Appendiceal bleeding: A case report
2022-06-27 08:30:48ShengYueZhouMaoDongGuoXiaoHuaYe
World Journal of Clinical Cases 2022年18期
關(guān)鍵詞:水質(zhì)
lNTRODUCTlON
The common causes of lower gastrointestinal bleeding are mostly known to be diseases of the colon,rectum, and terminal ileum[1]. However, appendiceal bleeding as the origin is extremely rare.Diverticulum, angiodysplasia, inflammation, and neoplasm are the usual etiologies for appendiceal bleeding[2,3]. Vascular diseases, such as angiodysplasia and Dieulafoy’s lesion, are one of the most common causes of massive bleeding and sometimes can be life-threatening[1,4]. We report herein a case of lower gastrointestinal bleeding due to appendiceal Dieulafoy’s lesion, with a literature review.
CASE PRESENTATlON
Chief complaints
The patient had been previously diagnosed with hemorrhoids and hypertension, but was taking no medications.
History of present illness
The patient reported having experienced approximately 600-800 mL bloody stools before presentation to the hospital. The patient also reported having experienced loss of consciousness for a few seconds.No other gastrointestinal symptoms, such as nausea, vomiting, or abdominal pain, were experienced during the process. The patient denied past history of hematochezia.
History of past illness
A 32-year-old male presented to the emergency department of our hospital with hematochezia that had lasted for 6 h.
Personal and family history
The authors declare that they have no conflict of interest.
Physical examination
The patient’s temperature was 36.5 °C, heart rate was 95 beats per minute, respiratory rate was 20 breaths per minute, blood pressure (measured with electronic cuff) was 147/105 mmHg, and oxygen saturation in room air was 99%. The physical examination showed an anemic appearance, without any other pathological signs.
Laboratory examinations
The laboratory tests showed that hemoglobin was 102 g/L (normal range: 130-175 g/L), revealing a mild anemia. Other routine relevant examinations, such as platelet counts and for markers of coagulation function, and liver and renal function, yielded normal findings. Unfortunately, the patient passed bloody stools again 1 d after conservative treatment in our department, with his hemoglobin level dropping to 86 g/L.
Imaging examinations
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
根據(jù)以上數(shù)據(jù)驗(yàn)證,丁辛醇裝置汽提廢水水質(zhì)較好,符合循環(huán)水水質(zhì)要求。在實(shí)際運(yùn)行中丁辛醇裝置汽提廢水回用于循環(huán)冷卻水的難度主要在于:在剛開工不穩(wěn)定階段,COD波動(dòng)較大,不利于微生物的控制。對(duì)此我們應(yīng)在剛開工不穩(wěn)定階段將丁辛醇汽提廢水切出系統(tǒng),并不斷監(jiān)測(cè)丁辛醇汽提廢水水質(zhì),待水質(zhì)各項(xiàng)指標(biāo)穩(wěn)定后方可切入循環(huán)水系統(tǒng)[3]。
FlNAL DlAGNOSlS
從理論計(jì)算和實(shí)驗(yàn)研究結(jié)果看,超高速動(dòng)能武器對(duì)地打擊效應(yīng)與已有常規(guī)鉆地彈差異很大,集中體現(xiàn)在侵徹深度趨近極限、成坑效應(yīng)和地沖擊效應(yīng)顯著等方面。目前對(duì)超高速動(dòng)能武器的防護(hù)尚缺乏成熟的設(shè)計(jì)規(guī)范,文獻(xiàn)[20]提出了一種“硬-軟-硬分層配置”的遮彈防護(hù)結(jié)構(gòu)方案,通過數(shù)值模擬計(jì)算,驗(yàn)證了方案的可行性。本文在該遮彈防護(hù)結(jié)構(gòu)方案的基礎(chǔ)上,提出了4種靶體分層設(shè)計(jì)優(yōu)化方案,稱為“軟硬結(jié)合、分層配置”。
TREATMENT
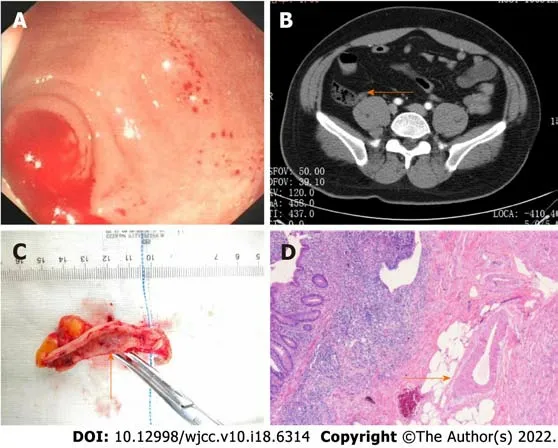
We suspected that the source of bleeding was the appendix, which prompted an emergency laparoscopic appendectomy. During that surgery, no signs of acute appendicitis or diverticulitis were observed; however, a large amount of blood clots was observed through the longitudinal incision of the appendix. A vessel stump was also found on the mucosa of the appendix (Figure 1C). Pathologically, a caliber-persistent artery was detected near the vessel stump of the mucosa surface, corresponding to Dieulafoy’s lesion within the appendix (Figure 1D).
