蛋白S缺乏癥的PROS1基因突變并臨床異質性表現一例
2023-11-13 20:21:08魏欣雨王娟譚榜云李子堅
中國醫學科學院學報 2023年5期
關鍵詞:突變
魏欣雨 王娟 譚榜云 李子堅
摘要:蛋白S活性降低是靜脈血栓栓塞的高危因素之一。遺傳性蛋白S缺乏癥是由PROS1基因突變引起的常染色體顯性遺傳病。本文報道1例PROS1基因突變的女性患者,測序發現在PROS1基因第3外顯子中c.292 G>T。譜系分析顯示該突變可能源自于患者的母親。經查詢PROS1基因突變數據庫及文獻檢索,證實這個突變為國際首次報道。
關鍵詞:突變;PROS1;蛋白S缺乏癥
中圖分類號: R559? 文獻標志碼: B? 文章編號:1000-503X(2023)05-0863-04
DOI:10.3881/j.issn.1000-503X.15541
PROSI Mutation With Clinical Heterogeneity in Protein S Deficiency:Report of One Case
WEI Xinyu1,WANG Juan1,TAN Bangyun2,LI Zijian1,3
1First Clinical Medical College of Lanzhou University,Lanzhou 730000,China
2Department of Laboratory,3Department of Hematology,The First Hospital of Lanzhou University,Lanzhou 730000,China
Corresponding author:LI Zijian? Tel:0931-8356912,E-mail:ldyy_lizj@lzu.edu.cn
ABSTRACT:Reduced protein S activity is one of the high-risk factors for venous thromboembolism.Hereditary protein S deficiency is an autosomal dominant disorder caused by mutations in the PROS1 gene.We reported a female patient with a mutation of c.292 G>T in exon 3 of the PROS1 gene,which was identified by sequencing.The genealogical analysis revealed that the mutation probably originated from the patients mother.After searching against the PROS1 gene mutation database and the relevant literature,we confirmed that this mutation was reported for the first time internationally.
Key words:mutation;PROS1;protein S deficiency
Acta Acad Med Sin,2023,45(5):863-866
