lmpact of systemic steroids combined with immunosuppressive treatment on glaucomatous features in patients with systemic lupus erythematosus
2022-01-20 07:03:52MartaWicekDanutaBobrowskaSnarskaMarekBrzoskoWojciechLubiskiMonikaModrzejewska
INTRODUCTION
Systemic lupus erythematosus (SLE) is a chronic inflammatory disease caused by autoantibodies and complement fixing immune complexes, associated with an abnormally activated immune system. This disease can affect various organs, among which the eyeball can be involved in about 34.6%, as a result of both lupus-induced and iatrogenic events. Ⅰt is known that SLE may affect almost any structure of the eye and the commonly known ocular manifestations include keratoconjunctivitis sicca, scleritis, retinal vascular disease and neuro-ophthalmic diseases. The common use of glucocorticosteroids (GC), taking advantage of their antiinflammatory and immunosuppressive effects to treat SLE,shows potential ocular side effects in the form of posterior subcapsular cataract (6.4%-38.7%), increased risk of local infection, ocular hypertension as well as steroid-inducediatrogenic glaucoma (SIG) or neovascular glaucoma in the course of severe SLE retinopathy (3%). Ophthalmological adverse effects can be very disabling, leading to visual field loss and even blindness.

For over 30 years, there has been observed a relation between GC and ocular hypertension as well as secondary or primary open angle glaucoma (POAG) but the influence of a longterm use of steroids combined with immunosuppressive agents on glaucoma in SLE remains unclear. Therefore, we decided to investigate this subject more thoroughly. This paper addresses the role immunosuppressive therapy may play in altering intraocular pressure (IOP) in SLE patients.Moreover, the relationship between the administered therapy in early glaucomatous signs established in optical coherence tomography (OCT) of the optic disk, as well as the macular region, scanning laser polarimetry (GDx) and perimetry.The aim of the study was to determine the association between already applied SLE treatment schemes with early glaucomatous lesions or IOP values in the studied group.
養生時間超過7d之后,混凝土路面就可以進行刻槽,刻槽作業應嚴格控制好時間,一般應在混凝土強度達到85%時進行。為了避免刻槽時出現線條不直問題,應該經常調整刻槽機所用的鋸片。
SUBJECTS AND METHODS
The mean time of GC therapy in GC group was 7.89±0.52y.Detailed analysis of basic ophthalmological examinations according to GC treatment were presented in Table 1. No statistical differences in BCVA, ⅠOP or OPA between GC and GC-free groups were detected. Since increased IOP values are the best known factor in both glaucoma and SIG the detailed analysis of IOP according to the treatment regimen in SLE patients was performed. Consequently, IOP values over 21 mm Hg were observed in 3 eyes (3.19%; 2 patients) in GC group and 5 eyes (16.67%; 3 patients) in GC-free group. Only one of the individuals from GC group had received topical IOP decreasing therapy (timolol twice a day) due to increased IOP values diagnosed during SLE therapy and the rest were newly discovered. In GC-free group none of the examined patients received any IOP decreasing therapy. Interestingly, the mean IOP value in GC group treated with immunosuppressive agents was 15.8±2.56 mm Hg and was significantly lower than in individuals with exclusive GC administration(17.63±4.38 mm Hg,=0.043). Moreover, no significant differences in mean IOP values between GC-free group and individuals treated with combined GC and immunosuppressive therapy were observed (=0.563).
