Ophthalmic manifestations of Cryptococcus gattii species complex: a case series and review of the literature
2022-01-20 07:00:32GraceMcCabeJackMcHughToddGoodwinDouglasJohnsonAnthonyFokThomasCampbell
關(guān)鍵詞:財(cái)務(wù)管理教師
INTRODUCTION
Thecomplex species are spore-forming,soil-dwelling fungi.() was historically considered a variety of().Increased recognition of unique epidemiological,morphological, and clinical features led to its designation as an independent species in 2002. Genotyping identified at least four molecular types or genotypes of(variety gattii; VG), VGI, VGII, VGIII, and VGIV, with each of these genotypes containing subtypes. Based on phylogenetic analysis of genetic loci and genotyping studies Hagendemonstrated significant genetic diversity and proposedbe divided into two species andinto five species. Subsequent published genotypes have revealed greater genetic diversity than is encompassed by the seven species. In an effort to recognise genetic diversity without creating confusion Kwon-Chungproposed the use of“species complex” as a practical solution, rather than creating more species. In this manuscript when “” is used it refers to the “species complex”.
Thoughhas long been established as a cause of endemic infection in the sub-tropics and in Australia, an outbreak in Vancouver Island in 1999 led to spread ofinto the Pacific Northwest region of the United States,with further reports described elsewhere in the United States and in Europe in more recent years. It appears genotype distribution and frequency are dependent on geographic regions. In Australia VGI is the most common genotype of isolates whereas isolates from the outbreak in Canada and the Pacific Northwest region of the United States were the molecular type VGII.
Infections caused byhave classically been associated with immunosuppressed individuals, most frequently HIV/AIDs patients. In contrast,infections have predominantly been documented in healthy and immunocompetent patients. The majority of patients present with central nervous system (CNS) infection, with concurrent or isolated pulmonary infection also common.
A notable observation ofCNS infection is the high rate of visual sequelae, particularly when compared to infections caused byWe present cases from multiple centres that illustrate the diverse ophthalmic manifestations of. We will also review the literature to evaluate ophthalmic manifestations ofinfection,prognosticators of visual outcome, and treatment modalities.To our knowledge this is the first study that has specifically examined ophthalmic manifestations ofinfection.
SUBJECTS AND METHODS
In summary, though many papers examiningmeningitis note ophthalmic signs and symptoms, there is limited data regarding long-term sequelae, and only one study that specifically examined risk factors for visual loss. Reported rates of visual loss varied from 11%-53%, in contrast to studies examining, where visual loss has been reported in 1%-9% of cases.
Four cases ofwere independently identified, including cases from Victoria and Queensland, Australia, and the midwest region of the United States. The ocular and systemic characteristics, treatment, and visual outcomes are reported.A MEDLINE literature search (1990 through 2020) was performed to identify cases ofmeningoencephalitis where ophthalmic manifestations were reported. All reported cases were reviewed and tabulated, together with our series of patients, in this report.
對(duì)本科護(hù)生進(jìn)行循證護(hù)理理念培養(yǎng)必不可少,將其與真實(shí)病人PBL教學(xué)相結(jié)合,并應(yīng)用于護(hù)生見習(xí)環(huán)節(jié),有助于提高護(hù)生批判性思維能力,提高護(hù)生見習(xí)參與度,且與傳統(tǒng)見習(xí)模式相比,其在提高護(hù)生自學(xué)能力、發(fā)現(xiàn)問題和解決問題的能力及團(tuán)隊(duì)合作能力方面認(rèn)可度較高。
RESULTS
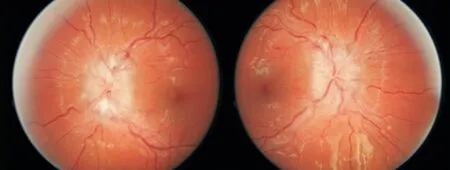
A 20-year-old healthy female presented to a tertiary hospital with a 2-month history of frontal headache, night sweats, and blurred vision. Neurological examination was notable for significant nuchal rigidity, visual acuity (VA) was 6/9 right eye and 6/9 left eye, with normal colour vision and no relative afferent pupillary defect (RAPD). Ophthalmoscopy showed bilateral optic nerve swelling (Figure 1). She had not travelled rurally.
