樹突狀細胞在心肌梗死及其修復重構中的作用*
2020-12-03 14:22:40張右銘劉海波
中國病理生理雜志 2020年11期
張右銘, 劉海波,2△
樹突狀細胞在心肌梗死及其修復重構中的作用*
張右銘1, 劉海波1,2△
(1同濟大學附屬東方醫院心內科,上海 200120;2復旦大學附屬中山醫院青浦分院心內科,上海 201700)
樹突狀細胞;心肌梗死;動脈粥樣硬化;缺血再灌注損傷;心肌重構
雖然隨著介入技術的發展,及時的再灌注治療降低了急性心肌梗死的死亡率,但心梗后心臟的缺血再灌注損傷及不良重構,導致患者發生慢性心力衰竭,生活質量急劇下降,對社會經濟造成了嚴重的負擔。所以如何預防心肌梗死和改善心梗后缺血損傷及不良重構引起的心力衰竭,提高患者預后及生存質量成了新的熱門研究話題。
目前的研究發現,炎癥與心肌梗死(myocardial infarction, MI)的發生發展關系密切,冠心病發生的根本原因是動脈粥樣硬化,目前研究表明炎癥參與了動脈粥樣硬化的整個進程[1],隨著慢性炎癥和脂質斑塊的累積,不斷緩慢進展,斑塊破裂或侵蝕導致血栓形成,阻塞血管并導致MI的發生,MI后,壞死凋亡的心肌細胞可激活損傷相關分子模式(damage-associated molecular patterns, DAMPs),通過釋放各種細胞因子及趨化因子,招募和激活各種免疫細胞,參與MI后心肌損傷的修復[2]。
樹突狀細胞(dendritic cells, DCs)作為重要的抗原呈遞細胞,能調節固有免疫和適應性免疫的各種炎癥細胞,從而在免疫反應中發揮重要的作用[3]。根據表面標志物的表達,DCs可以被粗略地分為經典樹突狀細胞(conventional dendritic cells, cDCs)及漿細胞樣樹突狀細胞(plasmacytoid dendritic cells, pDCs)兩大類,可用不同的表面標志物來區分,其中cDCs還可細分為cDCs1和cDCs2兩個亞型[4-6],詳見表1。不同的實驗使用了不同的方法來特異性清除小鼠體內的DCs或其亞型。近來,越來越多的實驗發現DCs在動脈粥樣硬化和MI后炎癥反應中發揮重要作用。因此,本文就DCs在MI全過程中各個階段的作用進行綜述,重點闡述DCs在動脈粥樣硬化、MI后心肌缺血再灌注損傷(myocardial ischemia-reperfusion injury, MI/RI)和心室重構中的作用。
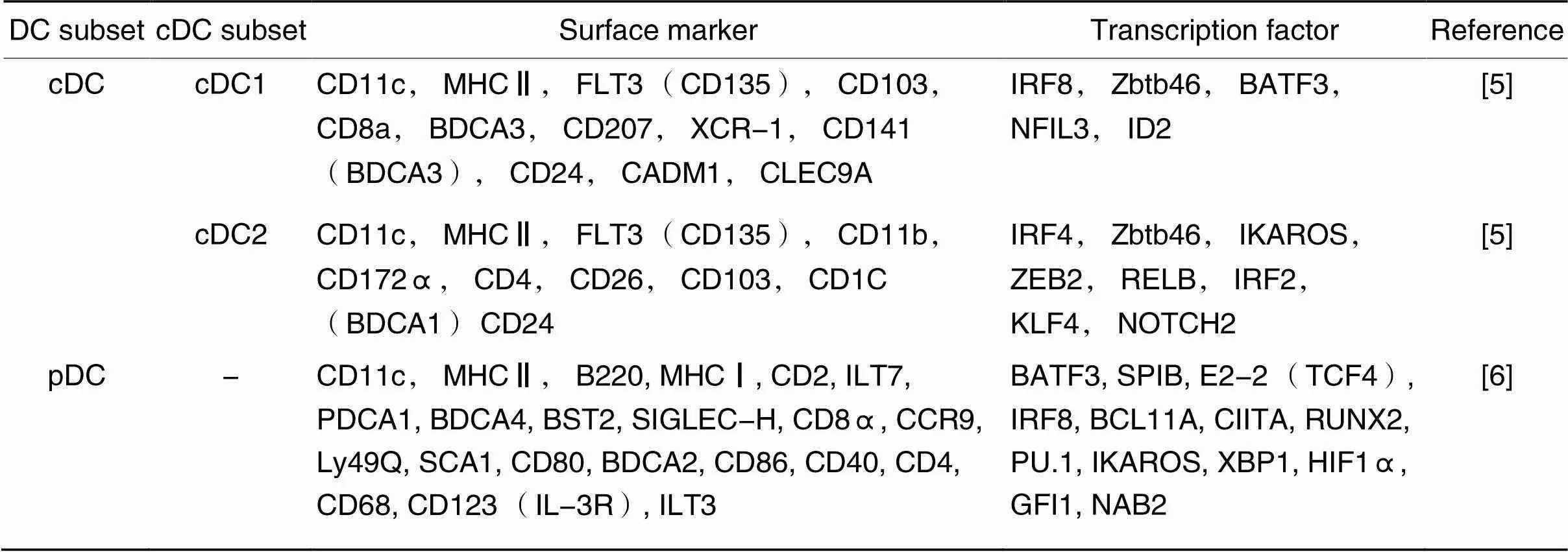
表1 DCs分類及常見表面標志物
1 DCs在動脈粥樣硬化中的作用
動脈粥樣硬化是一個復雜的終生過程,涉及先天和后天免疫反應及慢性炎癥,是引起缺血性心臟病和腦梗死最常見的原因[7]。動脈粥樣硬化斑塊的緩慢形成是無癥狀的,其特征是內皮功能障礙以及低密度脂蛋白(low-density lipoprotein, LDL)、免疫細胞和壞死碎片在內皮下間隙的積聚。內皮細胞激活觸發白細胞黏附分子的表達,后者通過CCR2發出信號,刺激炎癥性單核細胞的遷移和浸潤[8]。沉積在內膜的LDL可被進一步氧化修飾為氧化低密度脂蛋白(oxidized low-density lipoprotein, oxLDL),發揮抗原作用,被吞噬形成泡沫細胞后,可引發動脈粥樣硬化的形成,在這一過程中,巨噬細胞占主導作用[9]。雖然巨噬細胞在動脈粥樣硬化的細胞浸潤中占主導地位,但研究人員在小鼠動脈粥樣硬化模型的主動脈內膜[10]和斑塊內[11],均發現了CD11c+MHCII+DCs的聚集。并且,在人類的動脈內膜中[12]和斑塊內[13]也可找到大量CD1α+、CD83+及CD86+DCs,其主要存在于斑塊肩部以及斑塊核心的邊緣部位[13-14]。