血清半乳糖凝集素3 對胰腺癌的診斷價值
2012-11-06 07:15:22肖明兵謝玲倪溫慨陳不尤陸翠華李小彥江楓倪潤洲
中華胰腺病雜志 2012年2期
肖明兵 謝玲 倪溫慨 陳不尤 陸翠華 李小彥 江楓 倪潤洲
·論著·
血清半乳糖凝集素3 對胰腺癌的診斷價值
肖明兵 謝玲 倪溫慨 陳不尤 陸翠華 李小彥 江楓 倪潤洲
目的運用時間分解免疫熒光(TRFIA)法檢測血清半乳糖凝集素3(Galectin-3,Gal-3)水平,并探討Gal-3對胰腺癌的診斷價值。方法采用固相雙抗體夾心法建立檢測血清Gal-3的TRFIA,探討最佳實驗條件。在最適條件下檢測胰腺癌、胰腺良性占位、胰腺炎患者及健康對照者血清Gal-3水平,并聯合檢測血清CEA及CA19-9水平。結果TRFIA法檢測血清Gal-3的線性為0~100 μg/L,批內變異系數(CV)≤6.45%,批間CV≤8.68%,平均回收率為106.6%。胰腺癌患者血清Gal-3水平為4.93(0.85~23.80)μg/L,明顯高于胰腺良性占位者的2.83(2.17~4.06)μg/L、胰腺炎患者的2.62(0.55~9.76)μg/L和健康者的1.88(0.59~3.94)μg/L(P值均<0.05)。以3.77 μg/L為界,其診斷胰腺癌的敏感性為75.5%,特異性達90.9%。Gal-3與CEA及CA19-9水平均無相關性(r=0.1321,P=0.3761;r=0.0920,P=0.5384),Gal-3聯合CEA或CA19-9檢測,對胰腺癌的診斷敏感性可提高到92%。結論TRFIA法檢測血清Gal-3具有較好的敏感性和穩定性;Gal-3有望成為新的胰腺癌標記物。
胰腺腫瘤; 半乳糖凝集素3; 時間分解免疫熒光測定; 血清
目前臨床上常用的胰腺癌腫瘤標志物CA19-9和CEA的敏感性和特異性均不太高。如何提高胰腺癌早期定性診斷水平是臨床重要課題。半乳糖凝集素-3(Galectin-3,Gal-3)是半乳凝素家族的一員,能識別糖蛋白和糖脂的特異性低聚糖結構,在某些腫瘤組織中高表達[1-2],參與腫瘤細胞與血管內皮的黏附、血管生成和腫瘤免疫逃避,抑制腫瘤細胞凋亡。我們曾運用MALDI-TOF-MS技術,發現胰腺癌組織中Gal-3表達水平明顯上調[3]。但迄今國內外尚未見胰腺癌血清Gal-3的研究報道。為此,本研究檢測胰腺癌患者血清Gal-3水平,探討其對胰腺癌的診斷價值。
材料與方法
一、研究對象
收集本院2008年10月至2010年10月住院的胰腺癌患者49例,男性29例,女性20例,中位年齡67歲;胰腺良性占位患者16例,男性9例,女性7例,中位年齡45歲;急性胰腺炎患者36例,男性22例,女性14例,中位年齡53歲。所有病例均經臨床和(或)病理學證實。以體檢健康者36例作為對照,男性18例,女性18例,中位年齡20歲。均在治療前采集清晨空腹靜脈血,分離血清后立即置-80℃冰箱保存待測。
二、血清Gal-3水平檢測
