不同手術入路治療Siewert Ⅱ、Ⅲ型食管胃結合部腺癌近期療效對比▲
2016-02-17 03:47:40孫啟超吳鵬飛
廣西醫學 2016年2期
關鍵詞:手術
孫啟超 吳鵬飛
(江蘇省如皋市人民醫院1 胸外科,2 普外科,如皋市 226500,E-mail:15062747967@163.com)
不同手術入路治療Siewert Ⅱ、Ⅲ型食管胃結合部腺癌近期療效對比▲
孫啟超1吳鵬飛2
(江蘇省如皋市人民醫院1 胸外科,2 普外科,如皋市 226500,E-mail:15062747967@163.com)
目的 比較經腹食管裂孔入路與經胸入路手術治療SiewertⅡ、Ⅲ型食管胃結合部腺癌(AEG)的臨床效果。方法 82例SiewertⅡ、Ⅲ型AEG患者,根據不同手術路徑分為經胸手術組(經胸組)38例和經腹食管裂孔手術組(經腹組)44例。比較兩組患者術中出血量、手術時間、淋巴結清掃數、術后切口疼痛程度(視覺模擬評分)、術后住院時間、術后并發癥發生率等臨床資料。結果 兩組均無圍術期死亡病例,根治度均達到R0切除。經腹組手術時間、術中出血量、視覺模擬評分、術后住院時間均明顯少于或低于經胸組(P<0.05),腹腔淋巴結清掃數明顯多于經胸組(P<0.05)。經腹組術后并發癥發生率為11.4%(5/44),明顯低于經胸組的31.6%(12/38)(P<0.05)。兩組縱隔淋巴結清掃數比較,差異無統計學意義(P>0.05)。結論 與經胸入路手術比較,經腹食管裂孔入路治療SiewertⅡ、Ⅲ型AEG患者在腹腔淋巴結清掃數方面具有明顯優勢,且術后并發癥發生率更低。
食管胃結合部腺癌;SiewertⅡ型;SiewertⅢ型;手術入路;經腹;食管裂孔;經胸;療效
食管胃結合部腺癌(adenocarcinoma of the esophagogastric junction,AEG)是指腫瘤中心位于食管胃結合部,且遠端和近端范圍均不超過5 cm的腫瘤[1]。近年來我國AEG的發病率呈上升趨勢[2]。臨床上AEG分為3型,其中SiewertⅠ型患者的生物學特征更接近食管癌,其外科治療一般采用經胸手術入路。但SiewertⅡ、Ⅲ型患者的手術入路選擇存在爭議[3]。本研究回顧性分析82例SiewertⅡ、Ⅲ型AEG患者的臨床資料,比較不同手術路徑的臨床療效,以供臨床參考。
1 資料與方法
1.1 臨床資料 2007年3月至2013年12月我院收治的SiewertⅡ、Ⅲ型AEG患者82例,其中男55例,女27例,年齡45~88歲,平均62歲。根據不同手術路徑分為經胸手術組(經胸組)38例和經腹食管裂孔手術組(經腹組)44例。兩組患者年齡、性別、Siewert分型、TNM分期等臨床資料比較,差異無統計學意義(P>0.05),具有可比性。見表1。

表1 兩組臨床資料比較
1.2 納入標準和排除標準 納入標準:(1)術前經胃鏡、活組織病理檢查證實為SiewertⅡ、Ⅲ型AEG 患者;(2)腫瘤未發生遠處轉移;(3)術前未接受輔助放化療。排除標準:(1) SiewertⅠ型AEG患者;(2)姑息性手術或者僅行探查術者;(3)臨床資料不全者。