OUTCOME AND FOLLOW-UP
The patient had no recurrent hematochezia or melena, and was discharged from the hospital 6 d after the surgery. Follow-up 2 wk later showed no evidence of rebleeding.
PCR反應(yīng)體系采用康為公司提供的Mix 50 μL。擴(kuò)增程序參考汪琛穎等[8]的方法。擴(kuò)增產(chǎn)物經(jīng)含EB核酸染料的2%瓊脂糖凝膠電泳(電壓為80 V)檢測(cè)后,應(yīng)用全自動(dòng)數(shù)碼凝膠成像分析系統(tǒng)(Tanon 2500)進(jìn)行觀察、拍照。
DlSCUSSlON
Several modalities, such as colonoscopy, contrast-enhanced abdominal CT, and angiography, can be applied in diagnosing appendiceal bleeding[2,3,9]. In our case, colonoscopy directly revealed the active bleeding from the appendiceal orifice. For such cases, emergency colonoscopy for acute lower gastrointestinal bleeding should be utilized, at least to the terminal ileum. In addition, the orifice of the appendix should be carefully observed. Contrast-enhanced abdominal CT is useful in evaluating diverticulum, neoplasm, or acute inflammation. Although mesenteric artery angiography requires bleeding of more than 0.5 mL/min, vessel embolization is feasible in controlling acute bleeding[9].
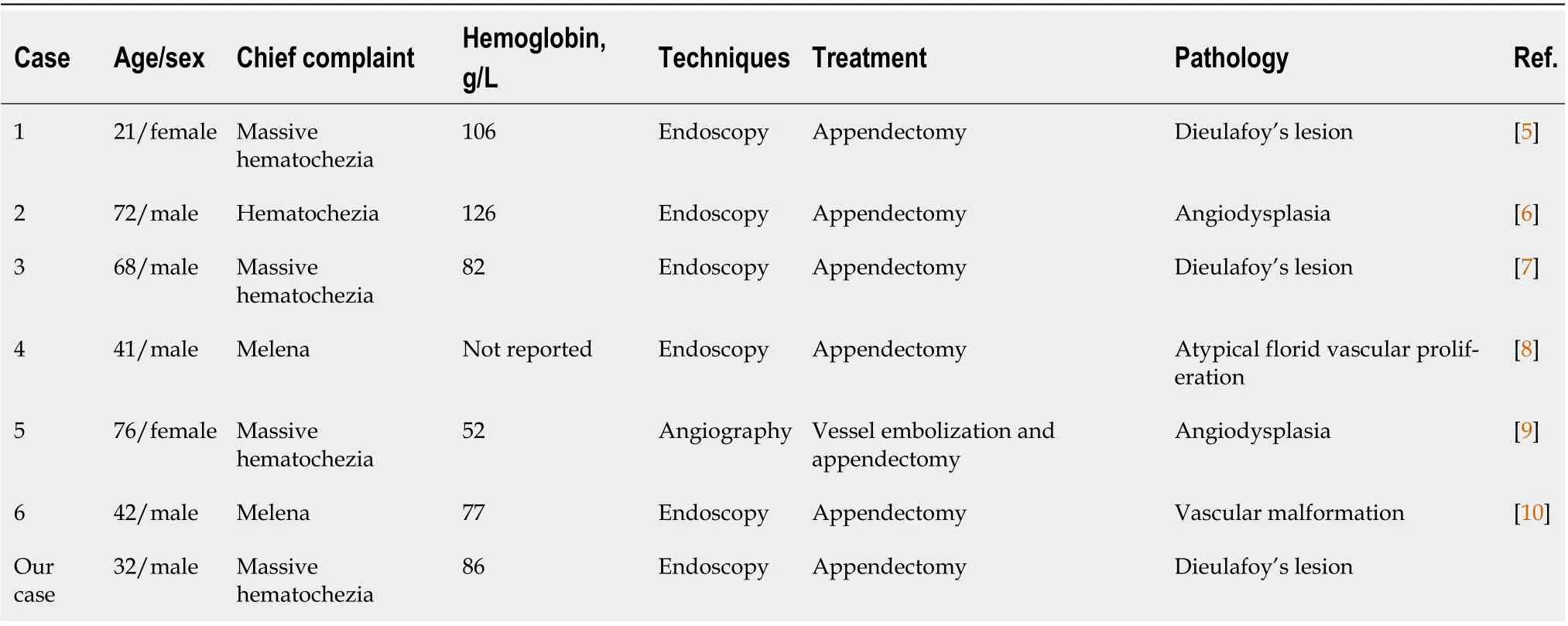
The average age of the included cases was 50.3 years (range: 21-76 years). In terms of sex, 5 males and 2 females are reported on herein. Similar to previous reports, the most likely cause of hospitalization was massive hematochezia, rather than melena[3]. Pathological analyses showed the main vascular factors of appendiceal bleeding to be angiodysplasia and Dieulafoy’s lesion. Dieulafoy’s lesion is caused by an abnormal artery that fails to diminish to the minute size of the mucosal capillary microvasculature[11]. The most common location of Dieulafoy’s lesion is the stomach. Others have reported Dieulafoy’s lesion in the esophagus, duodenum, small intestine, colon, and rectum[12-15]; however, an appendiceal Dieulafoy’s lesion is extremely rare. Among the included publications, there were only 2 cases of appendiceal bleeding due to Dieulafoy’s lesion published in English language[5,7], with ours being the third case.