采用自行建立的固相雙抗體夾心TRFIA法檢測。用包被稀釋液(0.05 mol/L碳酸鈉-碳酸氫鈉緩沖液,pH9.6,)將鼠抗人Gal-3單抗(Santa Cruz公司)稀釋至4 000 μg/L,聚苯乙烯板每孔加入100 μl 4℃包被過夜。棄包被抗體,PBS洗滌后每孔加入含10 g/L BSA的PBS封閉液200 μl/L, 37℃孵育1 h。棄封閉液,洗滌后每孔分別加入系列稀釋的Gal-3標準蛋白(ABR公司)、待測血清樣本50 μl,以單加封閉液為空白對照,37℃孵育1 h。洗滌后加入生物素化羊抗人Gal-3多抗100 μl(80 μg/L,Santa Cruz公司)37℃孵育1 h。洗滌后每孔加入用含10 g/L BSA的PBS稀釋的稀土離子(Eu3+)-標鏈親和素100 μl(600 μg/L,PE公司)37℃避光孵育1 h。洗滌后每孔加入熒光增強液200 μl(PE公司),室溫避光緩慢水平搖動5 min。在VICTORTM X5型自動時間分辨熒光檢測儀上設定。激發光波長為337 nm,發射光波長為615 nm,延時200 μs,測定615 nm處的熒光值(A615值)。以Gal-3標準蛋白的熒光值繪制標準曲線,根據樣品的熒光值計算Gal-3的濃度。
三、血清CEA和CA19-9水平檢測
采用化學發光免疫檢測法,檢測試劑盒購自美國雅培公司,按說明書操作。
四、統計學處理
采用Stata8.0及SPSS15.0統計軟件進行分析。血清Gal-3、CEA及CA19-9值用中位數表示,各組間的差異采用秩和檢驗;率的比較采用χ2檢驗,當理論頻數小于5時,采用Fisher′s確切概率法;血清Gal-3、CEA及CA19-9三者間的相關分析采用Spearman等級相關方法。界值的確定用受試者工作特征曲線(ROC)。P<0.05為差異具有統計學意義。
結 果
一、Gal-3檢測最適條件的確立
將抗Gal-3單抗、生物素化的羊抗人Gal-3多抗及Eu3+-標鏈親和素分別系列稀釋,以12.5 μg/L的Gal-3標準蛋白為陽性對照,封閉液為陰性對照,設3個復孔,讀取各孔熒光值。當抗Gal-3單抗、多抗及Eu3+-標鏈親和素濃度分別為4000、80及600 μg/L時,陽性對照與陰性對照平均熒光值之比(P/N值)最大(8.05),為最適工作濃度。
二、檢測方法學評價
將Gal-3標準蛋白系列稀釋,以上述最適條件測定,在0.78~100 μg/L范圍內成線性關系(圖1)。
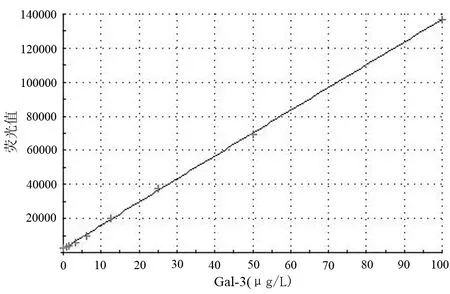
圖1 GAL-3 檢測劑量-反應曲線圖
將Gal-3標準蛋白稀釋至0 μg/L附近,作為檢測零點樣品,重復測量20次,計算其熒光均值及標準差。以熒光均值加上2倍的標準差所得的熒光值代入標準曲線方程計算得出的濃度為其最低檢測量。本法靈敏度為0.181 μg/L。
將Gal-3標準蛋白稀釋成3.13、6.25、12.5 μg/L作為質控樣品,分三批次進行測定,每批次各設8個復孔,批內變異系數(CV)≤6.45%,批間CV≤8.68%(表1)。
取3份胰腺癌患者血清混合,配制兩份Gal-3濃度為12.5 μg/L及3.1 μg/L的標準品,按下法配制試驗樣品:基礎樣品為血清0.9 ml加蒸餾水0.1 ml;分析樣品為血清0.9 ml加標準品(12.5 μg/L或3.1 μg/L)0.1 ml。按上述最適條件測定,每份樣品設8個復孔,求均值。兩分析樣品回收濃度分別為1.29、0.34 μg/L,回收率分別為103.5%及109.7%,平均回收率為106.6%。
三、血清Gal-3、CEA、CA19-9水平及三者間相關分析
因Gal-3、CEA及CA19-9水平均呈偏態分布,故以中位數表示。胰腺癌患者血清Gal-3、CEA及CA19-9水平均明顯高于其他各組(表2,P值均<0.05)。

表1 不同濃度Gal-3各批次的熒光值