1.3 手術方法 所有患者均使用靜吸復合插管全麻。經胸組由胸外科醫師主刀,取右側臥位,在左側胸6、7肋間后外側做一切口,行全胃及近端胃切除、第2站淋巴結清掃術。經腹組患者由普外科醫師主刀,取平臥位,采用腹上區正中手術切口、食管裂孔入路,行全胃及近端胃切除及第2站淋巴結清掃術。
1.4 觀察指標 (1)術中情況,包括手術出血量、手術時間、淋巴結清掃數;(2)術后恢復情況,包括術后切口疼痛程度、術后住院時間、術后并發癥發生率。術后切口疼痛程度于術后第7天采用視覺模擬評分(Visual Analogue Scale,VAS)法評定[4],其中0分為無痛、1~3分為輕度疼痛,4~6分為中度疼痛,7~10分為重度疼痛。
1.5 統計學分析 采用SPSS 20.0軟件進行統計分析,計量資料以(x±s)表示,兩組均數比較采用t檢驗,計數資料的比較采用χ2檢驗,以P<0.05為差異有統計學意義。
2 結 果
兩組均無圍術期死亡病例,根治度均達到R0切除。經腹組手術時間、術中出血量、VAS評分、術后住院時間均明顯少于或低于經胸組(P<0.05),腹腔淋巴結清掃數明顯多于經胸組(P<0.05)。經腹組術后并發癥發生率為13.6%(6/44),明顯低于經胸組的31.6%(12/38)(P<0.05)。兩組縱隔淋巴結清掃數比較,差異無統計學意義(P>0.05)。見表2。
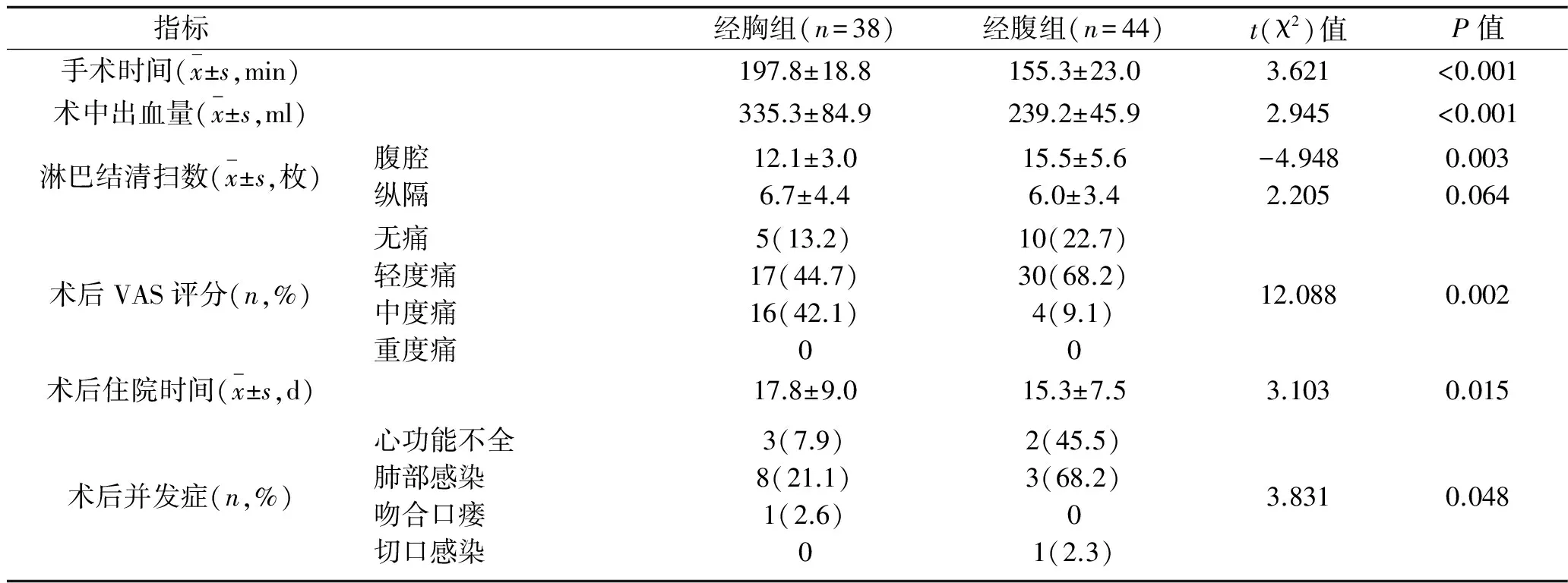
表2 經胸組和經腹組AEG患者術中及術后臨床資料比較
3 討 論
目前,AEG的Siewert分型已被國際胃癌協會和國際食管疾病學會等接受,是較為公認的分型方法[5]。由于AEG處于胸腹交界的特殊位置,特別是在Siewert Ⅱ、Ⅲ型AEG患者中,手術方式的選擇仍存在異議。
Siewert Ⅱ、Ⅲ型AEG患者通常由胸部外科或腹部外科的醫師接診。而不同科室的醫師在對疾病的認識和手術方式的選擇有不同的側重。故臨床中常用的手術徑路包括胸腹聯合、經胸和經腹3種手術入路。胸腹聯合手術入路的優勢在于可以同時便于腹部和縱隔淋巴結的清掃,但該術式創傷大,增加手術的風險。單純經胸入路常用于位置相對較高的Siewert Ⅰ型病例,便于對縱隔淋巴結進行徹底的清掃,但存在清除腹腔淋巴結相對不徹底、對心肺功能干擾大和術后恢復時間長、患者病死率高等缺點[6]。有學者報告,Siewert Ⅱ、Ⅲ型病例淋巴結轉移以腹腔轉移為主[7]。因此,經腹切口完全可以滿足其手術需要。一項隨機臨床對照研究結果顯示,經胸路徑并沒有提高Siewert Ⅱ、Ⅲ型患者總生存時間,相反增加手術死亡率[8]。
本文結果顯示,兩組患者均無圍術期死亡,根治度均達到R0切除;經腹組手術時間、術中出血量、VAS評分、術后住院時間均明顯少于或低于經胸組(P<0.05),腹腔淋巴結清掃數明顯多于經胸組(P<0.05);經腹組術后并發癥發生率明顯低于經胸組(P<0.05);兩組縱隔淋巴結清掃數比較,差異無統計學意義(P>0.05)。這說明,經腹食管裂孔入路治療Siewert Ⅱ、Ⅲ型AEG患者在根治度及縱隔淋巴結清掃上與經胸入路有相似的效果,但前者術后并發癥發生率低,而且具有以下優勢:(1)開腹迅速,損傷小;(2)對腹腔淋巴結清掃更為徹底;(3)由于對心肺功能干擾小,術后恢復快,因此住院時間縮短。而對于術前明確縱隔淋巴結轉移的病例,則需要胸部外科和普通外科醫生的相互配合,以提高病灶切除率,提高療效。