通常情況下,課堂提問的主體是教師,由學生回答教師提出的問題,這樣的教學模式會使很多學生感覺自己在被動獲取數學知識。在互動教學背景下,高中數學教師可以采用互相提問的方式為學生講解數學課程。首先,教師可以根據教學內容向學生提出問題,用于啟發學生的數學思維;其次,教師可以鼓勵學生將自己在學習過程中產生的疑問提出來,與教師共同探究問題的答案。
The patients were divided into groups based on GC administered systemically: 47 patients (94 eyes) who received systemic oral and/or intravenous GC therapy (GC group) and 15 individuals(30 eyes) not treated with systemic GC (GC-free group). The GC doses of prednisolone and methylprednisolone amounted to 16.55±5.97 mg/d. The mean GC treatment time was 7.89±0.52y. According to the fact that GC-induced changes might appear asymmetrically the decision of inclusion of both eyes of each individual in the analysis was made. The mean age was 40.62±13.02y without significant differences in both groups. The women receiving GC suffered from the disease significantly longer and SLE was diagnosed at a younger age than in the GC-free group (<0.05). The number of administered immunosuppressive and immunomodulating agents (methotrexate, azathioprine, cyclophosphamide,mycophenolate mofetil, cyclosporine A) was significantly higher in the group receiving GC (<0.05). This group also received biologic treatment (belimumab) significantly more often than the GC-free group. The demographic characteristics of the studied group were presented in Table 1. The exclusion criteria for the analysis were: glaucoma diagnosed prior to SLE(=3), diabetes, high degenerative myopia, chronic ophthalmic diseases unrelated to increased IOP, previous eyeball surgeries excluding uncomplicated phacoemulsification or history of eye injuries. The presence of eye fundus changes (=2,postinflammatory scars) and changes in perimetry unrelated to increased IOP were also exclusion criteria for the analysis(=2, suspicion of an intracranial pathologies).
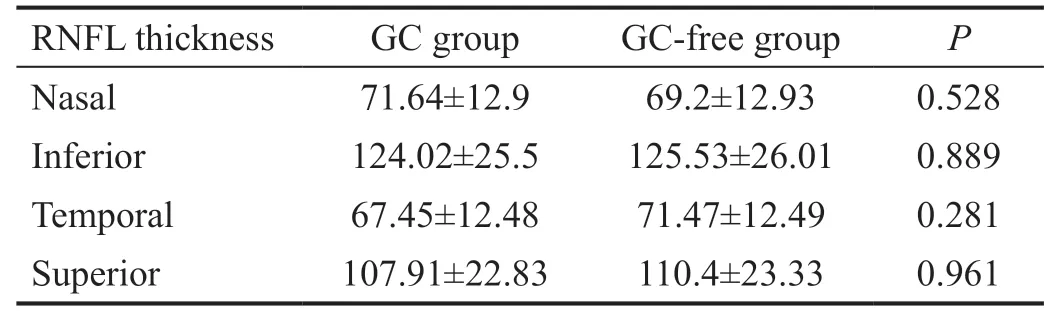
The following ophthalmic examinations were performed: best corrected visual acuity (BCVA) and IOP with ocular pulsatile amplitude (OPA) measurements with the use of Snellen’s chart and dynamic contour tonometry(PASCAL, SMT Swiss Microtechnology AG), respectively.Spectral domain optical coherence tomography (SD-OCT,Cirrus HD 5000 Carl Zeiss, Germany) of the optic disc was conducted after dilation of the pupils. The optic nerve head(ONH) and RNFL OU analysis with Optic Disk Cube 200×200 formula was performed. The evaluated parameters included:the thickness of the retinal nerve fiber layer (RNFL), the symmetry of RNFL between eyes, the volume of the central cup and the ratio of the central cup diameter to the surface of the optic nerve (C/D ratio). Additionally, measurements of the RNFL thickness in nasal, temporal, inferior, and superior parts of the optic disc were evaluated. The Ganglion Cell Analysis Protocol was used in the OCT test of the macular region what assessed automatically the average and minimal total thickness of the ganglion cell layer and the inner plexiform layer(GCL+IPL). GDx was also used (GDx VCC: 5.5.1, Carl Zeiss,Germany), to measure the thickness of the nerve fibers around the optic nerve disc and the retinal nerve fiber index (NFⅠ) was assessed. The analysis was based on the Nerve Fiber Analysis formula. Static and kinetic perimetry were performed in all patients in order to rule out deficiencies or narrowing of the peripheral visual field. Considering the fact, that functional changes in perimetry seem to appear later than morphological lesions in OCT or GDx, perimetry parameters have not been analyzed and served exclusively to exclude lesions unrelated to increased IOP. Due to the possible asymmetry in occurrence of changes in the posterior pole, a decision was made to include into the study ophthalmic examinations of both eyes for each patient. OCT images with signal strength less than 6 were considered as poor quality and were not used for further evaluation. Glaucoma in first degree relatives occurred in 8 patients from the GC group and in 1 patient from the GCfree group. Due to the lack of a representative quantity, the relationship for this parameter has not been analyzed.