表2 各組血清Gal-3、CEA及CA19-9水平(中位數,范圍)
注:經秩和檢驗,a與其他各組比,Z值分別為3.778、4.874及6.379,P值分別為0.0002、0.0000及0.0000;b與其他各組比,Z值分別為4.723、4.839及5.898,P值均為0.0000;c與其他各組比,Z值分別為3.007、3.508及3.899,P值分別為0.0026、0.0005及0.0001
根據ROC曲線(圖2),Gal-3、CEA及CA19-9對良、惡性胰腺疾病的診斷界值分別為3.77 μg/L、3.82 μg/L及41.61 kU/L,診斷胰腺癌的敏感性在70%左右,特異性在90%以上(表3)。Gal-3與CEA、CA19-9之間無相關性(r=0.1321,P=0.3761;r=0.0920,P=0.5384),而CEA與CA19-9之間呈正相關(r=0.3982,P=0.0056)。Gal-3聯合CA19-9或Gal-3聯合CEA檢測可明顯提高對胰腺癌的診斷敏感性,以Gal-3+CA19-9略優于Gal-3+CEA,但兩者無明顯差異(表3)。
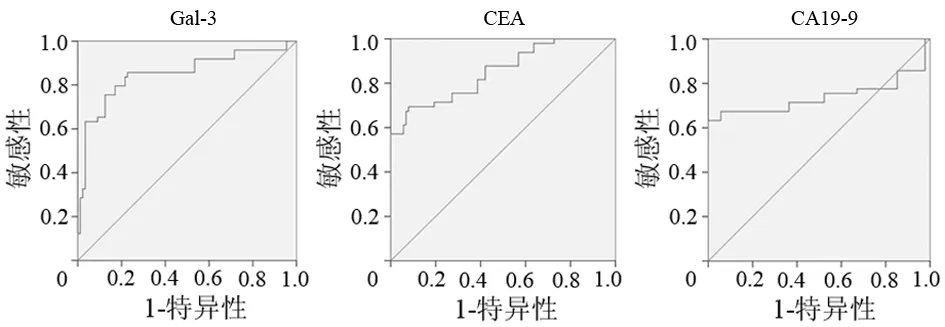
圖2 Gal-3、CEA及CA19-9診斷胰腺癌的ROC曲線
Gal-3是一種糖結合蛋白,分子質量約30 000,對β-半乳糖苷具有親和性。上皮細胞、血管內皮細胞[4]、活化的巨噬細胞[5]及樹突狀細胞等[6]均表達Gal-3,它在細胞質內合成,但可以運到胞核或分泌到細胞外,參與不同的生物過程。Gal-3在多種腫瘤中高表達,如結直腸癌[7]、胃癌[8]、肝癌[9]、甲狀腺癌[10]、垂體腺瘤[10]、腎透明細胞癌[11]、浸潤性乳腺癌[12]、舌鱗狀細胞癌[13]、惡性嗜鉻細胞瘤[2]、上皮性卵巢癌[14]、膀胱癌[15]等,其表達的增加與腫瘤的轉移和疾病進展呈正相關。
TRFIA技術利用3價稀土離子(Eu3+)代替熒光物質、放射性核素或酶為示蹤物,標記抗體、抗原、激素、多肽、蛋白質、核酸探針及生物細胞,抗原抗體反應后用檢測儀測定反應產物中的熒光強度,判斷分析物濃度。檢測系統可實現全部自動化,同時利用波長和時間兩種分辨有效地排除了非特異熒光,大大提高了分析靈敏度。具有操作簡便、靈敏度高、不受樣品自然熒光干擾、示蹤物穩定、標準曲線范圍寬、無放射性污染、標記物存儲時間長等優點[16]。本研究建立的血清Gal-3的TRFIA檢測法,具有分析線性范圍寬、靈敏度高、重復性及回收率好等特點,符合臨床體外診斷試劑檢測的要求。

表3 Gal-3聯合CEA及CA19-9檢測診斷胰腺癌的價值
本研究結果顯示,胰腺癌患者血清Gal-3明顯高于健康人及良性胰腺疾病患者,其診斷胰腺癌的敏感性與CA19-9及CEA相仿,且與CEA及CA19-9均無相關性。Gal-3聯合CEA或CA19-9檢測。可提高診斷敏感性,表明Gal-3對胰腺癌的診斷具有較好的臨床價值。
[1] Htwe TT, Karim N, Wong J, et al. Differential expression of galectin-3 in advancing thyroid cancer cells: a clue toward understanding tumour progression and metastasis. Singapore Med J,2010,51:856-859.
