 趙玉萍 王寶林 高翠紅 張 雙
(唐山市婦幼保健院,唐山063000)
?
手足口病重癥患兒營養素水平與病情的相關性分析
王曉波杜潘艷趙玉萍王寶林高翠紅張雙
(唐山市婦幼保健院,唐山063000)
[摘要]目的:探討手足口病患兒外周血中營養素前白蛋白(PA)、纖維連接蛋白(FN)、視黃醇結合蛋白(RBP)、C-反應蛋白(CRP)、微量元素鐵、鋅及維生素D(VitD)水平與病情的相關性。方法:采用免疫比濁法檢測PA、FN、RBP和CRP水平;采用火焰原子吸收法檢測全血微量元素鐵、鋅水平;采用電化學發光法檢測VitD水平。結果:重癥組與普通組、對照組比較,PA、FN、RBP、鐵、鋅及VitD水平均低,CRP水平升高(P<0.05);普通組與對照組比較,PA 、FN和RBP水平均降低,CRP水平升高(P<0.05);鐵、鋅及VitD水平在普通組和對照組間無統計學意義(P>0.05)。重癥恢復期PA、FN、RBP、鐵、鋅及VitD水平均高于急性期(P<0.01),但仍低于對照組(P<0.05);恢復期CRP水平與對照組無統計學意義(P>0.05)。PA、FN和RBP水平與手足口病病情呈顯著負相關(P<0.05);而CRP與病情呈顯著正相關(P<0.05);鐵、鋅、VitD水平與病情呈低度負相關(P<0.05)。結論:手足口病重癥病例存在營養缺乏,臨床應對其進行營養狀態動態評估并適量補充營養。
[關鍵詞]手足口病;重癥;營養素;相關性
手足口病(Hand,foot and mouse disease,HFMD)是一種主要由腸道病毒引發的急性傳染病。普通病例呈自限性,重癥病例可合并神經系統、呼吸系統、循環系統等嚴重并發癥[1]。低齡兒童是易感人群。有研究表明兒童體內營養素缺乏可影響免疫系統功能,容易發生感染性疾病[2,3]。本研究對本院確診的手足口病患兒外周血中營養指標前白蛋白(Pre albumin,PA)、纖維連接蛋白(Fibronectin,FN)、視黃醇結合蛋白(Retinol binding protein,RBP)、C-反應蛋白(C- reactive protein,CRP)、微量元素鐵(Iron)、鋅(Zinc)及維生素D(Vitamin D,VitD)水平等進行總結分析,并探討其與病情相關性。
1資料與方法
1.1研究對象病例組為2013年6月~2015年8月期間于本院兒科已確診的手足口病病例381例,年齡4月~8歲,平均年齡(3.2±1.2)歲。根據《手足口病診療指南 (2010年版)》臨床分類標準[4]表1病例組和對照組比較結果將病例分為普通組和重癥組。普通組276例,男142例,女134例,平均年齡(3.4±1.1)歲;重癥組105例,男56例,女49例,平均年齡(2.9±1.0)歲。對照組88例,為病例收集同期于兒童保健科體檢的健康兒童,男47例,女41例,年齡4月~8歲,平均年齡(3.2±1.0)歲,且近1月內未發生過消化系統疾病。對照組與病例組間性別、年齡比較,均無統計學意義(P>0.05)。
Tab.1Comparison between case group and control group

GroupsCasesPA(mg/L)FN(mg/L)RBP(mg/L)CRP(mg/L)Iron(mmol/L)Zn(μmol/L)VitD(nmol/L)Control88256.9±33.4236.6±38.939.4±8.21.7±0.98.4±2.289.4±8.341.6±8.4General276224.3±40.2217.3±44.734.6±10.515.5±9.28.2±2.386.8±17.938.2±16.6Severe105182.5±30.6168.6±43.926.7±9.445.4±19.76.7±2.670.4±12.831.5±12.7P1)<0.05P2)<0.05>0.05
Note:1)Comparison between the severe group and the general、control group;2)Comparison between the general group and control group.
表2重癥組急性期與恢復期比較結果
Tab.2Comparison between acute phase and convalescence of severe group

GroupsCasesPA(mg/L)FN(mgl/L)RBP(mg/L)Iron(mmol/L)Zn(umol/L)VitD(nmol/L)CRP(mg/L)Control88256.9±33.4236.6±38.939.4±8.28.4±2.289.4±8.341.6±8.41.7±0.9Acutestage105182.5±30.6168.6±43.926.7±9.46.7±2.670.4±12.831.5±12.745.4±19.7Recoveryperiod105211.4±46.6192.4±48.532.8±10.77.3±2.880.8±8.436.5±10.72.4±1.5P1)<0.01P2)<0.05>0.05
Note:1)Comparison of convalescence and acute phase;2)Comparison of convalescence and control group.