蛋白S是由肝細胞產生的維生素K依賴性糖蛋白,在抗凝過程中起重要作用[1]。蛋白S作為活化蛋白C的輔助因子,參與活化凝血因子Ⅴ和Ⅷ的降解途徑,此外,其通過與C4b結合蛋白結合在補體途徑中發揮作用[2]。遺傳性蛋白S缺乏癥(protein S deficiency,PSD)是導致亞洲人群靜脈血栓栓塞(venous thromboembolism,VTE)的常見因素[3]。PSD通常是由蛋白S基因PROS1突變引起。PROS1基因位于第3號常染色體長臂(3q11.2),總長度約為101 kbp,由15個外顯子和14個內含子組成[4]。截至2023年1月,人類基因突變數據庫(human gene mutation database,HGMD)收錄505種PROS1基因變異。本文報道1例深靜脈血栓形成的PSD患者,其PROS1基因存在雜合突變(c.292 G>T),此突變系國際首次報道。
臨床資料
患者女,20歲,主訴“黑便伴腹痛4 d”,于2021年7月就診于蘭州大學第一醫院急診科。腹部增強CT示門靜脈主干、腸系膜上靜脈及其分支和脾靜脈內血栓形成,伴絞窄性腸梗阻,故行小腸部分切除術及術后低分子量肝素抗凝治療,出院后改為口服利伐沙班抗凝預防血栓形成。易栓癥篩查結果顯示蛋白S活性0.23(參考值范圍0.76~1.35),蛋白C 1.10,抗凝血酶0.93。
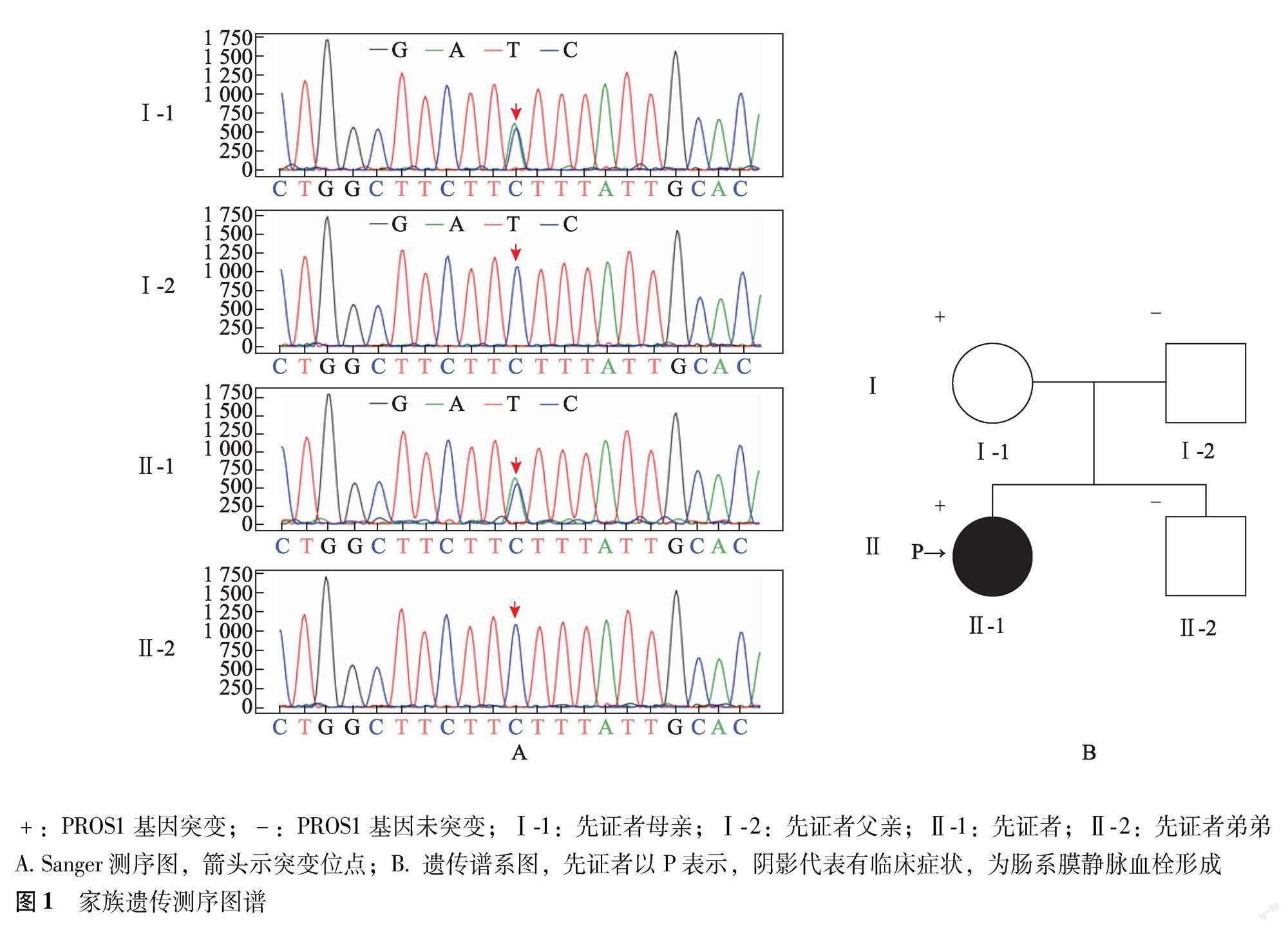
患者行下一代測序和Sanger測序鑒定出1個新的PROS1基因雜合突變(c.292 G>T)。采用Sanger測序在直系親屬和兄弟中驗證突變,結果顯示在先證者(Ⅱ-1)和母親(Ⅰ-1)中發現PROS1基因c.292 G>T突變,其父親(Ⅰ-2)和兄弟(Ⅱ-2)中未發現突變(圖1A)。家族史回顧顯示,患者父母和弟弟均未出現相關臨床表型(圖1B)。患者母親蛋白S活性0.475(參考值范圍0.635~1.490),蛋白C 1.02(參考值范圍0.70~1.40)。
先證者在來自chr3:93646132(基因組版本:hg19)的轉錄本NM_001314077的第3外顯子中發現PROS1基因292位點堿基G突變為T。查詢HGMD專業版數據庫(http://www.hgmd.org)、Clinvar數據庫(https://www.ncbi.nlm.nih.gov/clinvar)、基因組聚集數據庫(https://gnomad.broadinstitute.org)東亞人群中均無收錄。采用SIFT和Polyphen-2軟件無法預測該位點蛋白結構。Mutation Taster致病性預測軟件(http://www.mutationtaster.org)預測該突變致病性為A級(評分1分)。根據美國醫學遺傳學與基因組學學會相關指南[5],將c.292 G>T評級為可能致病變異(PVS1+PM2_Supporting)。
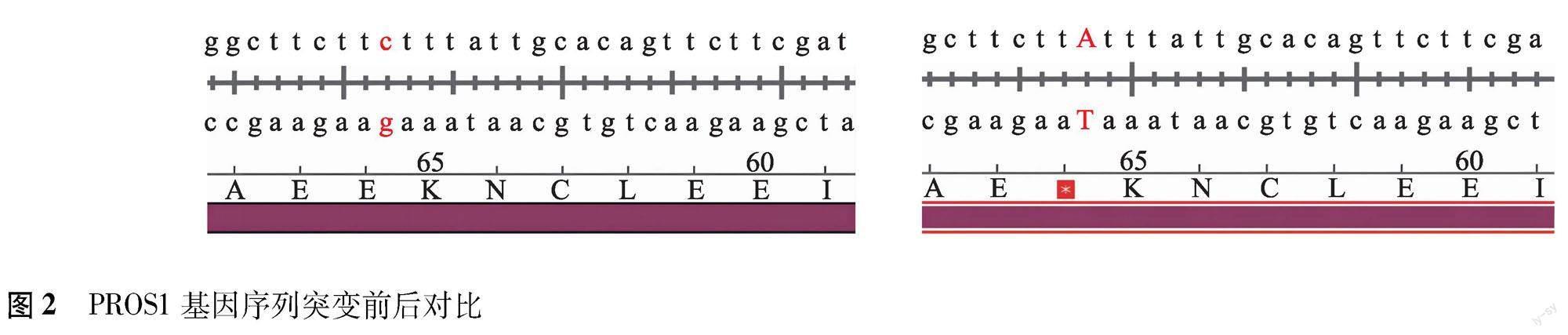
根據測序報告,在美國國家生物技術信息中心網站(https://www.ncbi.nlm.nih.gov)尋找chr3:93646132位點,獲得基因組比對結果。下載第1個序列的Genbank文件導入SnapGene軟件分析。雜合突變c.292 G>T對應基因編碼序列第65位密碼子從野生型編碼谷氨酸的GAA(圖2A)突變為TAA(圖2B),而TAA為終止密碼子,突變后的蛋白質翻譯提前終止,導致PROS1基因無法編碼正常功能的蛋白質。
討論