Acute lower gastrointestinal bleeding is commonly encountered in clinical practice, with colon being responsible for the majority of cases[1]. Appendiceal bleeding, on the other hand, is an extremely rare cause, and as such may be missed or misdiagnosed.Although lower gastrointestinal bleeding is generally less severe than upper gastrointestinal bleeding - with spontaneous cessation of the bleeding occurring in most cases, appendiceal bleeding attributed to vascular diseases, such as angiodysplasia and Dieulafoy’s lesion, may result in massive lower gastrointestinal bleeding and sometimes can be lifethreatening[1,4]. As a clinician, having an awareness of appendiceal bleeding is significant. A literature search of relevant articles on the PubMed/MEDLINE database, from January 1977 to November 2021,was conducted, using the key words of “appendix bleeding” or “appendix hemorrhage”. Six articles regarding appendiceal bleeding due to vascular diseases were identified (Table 1)[5-10].
A reliable and effective choice of treatment for appendiceal bleeding is appendectomy[2]. Other attempts, including vessel embolization and endoscopic therapy (therapeutic barium enema and endoclips), have been reported as successful for controlling bleeding[9,16,17]; however, the risk of acute appendicitis and rebleeding after vessel embolization and endoscopic therapy are unmanageable, and the patient may still require an appendectomy[9,17]. Studies for the feasibility of vessel embolization and endoscopic therapy continue to be warranted.
CONCLUSlON
We present a treatment experience of appendiceal bleeding caused by Dieulafoy’s lesion. Although appendiceal bleeding is a rare cause of acute lower gastrointestinal bleeding, clinicians should consider it during differential diagnosis.
469 Risk factors of intravesical recurrence after upper-tract urothelial carcinoma surgery
FOOTNOTES
Zhou SY designed and drafted the manuscript; Guo MD performed the colonoscopy; Ye XH revised the manuscript for important intellectual content; and all authors approved the final version of the manuscript.
Bleeding of the appendix.
the Natural Science Foundation of Zhejiang Province, No. LQ19H030003; and Key Project of Jinhua Science and Technology Bureau, No. 2018A32022.
Consent was obtained from the patient for publication of this report and any accompanying images.
The personal and family history-taking revealed no information relevant to the current case.