1.2實驗方法采集研究對象入院12 h內及重癥患兒恢復期空腹靜脈血3管,一管肝素鋰抗凝2 ml,采用火焰原子吸收法檢測全血微量元素鐵、鋅水平,試劑由北京博暉公司提供;兩管無抗凝劑3 ml,分離血清,其中1管采用免疫比濁法檢測PA、FN、RBP、CRP水平,試劑由南京波音特生物科技公司提供;另1管采用電化學發光法檢測維生素D水平,試劑為德國羅氏診斷公司提供。

2結果
2.1病例組和對照組比較結果重癥組與普通組、對照組比較,患兒PA、FN、RBP、鐵、鋅及VitD水平均低,CRP水平升高,差異均有統計學意義(P<0.05);普通組與對照組比較,PA、FN和RBP水平均降低,CRP水平升高,差異均有統計學意義(P<0.05);微量元素鐵、鋅及VitD水平在普通組和對照組間無統計學意義(P>0.05)。見表1。
表3營養素與HFMD病情相關性
Tab.3Correlation between nutrients and state of HFMD
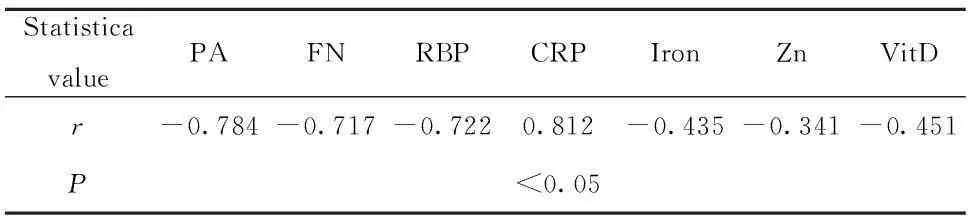
StatisticavaluePAFNRBPCRPIronZnVitDr-0.784-0.717-0.7220.812-0.435-0.341-0.451P<0.05
2.2重癥組急性期與恢復期比較結果重癥組患兒恢復期與急性期比較,PA、FN、RBP、鐵、鋅及VitD水平均升高(P<0.01);但這些指標水平均低于對照組(P<0.05);恢復期CRP水平降低,與對照組無統計學意義(P>0.05)。見表2。
2.3營養素與HFMD病情相關性PA、 FN、RBP水平與HFMD病情呈顯著負相關(P<0.05);而CRP與病情呈顯著正相關(P<0.05);鐵、鋅、VitD水平與病情呈中度負相關(P<0.05)。見表3。
3討論
手足口病起病急,病情發展迅猛,控制不及時容易發展成重癥病例,甚至危及生命。HFMD的發生發展與機體免疫水平密切相關[5],而人體免疫水平的高低受多種因素影響,其中營養因素起著非常重要的作用,是維持人體正常免疫功能和健康的物質基礎。營養失調會對人體免疫系統造成很大損傷。有研究顯示在發展中國家入院或重癥監護病房存在急性或慢性營養不良的患兒可達53%[6]。
PA、FN、RBP對于急性營養不良具有早期診斷價值,能及時反映患者腸外營養狀況及恢復[7,8]。微量元素鐵、鋅和VitD在調節和介導免疫反應的過程中有著重要的作用,營養素缺乏影響機體免疫功能[9-11]。本研究中HFMD病患兒,尤其是重癥病例營養素水平均低,與病情嚴重程度呈負相關,提示手足口病存在營養素缺乏,營養素水平可能影響機體正常的免疫功能。住院期間患兒受多種因素影響,營養狀況進一步惡化,易導致病情加重,而病情惡化又會影響營養素的攝入、合成和吸收[3]。因此重癥患兒住院期間營養風險篩查和營養評估至關重要。
CRP作為非特異性急性炎性反應標記物,在急性應激反應狀態下,肝臟優先合成CRP而減少合成白蛋白、前白蛋白[12]。有研究用CRP與PA的比值作為評估消化系統手術成功的指標[13]。本研究中CRP水平與HFMD病情呈顯著正相關,提示CRP不僅可以判斷疾病的嚴重程度[14],還可以間接反映患者營養狀況。
本研究中重癥患兒恢復期營養素水平均高于急性期,提示臨床應對重癥病例進行營養狀態動態評估,有助于監測病情。重癥患兒恢復期營養素水平仍低于健康兒童,可能由于病毒對患兒機體造成炎性反應,盡管處于恢復期,但仍會影響機體對營養素的吸收和合成。
綜上所述,手足口病重癥患兒存在營養素缺乏狀況,在疾病的診療過程中進行定期、動態評估并及時給予補充,可利于監測病情及改善預后。
參考文獻:
[1]Ma E,Chan KC ,Cheng P,etal.The Enterovirus 71 epidemic in 2008 --public health implications for Hong Kong[J].Int Infection Dis,2010,14(9):e775-e780.
[2] Mao S,Zhang A,Huang S.Meta-analysis of Zn,Cu and Fe in the hair of Chinese children with recurrent respiratory tract infection[J].Scand J Clin Lab Invest,2014 ,74(7):561-567.
[3]Krawinkel MB.Interaction of nutrition and infections globally:an overview[J].Ann Nutr Metab,2012,61(Suppl 1):39-45.