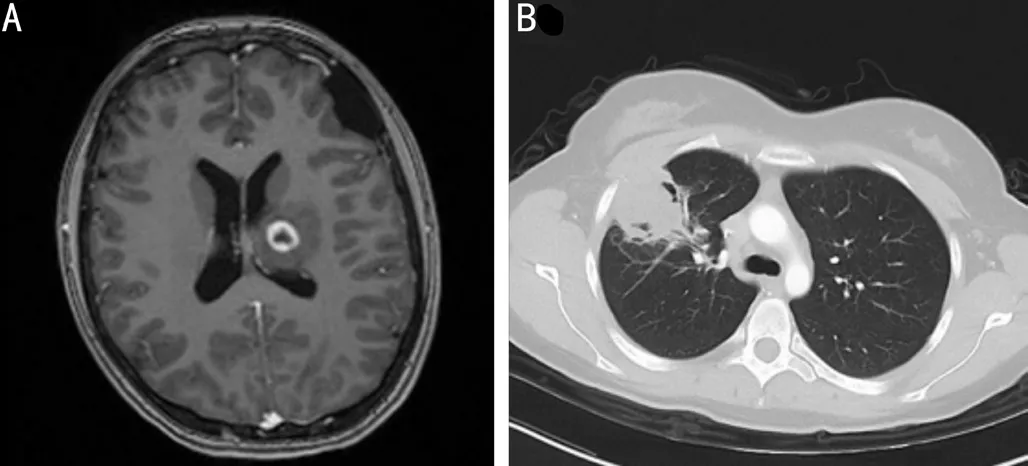
Magnetic resonance imaging (MRI) brain showed T1 ringenhancing lesion (Figure 2A) and computed topography (CT)chest showed cavitating lesions in both lungs (Figure 2B).Lumbar puncture (LP) revealed a normal opening pressure(OP), with analysis of cerebrospinal fluid (CSF) demonstrating lymphocytic pleocytosis and Cryptococcal antigen (Crag) titre>1:2560. CSF culture grewwhich was subtyped toVGI using matrix-assisted laser desorption/ionization coupled to time-of-flight spectrometry (MALDI-TOF).Liposomal amphotericin B and flucytosine were initiated. HⅠV testing was negative.
網(wǎng)絡(luò)形式是企業(yè)引進(jìn)新型財(cái)務(wù)管理模式的中心,且網(wǎng)絡(luò)支付是創(chuàng)新需要考慮的首要因素。網(wǎng)絡(luò)環(huán)境也并非如想象般安全,潛在的很多不安定因素將會(huì)給企業(yè)創(chuàng)新帶來大量的問題。例如,不完善的網(wǎng)絡(luò)管理制度,將會(huì)給黑客等不法分子提供可乘之機(jī),對(duì)網(wǎng)絡(luò)安全造成極其惡劣的影響。此外,企業(yè)網(wǎng)絡(luò)方面的優(yōu)秀人才和過硬的軟件管理技術(shù)的匱乏也將可能提高網(wǎng)絡(luò)環(huán)境的危險(xiǎn)程度。更為嚴(yán)重的是,在中國(guó)沒有制定相應(yīng)的網(wǎng)絡(luò)法律條文,在法制時(shí)代下,沒有法律的約束,企業(yè)財(cái)務(wù)管理所面臨的危險(xiǎn)將大大提高。所以,企業(yè)需要?jiǎng)?chuàng)新網(wǎng)絡(luò)財(cái)務(wù)管理制度,著重提高網(wǎng)絡(luò)技術(shù),雇傭相應(yīng)的網(wǎng)絡(luò)技術(shù)人才。國(guó)家也需要盡快建立專門的網(wǎng)絡(luò)法律法規(guī)約束不法分子,加強(qiáng)對(duì)網(wǎng)絡(luò)的保護(hù)。
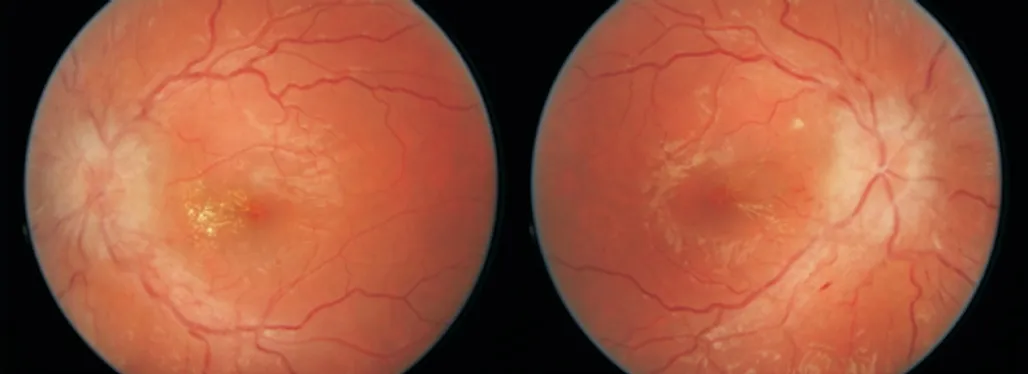
One week post-initiation of therapy headache continued.Repeat LP revealed an OP of 32 cm HO CSF. Ophthalmic assessment demonstrated dyschromatopsia, right RAPD and worsening of optic disc swelling consistent with grade 5 papilloedemaRepeat MRI brain showed hydrocephalus. She had daily LP until day 20 of admission, when a ventriculoperitoneal (VP) shunt was inserted, resulting in immediate symptomatic improvement. She completed a 6-week induction course of liposomal amphotericin B and flucytosine infusions,followed by a 12mo course of fluconazole to complete consolidation and maintenance therapy. At follow-up 4-months post-discharge her visual acuity was 6/5 in both eyes, with grade 3 papilloedema, and lipid deposits present at the left parafoveal area (Figure 3)
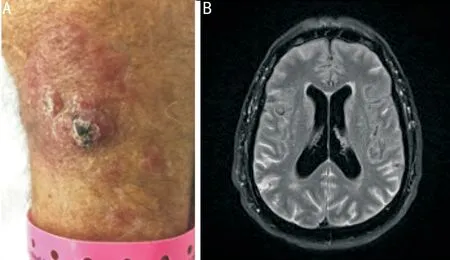