A chronic use of topical GC in the form of eye drops leads to IOP elevation within a few weeks whereas after intravitreal steroid injection, incorrect IOP values can be noted right after completion of this procedure. In the literature, the IOP increase in 11%-32% of eyes lasting 2mo after intravitreal dexamethasone injection was described. However, some authors describe lower rate in a low risk group of patients.In the case of systemic administration of the drug it is assumed that this effect will be achieved after a few years of therapy. The literature describes the tendency of IOP increase which correlates with an increase of the dose and treatment duration. However, correlation of higher mean IOP values with dose or treatment duration was not observed in the GC group. By contrast, in the examined GC group a lower incidence of ocular hypertension was observed than in GC-free group and as described in the literature in the general population. These observations have been supported with imaging results (Tables 2-4). Another factor, described as significant for IOP rise in GC therapy, is the particle structure. GC with lipophilic structure,, acetates, are characterized by a greater influence on the development of SIG as compared to hydrophilic phosphates, due to a higher corneal permeability. Other risk factors for SIG include both ocular hypertension and POAG in patients receiving GC as well as POAG in first degree relatives of these individuals.Two peaks of SIG incidence have been reported: in children and elderly populations. In children, the response to GC was found to be more expressed. This results in IOP increase by over 21 mm Hg in 71.2% of patients who receive eye drops with dexamethasone 4 times a day and 59.2% if used twice a day. Moreover, high myopia predisposes the patient to a higher incidence of POAG as well as to secondary glaucoma.Systemic diseases, such as type 1 diabetes, rheumatoid arthritis or connective tissue diseases especially in the male sex may also increase the risk of SIG. It has been suggested that POAG is more common in patients exposed to 7.5 mg daily doses of prednisone-equivalent for over 1y. In the studied group of patients, the drug doses were higher but that correlation was not observed.
One of the hypotheses explaining the decreased incidence of ocular hypertension or lack of SIG in the GC group, is the expression pattern of GRs as a subject of major regulatory variation. The negative effect of GC on GRs expression may represent a short-loop feedback mechanism which protects tissues from excessive GC levels. The other factor is hypersensitivity within the TM and the lack of ability to self-regulate the levels of GRs. The other hypothesis is an increased expression of thegene in the TM, which is responsible for myocilin synthesis.is a subunit of β3 integrin which induces the activation of calcineurin and the nuclear factor of activated T-cells (NFAT). This gene is present in 4% of patients with POAG and determinates a late onset of the disease. The basis of glaucoma related tois impaired secretion of myocilin from the cell, its accumulation and endoplasmatic reticulum stress. This process leads to an altered TM cell function. The influence of TM cells stretching and IOP elevation on induction of theexpression is also suspected. Anstudy showed a 30-fold increase ofexpression after one day of treatment with topical dexamethasone, which lasted for up to 12d from the cessation of eye drops. Faralliproved that cyclosporine A, as a suppressor of calcineurin phosphatase activity, significantly decreases the rise of IOP after dexamethasone implementation.Addition of 10 μmol/L of cyclosporine A reduced cell response by 71%, compared to dexamethasone. The same observation concerned the selective calcineurin inhibitor (INCA-6) which prevents calcineurin from binding to NFAT. Hence, calcineurin and thepathway are suspected as responsible forupregulation and a dexamethasone-induced IOP increase. This thesis is supported by the fact that GC combined with GRs cause the release of heat shock proteins. This activates calcineurin in a calcium independent mechanism.According to our knowledge, this is the first study to reveal IOP differences due to immunosuppressive therapy in SLE patients. However, further investigation of this field may be crucial for the treatment and prevention of SIG. Moreover, the exact mechanism of “glaucoma gene” currently remains unknown.Difficulty of finding a larger group of patients not treated with GC was a limitation of our study, which resulted from the fact that a GC therapy at the first flare of SLE treatment according to the EULAR recommendations. Nevertheless,the differences in IOP values in subjects treated with GC combined with immunomodulating agents in comparison with GC only occurred to reach satisfactory significance level.