[4]衛生部辦公廳關于印發《手足口病診療指南(2010年版)》的通知[EB/OL].(2010-04-06)[2010-06-01]http://www.moh.gov.cn/publicfiles/business/ht mlfiles/mohyzs/s3586/202004/46884.htm.
[5] Zhang Y,Liu H,Wang L,Yang F,etal.Comparative study of the cytokine/chemokine response in children with differing disease severity in enterovirus 71- induced hand,foot,and mouth disease[J].PLoS One,2013,8(6):e67430.
[6] Bhutta ZA,Salam RA.Global nutrition epidemiology and trends[J].Ann Nutr Metab,2012,61(Suppl 1):19-27.
[7]Xu D,Li J,Song Y,etal.Laparoscopic surgery contributes more to nutritional and immunologic recovery than fast-track care in colorectal cancer[J].World J Surg Oncol,2015,13(1):18.
[8]Feferbaum R,Delgado AF,Zamberlan P,etal.Challenges of nutritional assessment in pediatric ICU[J].Curr Opin Clin Nutr Metab Care,2009,12(3):245-250.
[9]Cassat JE,Skaar EP.Iron in infection and immunity[J].Cell Host Microbe,2013,13(5):509-519.
[10]Nishida K.New knowledge from past decade:role of zinc in immune system[J].Nihon Eiseigaku Zasshi,2013,68(3):145-152.
[11]Lang PO,Samaras N,Samaras D,etal.How important is vita min D in preventing infections?[J].Osteoporos Int,2013 ,24(5):1537-1553.
[12] Mehta NM,Compher C;A.S.P.E.N.Board of Directors.A.S.P.E.N.Clinical Guidelines:nutrition support of the critically ill child[J].JPEN J Parenter Enteral Nutr,2009 ,33(3):260-276.
[13]Harriman S,Rodych N,Hayes P,etal.The C-reactive protein:prealbu min ratio as a predictor of successful surgical closure of gastrointestinal fistulas[J].Am Surg,2015,1(2):73-77.
[14]Page AL,de Rekeneire N,Sayadi S,etal.Diagnostic and prognostic value of procalcitonin and C-reactive protein in malnourished children[J].Pediatrics,2014,133(2):e363-370.
[收稿2015-09-11修回2015-09-21]
(編輯倪鵬)
Correlation of nutrient levels and state of severe cases with HFMD
WANGXiao-Bo,DUPan-Yan,ZHAOYu-Ping,WANGBao-Lin,GAOCui-Hong,ZHANGShuang.
TangshanWomenandChildrenHealth-CareHospital,Tangshan063000,China
[Abstract]Objective:To detect the levels of PA,FN,RBP,CRP,Iron,Zinc,VitD in peripheral blood of children with HFMD and to explore the relationship between them and the disease.Methods: The levels of PA,FN,RBP and CRP were detected by immune turbidimetric assay;and the levels of Iron and Zinc were detected by flame atomic absorption spectrometry;while the levels of VitD were detected by electro chemilumin escence.Results: The levels of PA,FN,RBP,Iron,Zinc and VitD in the severe group were lower than those in other groups,while the levels of CRP were higher than those in other groups(P<0.05);and the levels of PA,FN and RBP in the general group were lower than that in the control group,while the levels of CRP were higher than that in the control group(P<0.05).And no significance were found of the levels of Iron,Zinc and VitD in the general group and the control group(P>0.05).The levels of PA,FN,RBP,Fe,Zn and VitD in the convalescence were higher than those in the acute phase of the severe cases(P<0.01),and lower than those in the control group(P<0.05);And no statistical significance were found of the levels of CRP between the convalescent phase of severe cases and the control group(P>0.05).There were negative correlation between the levels of PA,FN,RBP and the state of HFMD(P<0.05),while there were positive correlation between the levels of CRP and the state of HFMD(P<0.05).And there were low negative correlation between the levels of Iron,Zinc,VitD and the state of HFMD(P<0.05),respectively.Conclusion: There were nutritional deficiency in severe cases of HFMD,and the nutritional status should be assessed dynamically,then proper amount of nutrition should be supplement.
[Key words]HFMD;Severe cases;Nutrients;Correlation
中圖分類號R725.1
文獻標志碼A
文章編號1000-484X(2016)03-0414-03
作者簡介:王曉波(1976年-),男,主管檢驗師,主要從事臨床兒科檢驗研究。
doi:10.3969/j.issn.1000-484X.2016.03.026
猜你喜歡
商情(2016年42期)2016-12-23 14:25:52
商情(2016年42期)2016-12-23 13:35:35
東方教育(2016年4期)2016-12-14 22:15:13
財經界·學術版(2016年19期)2016-11-16 16:28:33
科技視界(2016年21期)2016-10-17 17:37:34
中國實用醫藥(2016年24期)2016-10-17 04:31:12
中國實用醫藥(2016年24期)2016-10-17 03:37:40
中國實用醫藥(2016年24期)2016-10-17 03:35:06
科學與財富(2016年28期)2016-10-14 21:58:50