同樣有研究表明,在人為制造高膽固醇血癥幾天后,低密度脂蛋白受體基因敲除(low-density lipoprotein receptor gene knockout,-/-)小鼠的內膜血管CD11c+DCs內就可以發現脂質的積聚,并呈現泡沫細胞樣外觀,參與早期階段斑塊的形成[15]。還有研究發現,無論在-/-小鼠模型或載脂蛋白E基因敲除(apolipoprotein E gene knockout,-/-)小鼠模型中,耗竭CD11c+DCs都會導致血漿總膽固醇水平的升高。人為延長-/-或-/-小鼠模型中DCs壽命和免疫原性后,血漿LDL和極低密度脂蛋白(very-low-density lipoprotein, VLDL)水平明顯降低,但與對照組相比,小鼠動脈粥樣硬化斑塊的大小并沒有明顯改變[16]。這一過程的具體分子機制尚不清楚,不過可以看出DCs同樣具有攝取脂質的能力并參與泡沫細胞的形成。
此外,也有研究發現,人X組分泌磷脂酶A2修飾的低密度脂蛋白(low-density lipoprotein modified by human group X-secreted phospholipase A2, LDLx)和oxLDL可通過DCs激活T細胞[17],提呈抗原并啟動特異性免疫被認為是DCs在動脈粥樣硬化中的重要功能。先前研究發現,分離的主動脈CD11c+DCs暴露于血液中的抗原后,可在體外誘導抗原特異性T細胞增殖[18-19],并且主動脈CD11c+DCs可在體外促進抗原T細胞產生腫瘤壞死因子α (tumor necrosis factor-α,TNF-α)和干擾素γ (interferon-γ, IFN-γ)[20],提示DCs可引起局部T細胞的活化和促炎細胞因子的產生。
不過,DCs對動脈粥樣硬化起抑制還是促進的作用卻存在爭議。有實驗報道人為刪除-/-小鼠中的CD74 (一種參與MHCⅡ復合物形成的關鍵蛋白),間接減少DCs的數量后,發現T細胞的激活及斑塊的形成減少了[21]。然而,另一實驗發現在人為制造的-/--/-小鼠中,起保護起作用的調節性T細胞(regulatory T cells, Treg)減少,促動脈粥樣硬化的CD8+T細胞增加,最終促進了動脈粥樣硬化斑塊的形成[22]。
同樣的矛盾結果還體現在對DCs亞型功能的研究中。有研究將含鋅指及BTB結構域蛋白46 (zinc finger and BTB domain containing 46,)-白喉毒素受體(diphthera toxin receptor,)轉基因小鼠的骨髓移植到-/-小鼠模型中,注射白喉毒素選擇性清除-/-小鼠體內cDCs,發現斑塊大小不受影響[23]。但在利用FMS樣酪氨酸激酶3 (FMS-like tyrosine kinase, Flt3)制造-/--/-小鼠模型、特異性耗竭CD103+cDCs的實驗中,發現小鼠體內Treg減少,加重了動脈粥樣硬化,提示cDCs對動脈粥樣硬化有抑制作用[24]。同樣,在利用堿性亮氨酸拉鏈ATF樣轉錄因子3 (basic leucine zipper ATF-like transcription factor 3, Batf3)制造-/--/-小鼠模型、特異性耗竭cDCs的實驗中,斑塊大小沒有明顯變化[25]。但在基于-/--/-小鼠模型的實驗中卻發現cDCs可以通過刺激Th1細胞來促進動脈粥樣硬化斑塊形成[26]。在針對pDCs的實驗中,使用大量抗骨髓基質細胞抗原2 (bone marrow stromal antigen 2, BST2)的抗體來清除pDCs,發現清除pDCs促進了-/-小鼠的動脈粥樣硬化[27],但減輕了-/-小鼠的動脈粥樣硬化[28]。同樣,有研究將血樹突狀細胞抗原2 (blood dendritic cell antigen 2,)-轉基因小鼠的骨髓移植到-/-小鼠模型中,注射白喉毒素選擇性清除-/-小鼠體內pDCs,發現清除pDCs促進了斑塊發展[29],但在-/--小鼠模型中,斑塊大小沒有變化[30]。