有研究表明,各型AEG均可向下轉移至腹部淋巴結,并可向上轉移至縱隔淋巴結;而對于Siewert Ⅱ、Ⅲ型AEG患者,腹部淋巴結是其主要轉移部位,常見轉移部位有賁門周圍、胃大彎、胃小彎、胃左動脈和腹腔動脈周圍,腹主動脈旁的淋巴結則更易發生轉移[5,9]。由于淋巴結轉移是影響AEG患者術后生存的獨立因素[10],而本文經腹組腹腔淋巴結清掃數明顯多于經胸組(P<0.05),提示經腹食管裂孔治療Siewert Ⅱ、Ⅲ型AEG患者的臨床療效優于經胸手術組。目前學者們對Siewert Ⅱ、Ⅲ型AEG患者的治療逐漸形成如下共識:術中淋巴結清掃均應以腹部為重點,需常規清掃賁門左右、胃小彎、腹腔動脈分支周圍淋巴結,是否行縱隔淋巴結清掃應根據腫瘤類型、分期、食管浸潤程度而定[10]。雖然本文結果顯示,兩組縱隔淋巴結清掃數比較,差異無統計學意義(P>0.05),提示經胸手術組對縱隔淋巴結的清掃并沒有明顯優勢,且患者術后恢復效率卻不及經腹組。
疼痛作為第5大生命體征,直接影響著術后患者的康復速度。過度的疼痛應激甚至會引起消化系統的嚴重并發癥,所以在不影響病情觀察的前提下,減少疼痛的發生或鎮痛治療是非常有必要的。本文結果顯示,經腹組VAS評分明顯低于經胸組(P<0.05),說明經胸組患者術后第7天的疼痛程度較經腹組嚴重,這可能是經胸組患者術后恢復較慢的重要因素。
綜上所述,對于SiewertⅡ、Ⅲ型AEG患者,經腹食管裂孔入路較經胸入路在手術時間、術中出血量、減輕術后疼痛、術后住院時間、腹腔淋巴結清掃數方面具有明顯優勢,且術后并發癥發生率更低。
[1] Siewert JR,Feith M.Adenocarcinoma of the esophagogastric junction:competition between Barrett and gastric cancer[J].J Am Coll Surg,2007,205(4 Suppl):S49-S53.
[2] Huang Q,Shi J,Sun Q,et al.Distal esophageal carcinomas in Chinese patients vary widely in histopathology,but adenocarcinomas remain rare[J].Hum Pathol,2012,43(12):2 138-2 148.
[3] Takeuchi H,Kitagawa Y.Adenocarcinoma of the esophagogastric junction:territory of the esophagus or stomach,or an independent region?[J].Ann Surg Oncol,2013,20(3):705-706.
[4] 高萬露,汪小梅.視覺模擬疼痛評分研究的進展[J].醫學研究雜志,2013,42(12):144-146.