A 61-year-old male presented to an Emergency Department in the mid-west region of the United States, with a 6-month history of headache, vomiting, and 5 kg weight loss. He was immunosuppressed with tacrolimus 2 mg BID, prednisone 10 mg OD, mycophenolate mofetil 250 mg BID following renal transplantation two years prior. The source of infection was not clear. Donor derived transmission ofhas previously been described, however this patient had travelled toendemic regions in the north-western United States. Examination was notable for skin lesions on left forearm (Figure 4A). LP was obtained;OP was 50 cm HO CSF. CSF fungal smear demonstrated. Amphotericin B and flucytosine were initiated and his immunosuppressive regimen was tapered.
The 4 cases presented here, allied with a review of the existing literature, illustrate a number of important principles related to infection with. The first of these is the broad geographical distribution. While previously thought to be a disease of the tropics and sub-tropics,is now recognized as an endemic fungus in the United States, most prevalent in the North-western regions of the country. Host factors also appear to differ significantly when compared to, with infection withobserved more frequently in immunocompetent hosts.
A 41-year old previously well male presented to an Emergency Department in Queensland with a 4-week history of worsening headaches and fever. LP was performed and revealed normal OP with CSF Crag titre of >1:1280 with subsequent culture positive for. CT brain was unremarkable and CT chest demonstrated a pulmonary cryptococcoma in the left lower lobe.
The patient had no visual symptoms but was referred to the ophthalmologist for routine review, with initial VA of 6/4.5 in both eyes. Dilated slit lamp examination was notable for a retinal lesion temporal to the fovea of the left eye, with intra-retinal oedema. Infrared imaging and optical coherence tomography (OCT) and demonstrated a cryptococcoma (Figure 5A, 5B). The optic nerves were normal.
He was treated with amphotericin B and flucytosine infusions.Daily funduscopic examinations showed the retinal lesion reducing in size. After 3wk of inpatient care, he was discharged home after 3wk on oral fluconazole.
The patient returned to the emergency department 5d post discharge with worsening headaches. Repeat MRI demonstrated multiple cerebral cryptococcomas. He was recommenced on amphotericin B and flucytosine infusions and oral fluconazole. The retinal cryptococcoma continued to reduce in size, however the patient developed optic nerve head swelling that continued to worsen on subsequent reviews despite several LPs demonstrating OPs of no higher than 25 cm HO of CSF. He was re-commenced on amphotericin B and flucytosine infusions for 6wk.