本研究報道1例臨床表現為深靜脈血栓并攜帶PROS1基因突變的女性患者。遺傳性易栓癥存在顯著的種族差異,亞洲地區人群以抗凝蛋白缺陷為主,包括抗凝血酶缺乏癥、蛋白C缺乏癥、PSD等[6]。PROS1基因突變常引起蛋白S活性和功能發生改變,其基因突變譜在中國、日本和韓國人群中有所差異[7]。一些針對中國PSD家系的研究總結了中國人群PSD的臨床特征,并報道了一些新的突變位點。Tang等[8]研究發現華中地區40例PSD血栓性疾病患者中的20種不同PROS1基因突變,其中包括15種新突變。Li等[9]研究中國53個不相關PSD家系,在48例先證者中檢測到36種PROS1基因突變,包括16種新突變,并首次發現3個熱點突變(Glu67Ala、Arg561Trp和Tyr560)。Zhang等[10]發現一種HGMD未收錄的新型PROS1基因突變,提示PROS1基因突變的多樣性。
本例患者及其母親均攜帶PROS1基因突變,且蛋白S活性降低,然而只有患者出現VTE,提示本例為常染色體顯性遺傳病,PROS1基因突變可引起蛋白S活性降低,但不一定發生易栓癥。基因-環境相互作用學說解釋了在特定環境條件下基因與環境共同影響了特定患者血栓形成的發生與發展[11]。目前建議VTE的風險評估應綜合生物標志物識別、基因篩選和多種危險因素分析,而不是簡單地歸因于某種單一因素[12]。
常見引起VTE的危險因素包括手術創傷、口服避孕藥、激素替代、妊娠、惡性腫瘤、感染和某些炎癥狀態等[13-15]。本例患者無相關危險因素,但體重指數(body mass index,BMI)為30.9 kg/m2,其母親BMI為22.5 kg/m2。研究發現,BMI過高不僅是有基礎病患者血栓形成的危險因素,在正常人群中也會增加血栓形成的風險[16-17]。肥胖作為VTE的危險因素之一,與靜脈淤血、靜脈系統內皮細胞損傷和血液高凝狀態等多種因素相關。對于肥胖癥患者,高腹內壓和股靜脈低血流速率會增加靜脈回流受阻的風險,從而促進深靜脈血栓形成[13]。Gregson等[18]研究表明不同的肥胖標志物(BMI、腰臀比和腰圍)與血栓發生呈正相關。BMI>30 kg/m2者血栓發病率為2.01/1000[19],顯著高于BMI正常人群[20]。此外,腹型肥胖者(腰圍男性>94 cm,女性>80 cm)與血栓發生關系更密切[21],腰圍可作為預測血栓疾病的獨立危險因素。肥胖人群BMI每增加10 kg/m2,血栓復發的風險增加24%[22]。此外,VTE的風險因素還與性別有關,與男性相比,人體肥胖指數(包括體重、BMI、腰圍、臀圍、脂肪百分比等)對女性VTE影響更大[23]。本例患者及其母親都有PSD遺傳學異常及蛋白S活性減低,而肥胖可能誘發血栓形成,導致不同的臨床表型。
綜上,本研究結果表明PROS1基因突變譜的多樣性和臨床表型的異質性,VTE的發生受到基因、性別、BMI等多種因素的影響。對于無明顯誘因但蛋白S活性測定異常的VTE患者,建議對患者及親屬進行PROS1基因測序,以便及時發現可能的致病突變。
參考文獻
[1]Castoldi E,Hackeng TM.Regulation of coagulation by protein S[J].Curr Opin Hematol,2008,15(5):529-536.DOI:10.1097/MOH.0b013e328309ec97.