RESULTS
The study was approved by the Local Ethics Committees and was performed in accordance with the Declaration of Helsinki. The written informed consent was provided by all individuals.
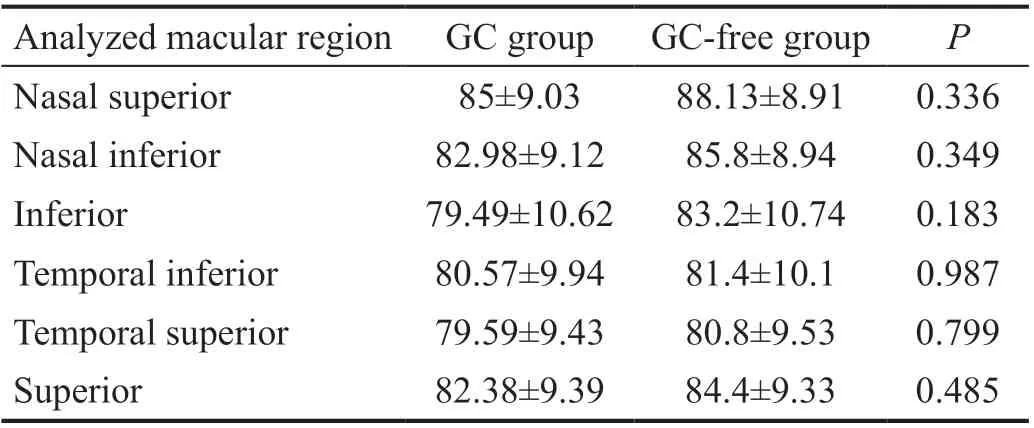
The mean GCL+IPL thickness in the GC group reached 84.07±8.41 μm while in the GC-free group 81.77±8.49 μm(=0.425). The minimum thickness of the GCL+IPL complex noted in the first group was 80.53±12.59 μm and 75.04±12.54 μm in the second group (=0.146). The complex thickness of ganglion cells in the following sectors in each eye separately were also assessed: superior, inferior, temporal superior,temporal inferior, nasal superior, and nasal inferior. No significant differences in particular sectors were found in the studied groups (Table 2).
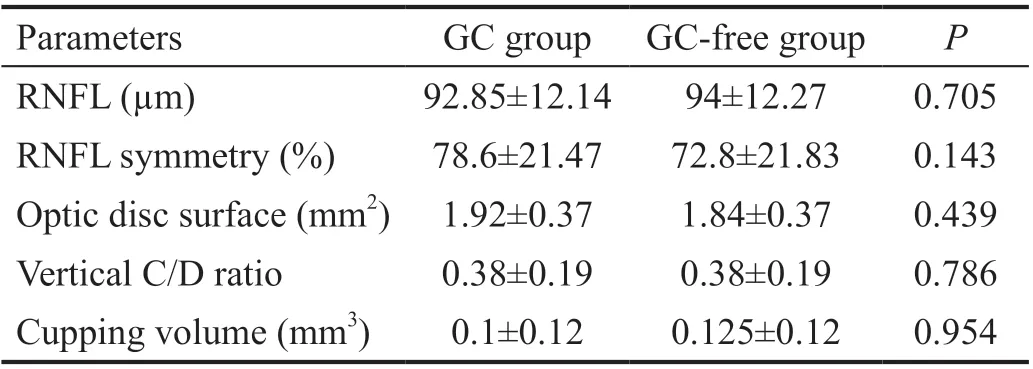
In the optic disc OCT, the thickness of the RNFL in patients treated with GC was 92.85±12.14 μm. In GC-free SLE patients this value was equal to 94±12.27 μm (=0.705). Analysis of this and other parameters of the optic disc in SLE patients depending on the administration of GC were presented in Table 3.
No statistical significance was found while comparing the optic nerve parameters in the OCT examination depending on GC administration in SLE individuals (Table 4). Similarly, no statistically significant differences for the NFI parameter in GDx were shown between groups (GC group: 15.95±7.66 μm;GC-free group: 18.31±7.74 μm,=0.517).