造成這些差異的原因目前尚不清楚,不過由于-/-和-/-小鼠模型中脂質分布的不同和對免疫細胞效應的不同,兩者有各自的優缺點[31],所以造成這些相互矛盾結果的原因可能是由于小鼠模型的不同。此外,于永慧等[32]發現,不同階段-/-小鼠的炎癥基因存在差異化表達且不同周齡-/-小鼠中炎癥因子表達情況有顯著差異。因此不同實驗中小鼠模型周齡的不同也可能是造成不同結果的重要因素。另外,考慮到用來標記DCs及其亞型的分子(如MHCⅡ、CD103、CD8a等)也可以被其他免疫細胞表達,因此不能排除受到了其他免疫細胞的影響。并且由于模型的限制,無法維持長期的特異性耗竭,也無法有效評價DCs及其亞型在慢性炎癥中的作用,更有效的特異性耗竭DCs及其亞型的辦法仍需進一步研究。
2 DCs在MI/RI中的作用
隨著介入技術的發展,MI患者的生存率大大提高,然而,缺血心肌的血流恢復過程亦會引起損傷,這種現象被稱為MI/RI,它會降低心肌再灌注的有益影響[33]。MI/RI的發病機制很復雜,炎癥反應在這一過程中扮演了重要角色。除了中性粒細胞、巨噬細胞和淋巴細胞外, DCs在缺血再灌注損傷中也發揮了重要作用。已有文獻報道,人DCs中P2Y11受體具有免疫抑制作用,P2Y11受體激動劑可以減輕缺血再灌注過程中的炎癥反應并保護缺血器官[34]。但也有研究發現,在大鼠心肌缺血再灌注過程中,CD1a+CD80+DCs向心肌的遷移、黏附和聚集增加,加重了心肌損傷[35]。
不過,目前針對DCs在MI/RI中作用的研究相對較少,尚未能有確切的結論。但在小鼠研究中有一致的證據表明,促炎CD4+T細胞的浸潤加重了MI/RI。除了CD4+T細胞外, CD8+記憶T細胞亞群在再灌注開始后早期就聚集在冠狀動脈微循環中,可能參與到再灌注過程中,對心肌產生損害[36-37]。考慮到DCs作為強大的抗原提呈細胞,是特異性免疫應答的始動者,所以在MI/RI過程中,各類T細胞的浸潤很大可能是通過DCs發動。已有證據表明,在肝臟、腎臟等器官移植時發生的缺血再灌注損傷中, DCs可以激活T細胞,加強炎癥對再灌注后組織的損傷[38-39]。
亦有實驗發現,在結扎小鼠冠狀動脈后,壞死心肌和正常心肌之間的梗死邊界區內CD11c+DCs數量明顯增加,并且和CD4+T細胞形成集落[40]。這些實驗均提示在MI時, DCs與T細胞有某種聯系,但其確鑿的實驗證據和內在的分子機制仍有待進一步研究。
3 DCs在心室重構中的作用
MI后左室重構是一個復雜的心肌結構改變過程,不良左室重構嚴重影響患者的預后。已有大量研究表明,炎癥在心肌梗死愈合和隨后的左室重構中起著至關重要的作用[41-42]。
Anzai等[43]的研究設計了條件性DCs敲除小鼠,將人DTR結合在DCs的啟動子區域,在小鼠MI術前采用注射白喉毒素的方法完全清除小鼠體內的CD11c+DCs,發現在DCs敲除小鼠MI模型中,其左室重構較對照組明顯惡化,雖然病理檢查未顯示梗死面積有明顯區別,但DCs敲除小鼠梗死區域心臟壁更薄,并且新生血管受損。他們更深入的研究發現,梗死區及周邊區域浸潤高表達Ly6C (Ly6Chigh)的單核細胞和M1型巨噬細胞明顯增加,而低表達Ly6C (Ly6Clow)的單核細胞和M2型巨噬細胞顯著降低,并且在DCs敲除MI模型小鼠中,炎癥因子和MMP-9的表達也明顯增高,而抗炎因子IL-10卻顯著降低。這些研究結果表明DCs敲除后通過激活炎癥單核細胞和M1型巨噬細胞及抑制抗炎單核細胞和M2型巨噬細胞,增強了炎癥反應及細胞外基質的降解,從而延緩MI后的心臟愈合,導致心功能惡化。這些研究提示DCs可通過調節單核細胞和巨噬細胞的動態平衡及轉化而起到抑制心臟重構的作用。