[2] Saffar H, Sanii S, Heshmat R, et al. Expression of galectin-3, nm-23, and cyclooxygenase-2 could potentially discriminate between benign and malignant pheochromocytoma. Am J Clin Pathol, 2011,135:454-460.
[3] Chen JH, Ni RZ, Xiao MB, et al. Comparative proteomic analysis of differentially expressed proteins in human pancreatic cancer tissue. Hepatobiliary Pancreat Dis Int, 2009,8:193-200.
[4] Khaldoyanidi SK, Glinsky VV, Sikora L, et al. MDA-MB-435 human breast carcinoma cell homo-and heterotypic adhesion under flow conditions is mediated in part by Thomsen-Friedenreich antigengalectin-3 interactions.J Biol Chem, 2003, 278:4127-4134.
[5] Kim K, Mayer EP, Nachtigal M. Galectin-3 expression in macrophages is signaled by Ras/MAP kinase pathway and up-regulated by modified lipoproteins.Biochim Biophys Acta, 2003, 1641:13-23.
[6] Vray B, Camby I, Vercruysse V, et al. Up-regulation of galectin-3 and its ligands by Trypanosoma cruzi infection with modulation of adhesion and migration of murine dendritic cells. Glycobiology, 2004, 14:647-657.
[7] Zaia Povegliano L, Oshima CT, de Oliveira Lima F, et al. Immunoexpression of galectin-3 in colorectal cancer and its relationship with survival. J Gastrointest Cancer, 2011,42:217-221.
[8] Okada K, Shimura T, Suehiro T, et al. Reduced galectin-3 expression is an indicator of unfavorable prognosis in gastric cancer. Anticancer Res, 2006, 26:1369-1376.
[9] Matsuda Y, Yamagiwa Y, Fukushima K, et al. Expression of galectin-3 involved in prognosis of patients with hepatocellular carcinoma. Hepatol Res, 2008, 38:1098-1111.
[10] Righi A, Jin L, Zhang S, et al. Identification and consequences of galectin-3 expression in pituitary tumors. Mol Cell Endocrinol, 2010, 326:8-14.
[11] Sakaki M, Fukumori T, Fukawa T, et al. Clinical significance of Galectin-3 in clear cell renal cell carcinoma. J Med Invest, 2010, 57:152-157.
[12] Koo JS, Jung W. Clinicopathlogic and immunohistochemical characteristics of triple negative invasive lobular carcinoma. Yonsei Med J, 2011, 52:89-97.
[13] Alves PM, Godoy GP, Gomes DQ, et al. Significance of galectins-1, -3, -4 and -7 in the progression of squamous cell carcinoma of the tongue. Pathol Res Pract, 2011, 207:236-240.
[14] Kim MK, Sung CO, Do IG, et al. Overexpression of Galectin-3 and its clinical significance in ovarian carcinoma. Int J Clin Oncol, 2011, 16:352-358.