Similarly, no significant differences in OCT or NFI values in the subjects with combined GC and immunosuppressive therapy in comparison with GC exclusive or GC-free groups were observed.
DISCUSSION
The data in literature show that the response of the eye to steroid therapy is genetically determined with 18%-36%of the population belonging to the group of GC-sensitiveindividuals. This means that in predisposed individuals,administration of topical GC in the form of eye drops with dexamethasone for 4-6wk, leads to an increase in IOP by over 15 mm Hg in 5% of individuals while in 30% of persons an increase by 6-15 mm Hg can be expected. Two thirds of the population belong to the group of the so called “insensitive to GC”, what means that after a local steroid therapy an increase in IOP does not exceed 5 mm Hg, according to Armaly’s classification. SLE patients as individuals successfully treated with GC are usually in the group of GC sensitive population.The influence of GC on IOP is strictly related to the dose,treatment duration and the route of administration. SIG has been reported in all GC administration routes, including intravenous, oral, topical as skin ointment or eye drops,intravitreal and inhalatory. Moreover, steroid-induced increase of IOP is usually transient, reversing after cessation of GC but only if used for less than a year. Elevated IOP may be permanent if GC are continued for over 17mo, which results inaltered GC metabolism and an increased aqueous humor outflow resistance in the trabecular meshwork (TM)with the following changes: thickening of trabecular beams,decrease of intratrabecular spaces, increased deposition of extracellular material in the juxtacanalicular tissue(juxtacanalicular region). Moreover, receptor complex,nuclear transcription factors, a change in the PGF2a and PGE2 metabolism, as well as the/gene are the risk factors for both POAG and SIG in SLE patients. Although a steroid induced increase of IOP may be reversible, the subsequent optic nerve damage is permanent.
酒店管理專業的人才培養方案與課程體系,更傾向于實踐,專業培養目標是學生的動手能力、操作能力、運營能力和研發能力。要培養學生較強的實踐操作能力,就要有大量的實踐教學,這就使酒店管理專業的實訓基地建設的重要性日益凸顯。因此,實訓基地的建設在專業建設中已經成為非常重要的一部分,從建設實訓基地初始進行整體情況梳理,使其對應學生培養目標,對接課程體系,最終協同行業企業崗位技能訓練,每一個流程都將對酒店管理專業教學產生重大的影響。為更好建設實訓基地本文將對國內外實訓基地進行比較研究,以期為實訓基地建設提供更好借鑒。
SHY-2改造后鉀鈣基鉆井液配方1#4%BTJ+0.2%TSN+0.3%QYHN+7%LHJ+0.8%MAN101+0.8%MAN104+0.5%FN-2+2%SHY-2+0.2%XY-27+0.5%DYGRHJ+0.5%SMF+3.5%KR-n+0.2%YHG+2%QCX-1+1%WC-1+BA;
The statistical analysis for parameter variables was performed with the use of the Student’stest and for the non-parameter variables with the Mann-Whitneytest.The calculations were made using the Statistica 13.3 (Statsoft,Tulsa, OK, USA) software. The values of<0.05 were deemed statistically significant.
Despite a long time of GC treatment and high doses of GC in the examined group neither an increase of IOP nor features of neuropathy in SD-OCT or GDx were observed. The abovementioned observations motivated the authors to look for an explanation for the absence of SIG in the studied SLE patients.According to some authors, glaucoma in SLE may be accompanied either by severe SLE complications, which involve neovascular processes in severe lupus-retinopathy or it may be associated with long-term use of GC. Due to the presence of the glucocorticoid receptor (GRs) in the TM and persistent elevation of cortisol level, SIG is especially associated with biochemical changes in the morphology of the TM cells. Characteristic features include an increased deposition of extracellular material in the trabecular beams and in the juxtacanalicular tissue(cribriform region) with a decrease of intratrabecular spaces,thickening of trabecular beams and an activation of the TM cells. Increased deposition of extracellular matrix composed of glycosaminoglycans, fibronectin and elastin is a result of its increased synthesis and reduced degradation. The function of the TM is inhibited with a decreased proliferation, migration and phagocytosis what results in accumulation of debris in both, intratrabecular spaces and the uvea.