有研究對ST段抬高心肌梗死死亡患者進行尸檢,發現心臟破裂組與非破裂組相比, CD68+巨噬細胞浸潤增加, CD209+DCs和CD11c+DCs浸潤及修復性纖維化程度較低,提示心梗部位DCs數量的減少與巨噬細胞浸潤增加會使修復性纖維化受損,增加心肌梗死后心臟破裂的風險,表明DCs在心肌梗死后炎癥及隨后的愈合過程中具有保護作用[44]。我們前期的研究發現,MI小鼠模型中CD11c+DCs產生的外泌體可將CD4+輔助性T細胞招募到心肌梗死區,并有助于預防心肌梗死后的左心室不良重構[45]。這些結果均提示DCs在MI后炎癥反應和隨后的左心室重構中具有心肌保護作用,但具體針對DCs各亞型的功能,不同實驗報告了不同的結果。
有研究利用-重組小鼠,注射白喉毒素選擇性地清除CD103+及CD11b+cDCs,發現與對照組相比,選擇性清除cDCs顯著減少了MI后心肌損傷的范圍,且能預防心室不良重構,改善心功能,表明cDCs不利于MI后心肌損傷的恢復及心功能的改善,加重了心室不良重構[46]。但也有實驗發現,心肌梗死后, XCR-1+CD172α+cDCs浸潤心肌,攝取壞死心肌細胞釋放的α-肌球蛋白碎片,逐漸遷移到縱膈淋巴結中并將心臟自身抗原提呈給CD4+T細胞,并最終引起Treg的增殖[47]。活化的Treg可通過增加巨噬細胞精氨酸酶1、IL-13、骨橋蛋白及TGF-β的表達而誘導巨噬細胞向M2型分化,從而抑制了MI后的心臟重構[48];而耗竭Treg可加速心肌梗死后心室的擴張,加重心室重構[49]。由此可以推測cDCs對心室功能有保護作用。
為了探討pDCs的作用,研究者在-重組小鼠中注射白喉毒素選擇性地耗竭pDCs,發現對MI后心功能沒有影響,其作用可能在于產生I型干擾素并保護組織免受病毒感染,在MI后心臟修復的過程中并不重要[46]。
整體來說,DCs在預防心室不良重構方面發揮了積極的作用,但在針對DCs不同亞群的研究中,不同實驗卻得出了矛盾的結論,有待進一步研究。
4 基于DCs的免疫療法
近年來,人們越來越意識到炎癥在整個心梗過程中的重要性,研究人員一直以來都嘗試開發基于免疫炎癥的新型療法,并且已收獲很多成果[50-52]。DCs作為免疫調控的中心環節,深入參與了MI發生發展的全過程,因此基于DCs的免疫療法潛力巨大。
將攜帶人載脂蛋白B100 (apolipoprotein B100, ApoB100)的致耐受樹突狀細胞(tolerogenic dendritic cells, tDCs)導入-/-小鼠中,使之成為具有人基因的轉基因-/-小鼠(tg×-/-小鼠),可顯著降低小鼠體內效應T細胞的數量并誘導Treg的增殖,從而顯著延緩動脈粥樣硬化病變的發展[53]。這提示基于DCs的免疫治療可以延緩動脈粥樣硬化的發展,在預防MI方面有極大潛力。同樣,李大主等[54]將攜帶熱休克蛋白60 (heat shock protein 60, HSP60)的tDCs接種至-/-小鼠后,發現小鼠動脈粥樣硬化斑塊中的炎癥反應和斑塊的進展受到抑制。后續有研究者發現,經典調脂藥物——他汀類藥物可以通過抑制人CD83+CD86+DCs中的miRNA let-7c來抑制oxLDL誘導DCs的成熟,進而抑制DCs促進T細胞增殖的能力,從而影響動脈粥樣硬化斑塊的發生和發展[55]。這揭示了他汀類藥物治療動脈粥樣硬化時還具有免疫治療方面的作用。