[15] Canesin G,Gonzalez-Peramato P,Palou J,et al.Galectin-3 expression is associated with bladder cancer progression and clinical outcome.Tumour Biol,2010,31:277-285.
[16] Andoh T, Nagasawa H. Development of a time-resolved fluoroimmunoassay for insulins and its application to monitoring of insulin secretion induced by feeding in the barfin flounder, Verasper moseri. Gen Comp Endocrinol, 2002, 125:365-374.
Dignosisvalueofserumglypican-3forpancreascancer
XIAOMing-bing,XIELin,NIWen-kai,CHENBu-you,LUCui-hua,LIXiao-yan,JIANGFeng,NIRun-zhou.
DepartmentofGastroenterology,AffiliatedHospitalofNantongUniversity,Nantong226001,China
NIRun-zhou,Email:nirz@163.com
ObjectiveTo establish the time-resolved fluoroimmunoassay (TRFIA) method for the detection of serum galectin-3 and investigate the clinical value of serum galectin-3 for the diagnosis of pancreas cancer.MethodsMonoclonal anti-human galectin-3 antibody and biotinylated polyclonal antibody were used to establish the sandwich TRFIA for detection of serum galectin-3. The optimal experimental condition was studied. Serum levels of galectin-3, CEA and CA19-9 in the patients with pancreatic cancer, benign pancreatic mass, pancreatitis, and healthy controls were measured. The diagnostic value of serum galectin-3, CEA and CA19-9 for pancreas cancer was studied.ResultsThe linearity of the TRFIA for detection of serum galectin-3 ranged between 0 to 100 μg/L. The within-run CV and between-run CV were ≤6.45% and ≤8.68%, respectively, and the average recovery was 106.6%. The level of serum galectin-3 was 4.93(0.85~23.80)μg/L in pancreatic cancer group, which were significantly higher than those in benign pancreatic mass [2.83(2.17~4.06)μg/L], pancreatitis [2.62(0.55~9.76)μg/L], and healthy controls group [1.88(0.59~3.94)μg/L](P<0.05). By using 3.77 μg/L as the cut-off point, the sensitivity, specificity for the diagnosis of pancreatic cancer was 75.5% and 90.9%. The levels of Gal 3 and CEA, CA19-9 was not correlated (r=0.1321,P=0.3761;r=0.0920,P=0.5384). Combined determination of galactin-3 and CEA, CA19-9 levels could increase the diagnostic sensitivity to 92%.ConclusionsTRFIA method for the detection of galactin-3 is sensitive and stable. Galectin-3 could be a potentially novel serum tumor marker of pancreatic cancer.
Pancreatic neoplasms; Galectin-3; Time-resolved fluoroimmunoassay; Serum
10.3760/cma.j.issn.1674-1935.2012.02.001
江蘇省“六大人才高峰”資助項目(2006073);江蘇省衛生廳資助項目(H200923);南通市科技計劃資助項目(S2010012)
226001 南通,南通大學附屬醫院消化內科
倪潤洲,Email: nirz@163.com
2011-06-12)
(本文編輯:屠振興)
猜你喜歡
美與時代·美術學刊(2022年3期)2022-04-27 01:18:15
中學生數理化·七年級數學人教版(2021年6期)2021-11-22 07:50:58
中學生數理化·七年級數學人教版(2021年6期)2021-11-22 07:50:58
中學生數理化·七年級數學人教版(2021年6期)2021-11-22 07:50:58
中老年保健(2021年3期)2021-08-22 06:50:04
天津醫科大學學報(2021年2期)2021-03-29 05:31:08
現代臨床醫學(2021年1期)2021-01-26 00:56:02
人大建設(2019年12期)2019-05-21 02:55:32
海峽科技與產業(2016年3期)2016-05-17 04:32:12
現代檢驗醫學雜志(2014年4期)2014-02-02 02:44:59