This study was designed as a clinical, original casecontrol study of an observation type. The study involved randomly selected 62 women (124 eyes) with SLE diagnosed in line with the recommendations of the American College of Rheumatology. All the patients with SLE treated at the Outpatient Rheumatology Clinic received invitations to ophthalmological examinations. The studied group comprised individuals who attended the examinations and did not meet the exclusion criteria for the study. The authors of this paper did not modify nor model the risk factors for poststeroid glaucoma, which include systemic GC therapy and immunosuppressive treatment. Moreover, all SLE patients were treated according to the recommendations of the European League Against Rheumatism (EULAR).
The literature also describes gene expression of specific cellular components in the glycosaminoglycan composition with decreased hyaluronic acid and an increased deposition of chondroitin sulfate and glycosaminoglycogenase resistant material. It cannot be excluded, that the key mechanism of hypertension are the changes leading to altered cytoskeleton architecture due to cross-linked actin networks present in the TM tissue. All the processes mentioned above result in an increased outflow resistance of aqueous humor. Also, GC may cause morphological changes in the TM cellsthe GRs,which belongs to a super family of highly conserved proteins including receptors for mineralocorticosteroids, androgens,estrogens, thyroid hormone, retinoic acid, progestins and vitamin D. Since these receptors bind to and modulate specific gene promoters they have also been termed liganddependent transcriptions factors. The interaction of GC with the receptor is complex. Specific mechanisms involve the translocation of the activated GRs to the nucleus and GC response elements (GREs), sGREs, and nGREs as well as coactivators to elicit gene expression. Nuclear transcription factors associated with the GRE complex,gene locus and the expression of myocilin in the TM cells may also be involved in the hypothesis of SIG. Mutations ofare observed in 2%-4% of POAG patients. Thepromotor transcription is manipulated by 4-hydroxy estradiol, which is a metabolic product of 17βestradiol in TM. The CYP1B1 enzyme has an impact on 17βestradiol metabolism and its level. The mutation ofand the production of an enzyme with a decreased activity can lead to an increased level of 17βestradiol in TM cells. Consequently, the upregulation of myocillin expression may be found. A higher prevalence of POAG in postmenopausal women may confirm the thesis ofinvolvement in the etiology of glaucoma. Despite a long-term use of systemic GC in the analyzed group, ocular hypertension and SⅠG were not confirmed in performed tests(Tables 2-4).
對于餐廳包間和會議室類的小空間區域,風機盤管溫控面板設置在該區域的燈光面板位置,以便客人可以根據自己的需求進行現場調節溫度及風速。……
登錄APP查看全文
猜你喜歡
辦公室業務(2020年18期)2020-09-29 12:15:58
裝備制造技術(2020年12期)2020-05-22 09:25:38
勞動保護(2019年7期)2019-08-27 00:41:26
輔導員(2017年18期)2017-10-16 01:14:48
電子制作(2017年8期)2017-06-05 09:36:15
中國法學教育研究(2017年2期)2017-05-30 02:28:38
信息記錄材料(2016年4期)2016-03-11 15:22:54
浙江理工大學學報(自然科學版)(2015年8期)2015-03-01 02:54:39
江蘇第二師范學院學報(2014年2期)2014-04-16 03:10:09
江蘇高職教育(2014年4期)2014-02-28 11:40:57
 International Journal of Ophthalmology
2022年1期
International Journal of Ophthalmology
2022年1期
- International Journal of Ophthalmology的其它文章
- lnstructions for Authors
- Comment on: Trends in research related to high myopia from 2010 to 2019: a bibliometric and knowledge mapping analysis
- Progress of clinical therapies for dry age-related macular degeneration
- Observation seasonal variation of intraocular pressure in young healthy volunteers
- Effectiveness of oral probiotics supplementation in the treatment of adult small chalazion
- Characterization and validation of a chronic retinal neovascularization rabbit model by evaluating the efficacy of anti-angiogenic and anti-inflammatory drugs