最近,研究者基于CX3CL1/CX3CR1通路開發了一種針對CX3CR1的DCs靶向DNA疫苗,該疫苗通過將質粒與針對DCs的限制性抗原攝取受體DEC205的單鏈Fv抗體(scFv)結合,從而將質粒特異性提供給DCs,增強接種效果,并用于小鼠動脈粥樣硬化模型。研究發現,注射修飾后的DEC205-CX3CR1 DNA疫苗顯著減少了小鼠斑塊處巨噬細胞的浸潤,減小了小鼠粥樣硬化斑塊的大小,對動脈粥樣硬化具有顯著的抑制作用[56]。研究者已建議使用DNA疫苗阻斷CX3CR1通路的方法作為目前動脈粥樣硬化治療方法的補充。
有研究者發現,刺激人DCs內的P2Y11受體對MI/RI具有保護作用,在器官移植和急性MI后的MI/RI期間, P2Y11受體激動劑藥物可以提供有益幫助[34]。此外,有研究者發現,高遷移率族蛋白B1(high mobility group protein B1, HMGB1)作為MI/RI后心肌損傷產生的DAMPs,通過Toll樣受體4 (Toll-like receptor 4, TLR4)通路激活CD1a+CD80+DCs,影響其在心肌中的分布,誘導DCs活化和成熟。并且,使用HMGB1中和抗體可提供明顯的心臟保護[35]。所以說,基于DCs的免疫療法在減輕MI/RI方面亦有重要作用。
早期有研究通過敲除小鼠白細胞介素1受體相關激酶4 (interleukin-1 receptor-associated kinase 4,-)基因,消除CD11c+DCs動員、捕獲抗原、成熟及產生細胞因子的能力,從而使--/-MI模型小鼠心功能及心室不良重構獲得改善,存活率提高[57]。使用TNF-α和心臟抗原刺激骨髓源性樹突狀細胞(bone marrow-derived dendritic cells, BMDCs)以制備tDC,再向MI小鼠模型中注入tDC,可激活小鼠體內的Treg,進而促進早期巨噬細胞亞群從炎性M1型轉換為修復性M2型,并增加新生血管的生成,從而減少梗死面積,提升左室功能[52]。除此之外,我們前期的研究還發現,通過體外給予MI模型小鼠CD11c+DCs分泌的外泌體治療,可以激活CD4+T淋巴細胞并改善心臟功能[45]。同樣,經典藥物血管緊張素轉化酶抑制劑對CD11c+DCs介導的免疫炎癥反應也有抑制作用,可以減輕MI后的炎癥反應,從而改善心室功能,提高生存率[58]。
各種實驗結果均表明,基于DCs的免疫療法有十分光明的前景,相信隨著后續研究的不斷探索,免疫治療將在MI的預防與治療中發揮重要作用。
5 總結與展望
DCs在心肌梗死的發生和發展的各個階段都發揮著重要的作用,但現階段的研究對其在各個階段中的具體作用及相應的分子機制,尚不能達成共識,仍需進一步研究。基于DCs的免疫療法前景廣闊,目前已取得一定成果,這為延緩動脈粥樣硬化的發展、減輕急性心肌梗死后缺血再灌注損傷和預防心臟不良重構提供了全新的思路,具有巨大臨床應用潛力。
[1] Gistera A, Hansson GK. The immunology of atherosclerosis[J]. Nat Rev Nephrol, 2017, 13(6):368-380.
[2] Frangogiannis NG. The inflammatory response in myocardial injury, repair, and remodelling [J]. Nat Rev Cardiol, 2014, 11(5):255-265.
[3] Worbs T, Hammerschmidt SI, Forster R. Dendritic cell migration in health and disease[J]. Nat Rev Immunol, 2017, 17(1):30-48.