An emergency colonoscopy was performed, and extended up to the terminal ileum. During the procedure, blood clots in the cecum were first washed out and we were then able to observe a large quantity of fresh blood oozing out of the appendiceal orifice (Figure 1A). In addition, contrast-enhanced abdominal computed tomography (CT) scan showed a high-density area in the appendix without any signs of acute appendicitis, tumor, or diverticulum (Figure 1B).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
針對(duì)實(shí)驗(yàn)設(shè)計(jì)方案中所采用的單點(diǎn)并聯(lián)接地設(shè)計(jì)方案,與單點(diǎn)串聯(lián)聯(lián)接地方案對(duì)比,對(duì)于輸入信號(hào)噪聲的抑制對(duì)比結(jié)果如圖8、圖9所示。
China
當(dāng)然,產(chǎn)假制度也有其消極影響。一方面,對(duì)于企業(yè)來說,員工休產(chǎn)假會(huì)打亂企業(yè)平常的節(jié)奏,企業(yè)還要承擔(dān)部分因員工產(chǎn)假而導(dǎo)致的工作調(diào)動(dòng)、繳納社保、工資等費(fèi)用。另一方面,對(duì)于女職工自身而言,她們會(huì)因?yàn)樾莓a(chǎn)假而長(zhǎng)期脫離工作崗位,可能存在著影響個(gè)人晉升與職業(yè)長(zhǎng)期發(fā)展的擔(dān)憂。公司和員工在產(chǎn)假這個(gè)問題上進(jìn)行博弈,由于雇主擁有權(quán)力和信息方面的絕對(duì)優(yōu)勢(shì),可以通過釋放一些模棱兩可的信息和隱晦的威脅,從而對(duì)員工產(chǎn)生壓力并且在實(shí)際操作中變相降低她們的收入等。
Sheng-Yue Zhou 0000-0001-5808-2545; Mao-Dong Guo 0000-0003-4016-0773; Xiao-Hua Ye 0000-0002-8358-4093.
Wang JJ
從初中數(shù)學(xué)教材的角度出發(fā)來看,學(xué)生首先學(xué)習(xí)的函數(shù)圖像是一次函數(shù)圖像,老師在實(shí)際教學(xué)中往往根據(jù)一個(gè)具體函數(shù)表達(dá)式,首先通過一些計(jì)算,然后完成列表、描點(diǎn)、連線這三部曲,就此得到一次函數(shù)的圖像,再往后就是學(xué)習(xí)反比例函數(shù)圖像以及二次函數(shù)圖像,其教學(xué)歷程“自然”的讓人找不出任何瑕疵,很少有人會(huì)在這塊內(nèi)容的教學(xué)上提出異議.就這樣,函數(shù)圖像在不經(jīng)意之間來到了我們身邊,我們對(duì)此習(xí)以為常.
A
Wang JJ
猜你喜歡
環(huán)境(2023年5期)2023-06-30 01:20:01
小星星·閱讀100分(低年級(jí))(2022年6期)2022-08-22 02:33:40
供水技術(shù)(2021年3期)2021-08-13 09:08:34
建材發(fā)展導(dǎo)向(2019年10期)2019-08-24 06:25:02
當(dāng)代水產(chǎn)(2019年1期)2019-05-16 02:42:04
當(dāng)代水產(chǎn)(2019年3期)2019-05-14 05:42:48
電子制作(2018年14期)2018-08-21 01:38:16
水利規(guī)劃與設(shè)計(jì)(2018年1期)2018-01-31 01:53:53
水利規(guī)劃與設(shè)計(jì)(2016年7期)2016-02-28 15:06:27
世界文學(xué)評(píng)論(2014年2期)2014-04-12 06:23:43
 World Journal of Clinical Cases2022年18期
World Journal of Clinical Cases2022年18期
- World Journal of Clinical Cases的其它文章
- Stem cells as an option for the treatment of COVID-19
- Development of clustered regularly interspaced short palindromic repeats/CRISPR-associated technology for potential clinical applications
- Prostate sclerosing adenopathy: A clinicopathological and immunohistochemical study of twelve patients
- Effectiveness and postoperative rehabilitation of one-stage combined anterior-posterior surgery for severe thoracolumbar fractures with spinal cord injury
- Construction and validation of a novel prediction system for detection of overall survival in lung cancer patients
- Identification of potential key molecules and signaling pathways for psoriasis based on weighted gene coexpression network analysis