[2]Teraz-Orosz A,Gierula M,Petri A,et al.Laminin G1 residues of protein S mediate its TFPI cofactor function and are competitively regulated by C4BP[J].Blood Adv,2022,6(2):704-715.DOI:10.1182/bloodadvances.2021005382.
[3]Jin X,Kinoshita S,Kuma H,et al.Reduced activity of protein S in plasma:a risk factor for venous thromboembolism in the Japanese population[J].Clin Appl Thromb Hemost,2021,27:10760296211033908.DOI:10.1177/10760296211033908.
[4]García de Frutos P,Fuentes-Prior P,Hurtado B,et al.Molecular basis of protein S deficiency[J].Thromb Haemost,2007,98(3):543-556.
[5]中華醫學會血液學分會血栓與止血學組.易栓癥診斷與防治中國指南(2021年版)[J].中華血液學雜志,2021,42(11):881-888.DOI:10.3760/cma.j.issn.0253-2727.2021.11.001.
[6]Richards S,Aziz N,Bale S,et al.Standards and guidelines for the interpretation of sequence variants:a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology[J].Genet Med,2015,17(5):405-424.DOI:10.1038/gim.2015.30.
[7]Zhu T,Ding Q,Bai X,et al.Normal ranges and genetic variants of antithrombin,protein C and protein S in the general Chinese population.Results of the Chinese hemostasis investigation on natural anticoagulants study I group[J].Haematologica,2011,96(7):1033-1040.DOI:10.3324/haematol.2010.037515.
[8]Tang L,Jian XR,Hamasaki N,et al.Molecular basis of protein S deficiency in China[J].Am J Hematol,2013,88(10):899-905.DOI:10.1002/ajh.23525.
[9]Li L,Wu X,Wu W,et al.Clinical manifestation and mutation spectrum of 53 unrelated pedigrees with protein S deficiency in China[J].Thromb Haemost,2019,119(3):449-460.DOI:10.1055/s-0038-1677031.