[4] Guilliams M, van de Laar L. A Hitchhiker's guide to myeloid cell subsets: practical implementation of a novel mononuclear phagocyte classification system[J]. Front Immunol, 2015, 6:406.
[5] Sichien D, Lambrecht BN, Guilliams M, et al. Development of conventional dendritic cells: from common bone marrow progenitors to multiple subsets in peripheral tissues[J]. Mucosal Immunol, 2017, 10(4):831-844.
[6] Swiecki M, Colonna M. The multifaceted biology of plasmacytoid dendritic cells[J]. Nat Rev Immunol, 2015, 15(8):471-485.
[7] Herrero-Fernandez B, Gomez-Bris R,Somovilla-Crespo B, et al. Immunobiology of atherosclerosis: a complex net of interactions[J]. Int J Mol Sci, 2019, 20(21):5293.
[8] Gil-Pulido J, Zernecke A. Antigen-presenting dendritic cells in atherosclerosis [J]. Eur J Pharmacol, 2017, 816:25-31.
[9] Back M, Yurdagul A, Jr., Tabas I, et al. Inflammation and its resolution in atherosclerosis: mediators and therapeutic opportunities [J]. Nat Rev Cardiol, 2019, 16(7):389-406.
[10] Busch M, Westhofen TC, Koch M, et al. Dendritic cell subset distributions in the aorta in healthy and atherosclerotic mice[J]. PLoS One, 2014, 9(2):e88452.
[11] Sage AP, Murphy D, Maffia P, et al. MHC Class II-restricted antigen presentation by plasmacytoid dendritic cells drives proatherogenic T cell immunity[J]. Circulation, 2014, 130(16):1363-1373.
[12] Millonig G, Niederegger H, Rabl W, et al.Network of vascular-associated dendritic cells in intima of healthy young individuals[J]. Arterioscler Thromb Vasc Biol, 2001, 21(4):503-508.