[5] Schmidt SC,Schlechtweg N,Veltzke-Schlieker W,et al.Clinical and pathological prognostic factors for cancers of the esophagogastric junction[J].Zentralbl Chir,2009,134(5):455-461.
[6] Dresner SM,Lamb PJ,Bennett MK,et al.The pattern of metastatic lymph node dissemination from adenocarcinoma of the esophagogastric junction[J].Surgery,2001,129(1):103-109.
[7] Rüdiger Siewert J,Feith M,Werner M,et al.Adenocarcinoma of the esophagogastric junction:results of surgical therapy based on anatomical/topographic classification in 1 002 consecutive patients[J].Ann Surg,2000,232(3):353-361.
[8] Sasako M,Sano T,Yamamoto S,et al.Left thoracoabdominal approach versus abdominal-transhiatal approach for gastric cancer of the cardia or subcardia:a randomised controlled trial[J].Lancet Oncol,2006,7(8):644-651.
[9] Feith M,Stein HJ,Siewert JR.Adenocarcinoma of the esophagogastric junction:surgical therapy based on 1602 consecutive resected patients[J].Surg Oncol Clin N Am,2006,15(4):751-764.
[10]李德關,李永翔.食管胃結合部腺癌的手術治療進展[J].安徽醫學,2014,35(6):854-857.
Comparison of short-term efficacy between different operative approaches for treatment of Siewert type Ⅱ/Ⅲ adenocarcinoma of the esophao-gastric junction
SUNQi-chao1,WUPeng-fei2
(1DepartmentofThoracicSurgery,2DepartmentofGeneralSurgery,RugaoPeople′sHospital,Rugao226500,China)
Objective To compare the clinical efficacy between transabdominal surgery through esophageal hiatus and transthoracic surgery for the treatment of Siewert typeⅡ or Ⅲ adenocarcinoma of the esophao-gastric junction(AEG).Methods Eighty-two patients with Siewert type Ⅱ or Ⅲ AEG were divided into transthoracic surgery group(transthoracic group,n=38) and transabdominal surgery through esophageal hiatus group(transabdominal group,n=44) according to the surgical approach.The clinical data were compared between two groups,including intraoperative blood loss,operative time,the number of removed lymph nodes,the severity of postoperative incision pain(Visual Analogue Scale score),postoperative hospital stay and incidence of postoperative complications,ect.Results No perioperative death occurred in both groups,and the radical excision of both groups reached R0.The operation time,intraoperative blood loss,Visual Analogue Scale score and postoperative hospital stay of transabdominal group were significantly less than those of transthoracic group(P<0.05).And transabdominal group had more number of removed lymph nodes in the abdominal cavity compared to transthoracic group(P<0.05).The incidence of postoperative complications of transabdominal group was 11.4%(5/44),which was significantly lower than that of transthoracic group[31.6%(12/38)](P<0.05).There was no significant difference in the number of removed lymph nodes in the mediastinum between two groups(P>0.05).Conclusion Compared to transthoracic surgery,transabdominal surgery through esophageal hiatus for the treatment of Siewert typeⅡor Ⅲ AEG has the advantages in the number of removed lymph nodes in the abdominal cavity,and obtains lower incidence of postoperative complications.
Adenocarcinoma of the esophao-gastric junction,Siewert type Ⅱ,Siewert type Ⅲ,Surgical approach,Transabdominal,Esophageal hiatus,Transthoracic,Efficacy
江蘇省南通市市級醫學科研計劃項目(NTS2014067)
孫啟超(1987~),男,本科,住院醫師,研究方向:心胸外科。
吳鵬飛(1986~),男,碩士,住院醫師,研究方向:胃腸外科,E-mail:feifei515733887@126.com。
R 735.1
A
0253-4304(2016)02-0204-16
10.11675/j.issn.0253-4304.2016.02.03
2015-10-14
2016-01-18)
猜你喜歡
環球時報(2022-12-23)2022-12-23 09:28:37
昆明醫科大學學報(2022年1期)2022-02-28 07:45:04
中老年保健(2021年11期)2021-08-22 03:13:36
昆明醫科大學學報(2021年2期)2021-03-29 07:42:46
河北畫報(2020年10期)2020-11-26 07:20:50
小學閱讀指南·低年級版(2017年1期)2017-03-13 20:07:35
中國衛生標準管理(2015年3期)2016-01-14 03:41:47
中國醫療美容(2015年1期)2015-07-12 10:06:38
鄭州大學學報(醫學版)(2015年2期)2015-02-27 14:50:54
西南軍醫(2014年5期)2014-04-25 07:42:48