The second of these is thatis associated with significant visual sequelae, in particular when associated with intracranial hypertension. While papilloedema is strongly associated with vision loss, it is not present in all cases,and prompt recognition and management of intracranial hypertension with decompressive therapies is critical. Unlike in idiopathic intracranial hypertension, acetazolamide and mannitol are associated with adverse side effects and poor outcomes.Third, these cases highlight the protean ophthalmic and systemic manifestations possible ininfection. Our cases demonstrate thatinfections can cause myriad ophthalmic pathologies including vision loss, papilloedema,and retinal cryptococcomas. While the phenomena of endophthalmitis and retinal cryptococcomas secondary tohave been documented only rarely in the literature, their possibility warrants dilated funduscopic examination. We recommend that all patients diagnosed withmeningitis be referred to an ophthalmologist/neuro-ophthalmologist at presentation and receive long-term follow up during their treatment course to assess for ophthalmic sequelae. Whilst the literature is relatively sparse in this area, there is a suggestion thatis associated with worse visual outcomes than. Whether this is related to differential rates of fungal blockage of CSF, an as yet unidentified mechanism,or a spurious finding, requires further elucidation. Further studies that directly compare the mean ICP and ophthalmic manifestations ofandwould contribute significantly to the literature in this area.
由于杏A注水站停運(yùn)后將減少注水量約1.21×104m3/d,為保障區(qū)域內(nèi)生產(chǎn)用水需求,需要具備連通性的其他深度注水站提高注水量約1.21×104m3/d。相鄰深度注水站生產(chǎn)運(yùn)行情況見表4,由表中數(shù)據(jù)可知,杏B注水站、杏C注水站、杏D注水站注入能力可滿足杏A注水站停運(yùn)后的注水量需求。
An independent 58-year-old female from rural Victoria, Australia presented to the local Emergency Department with a cough and lethargy. She had hypertension,obstructive sleep apnoea and migraine.Treatment for community acquired pneumonia was initiated,however 6wk later she returned to the Emergency Department with headaches and confusion associated with photophobia,phonophobia and visual disturbance. Bronchoalveolar lavage with cultures confirmedinfection. MRI brain demonstrated a well circumscribed lesion of the right temporal lobe (Figure 6A). Flucytosine and amphotericin B were prescribed for a 6wk course, followed by consolidation with oral fluconazole. Weekly LPs were performed for chronic headache, with recorded OPs of 26-36 cm HO CSF.Four months following diagnosis she was transferred to our tertiary centre with ongoing postural headaches associated with photophobia, blurred vision, scintillations and new papilloedema. On ophthalmic examination, VA was 6/12 right eye and 6/7.5 left eye. Fundal examination demonstrated grade 2 papilloedema of both eyes (Figure 7). Repeat imaging showed multiple enlarging ring enhancing cryptococcomas with substantial progression of vasogenic oedema in the right supratentorial brain parenchyma (Figure 6B). VP shunt was inserted with improvement in symptoms.
兩組患者在治療前的舒張壓、……
登錄APP查看全文
猜你喜歡
快樂語(yǔ)文(2021年27期)2021-11-24 01:29:04
黃河之聲(2021年5期)2021-05-15 02:31:24
河南水利年鑒(2020年0期)2020-06-09 05:43:36
甘肅教育(2020年22期)2020-04-13 08:11:16
福建基礎(chǔ)教育研究(2019年3期)2019-05-28 23:14:43
小學(xué)生優(yōu)秀作文(高年級(jí))(2018年9期)2018-09-14 02:42:12
消費(fèi)導(dǎo)刊(2018年8期)2018-05-25 13:20:09
行政事業(yè)資產(chǎn)與財(cái)務(wù)(2016年10期)2016-09-26 12:05:29
行政事業(yè)資產(chǎn)與財(cái)務(wù)(2015年23期)2015-10-26 03:13:26
現(xiàn)代農(nóng)業(yè)(2015年5期)2015-02-28 18:40:58
 International Journal of Ophthalmology
2022年1期
International Journal of Ophthalmology
2022年1期
- International Journal of Ophthalmology的其它文章
- lnstructions for Authors
- Comment on: Trends in research related to high myopia from 2010 to 2019: a bibliometric and knowledge mapping analysis
- Progress of clinical therapies for dry age-related macular degeneration
- Observation seasonal variation of intraocular pressure in young healthy volunteers
- Effectiveness of oral probiotics supplementation in the treatment of adult small chalazion
- Characterization and validation of a chronic retinal neovascularization rabbit model by evaluating the efficacy of anti-angiogenic and anti-inflammatory drugs