[10]Zhang Y,Yang H,Chen Q,et al.A novel PROS1 mutation,c.74dupA,was identified in a protein S deficiency family[J].Thromb Res,2016,148:125-127.DOI:10.1016/j.thromres.2016.11.003.
[11]Rosendaal FR.Venous thrombosis:a multicausal disease[J].Lancet,1999,353(9159):1167-1173.DOI:10.1016/s0140-6736(98)10266-0.
[12]Albertsen IE,Piazza G,Goldhaber SZ.Lets stop dichotomizing venous thromboembolism as provoked or unprovoked[J].Circulation,2018,138(23):2591-2593.DOI:10.1161/CIRCULATIONAHA.118.036548.
[13]Vilahur G,Ben-Aicha S,Badimon L.New insights into the role of adipose tissue in thrombosis[J].Cardiovasc Res,2017,113(9):1046-1054.DOI:10.1093/cvr/cvx086.
[14]Barcellona D,Marongiu F,Grandone E.Contraceptives and thrombosis:an intertwined revolutionary road[J].Semin Thromb Hemost,2023.DOI:10.1055/s-0043-1764382.
[15]Pastori D,Cormaci VM,Marucci S,et al.A comprehensive review of risk factors for venous thromboembolism:from epidemiology to pathophysiology[J].Int J Mol Sci,2023,24(4):3169.DOI:10.3390/ijms24043169.
[16]Morange PE,Alessi MC.Thrombosis in central obesity and metabolic syndrome:mechanisms and epidemiology[J].Thromb Haemost,2013,110(4):669-680.DOI:10.1160/TH13-01-0075.
[17]Iglesias Morcillo M,Freuer D,Peters A,et al.Body mass index and waist circumference as determinants of hemostatic factors in participants of a population-based study[J].Medicina(Kaunas),2023,59(2):228.DOI:10.3390/medicina59020228.
[18]Gregson J,Kaptoge S,Bolton T,et al.Cardiovascular risk factors associated with venous thromboembolism[J].JAMA Cardiol,2019,4(2):163-173.DOI:10.1001/jamacardio.2018.4537.
[19]Tsai AW,Cushman M,Rosamond WD,et al.Cardiovascular risk factors and venous thromboembolism incidence:the longitudinal investigation of thromboembolism etiology[J].Arch Intern Med,2002,162(10):1182-1189.DOI:10.1001/archinte.162.10.1182.
[20]Caiano LM,Costanzo S,Panzera T,et al.Association between body mass index,waist circumference,and relative fat mass with the risk of first unprovoked venous thromboembolism[J].Nutr Metab Cardiovasc Dis,2021,31(11):3122-3130.DOI:10.1016/j.numecd.2021.07.018.
[21]Yuan S,Bruzelius M,Xiong Y,et al.Overall and abdominal obesity in relation to venous thromboembolism[J].J Thromb Haemost,2021,19(2):460-469.DOI:10.1111/jth.15168.
[22]Kernan WN,Inzucchi SE,Sawan C,et al.Obesity:a stubbornly obvious target for stroke prevention[J].Stroke,2013,44(1):278-286.DOI:10.1161/STROKEAHA.111.639922.
[23]Brink A,Elf J,Svensson PJ,et al.Sex-specific risk factors for deep venous thrombosis and pulmonary embolism in a population-based historical cohort study of middle-aged and older individuals[J].J Am Heart Assoc,2023,12(5):e027502.DOI:10.1161/JAHA.122.027502.
(收稿日期:2023-02-23)
猜你喜歡
中國現代醫生(2017年4期)2017-04-26 09:34:35
中國醫藥科學(2016年20期)2017-03-15 19:46:37
農業與技術(2016年20期)2016-12-08 21:34:56
體育教學(2016年10期)2016-12-01 00:16:53
考試周刊(2016年76期)2016-10-09 09:47:35
江蘇農業科學(2016年4期)2016-06-14 01:38:13
環球時報(2015-06-25)2015-06-25 19:30:56
安徽農學通報(2015年10期)2015-06-15 02:32:43
湖北農業科學(2014年22期)2015-01-20 11:21:07
江蘇農業科學(2014年11期)2015-01-15 12:13:21