[13] Yilmaz A, Lochno M, Traeg F, et al. Emergence of dendritic cells in rupture-prone regions of vulnerable carotid plaques[J]. Atherosclerosis, 2004, 176(1):101-110.
[14] Erbel C, Sato K, Meyer FB, et al.Functional profile of activated dendritic cells in unstable atherosclerotic plaque[J]. Basic Res Cardiol, 2007, 102(2):123-132.
[15] Paulson KE, Zhu SN, Chen M, et al. Resident intimal dendritic cells accumulate lipid and contribute to the initiation of atherosclerosis[J]. Circ Res, 2010, 106(2):383-390.
[16] Gautier EL, Huby T, Saint-Charles F, et al. Conventional dendritic cells at the crossroads between immunity and cholesterol homeostasis in atherosclerosis[J]. Circulation, 2009, 119(17):2367-2375.
[17] Liu A, Ming JY, Fiskesund R, et al. Induction of dendritic cell-mediated T-cell activation by modified but not native low-density lipoprotein in humans and inhibition by annexin a5: involvement of heat shock proteins[J]. Arterioscler Thromb Vasc Biol, 2015, 35(1):197-205.
[18] Weber C, Meiler S, Doring Y, et al. CCL17-expressing dendritic cells drive atherosclerosis by restraining regulatory T cell homeostasis in mice [J]. J Clin Invest, 2011, 121(7):2898-2910.
[19] Choi JH, Do Y, Cheong C, et al. Identification of antigen-presenting dendritic cells in mouse aorta and cardiac valves[J]. J Exp Med, 2009, 206(3):497-505.
[20] Koltsova EK, Garcia Z, Chodaczek G, et al. Dynamic T cell-APC interactions sustain chronic inflammation in atherosclerosis[J]. J Clin Invest, 2012, 122(9):3114-3126.
[21] Sun J, Hartvigsen K, Chou MY, et al. Deficiency of antigen-presenting cell invariant chain reduces atherosclerosis in mice[J]. Circulation, 2010, 122(8):808-820.
[22] Wigren M, Rattik S, Yao Mattisson I, et al. Lack of ability to present antigens on major histocompatibility complex class II molecules aggravates atherosclerosis in-/-mice[J]. Circulation, 2019, 139(22):2554-2566.
[23] Rombouts M, Cools N, Grootaert MO, et al. Long-term depletion of conventional dendritic cells cannot be maintained in an atherosclerotic Zbtb46-DTR mouse model[J]. PLoS One, 2017, 12(1):e0169608.
[24] Choi JH, Cheong C, Dandamudi DB, et al. Flt3 signaling-dependent dendritic cells protect against atherosclerosis[J]. Immunity, 2011, 35(5):819-831.
[25] Gil-Pulido J, Cochain C, Lippert MA, et al. Deletion of Batf3-dependent antigen-presenting cells does not affect atherosclerotic lesion formation in mice[J]. PLoS One, 2017, 12(8):e0181947.
[26] Li Y, Liu X, Duan W, et al. Batf3-dependent CD8α+dendritic cells aggravates atherosclerosis via Th1 cell induction and enhanced CCL5 expression in plaque macrophages[J]. EBioMedicine, 2017, 18:188-198.
[27] Daissormont IT, Christ A, Temmerman L, et al. Plasmacytoid dendritic cells protect against atherosclerosis by tuning T-cell proliferation and activity[J]. Circ Res, 2011, 109(12):1387-1395.
[28] Macritchie N, Grassia G, Sabir SR, et al. Plasmacytoid dendritic cells play a key role in promoting atherosclerosis in apolipoprotein E-deficient mice [J]. Arterioscler Thromb Vasc Biol, 2012, 32(11):2569-2579.
[29] Yun TJ, Lee JS, Machmach K, et al. Indoleamine 2,3-dioxygenase-expressing aortic plasmacytoid dendritic cells protect against atherosclerosis by induction of regulatory T cells[J]. Cell Metab, 2016, 23(5):852-866.
[30] Mandl M, Drechsler M, Jansen Y, et al. Evaluation of the BDCA2-DTR transgenic mouse model in chronic and acute inflammation[J]. PLoS One, 2015, 10(8):e0134176.
[31] Getz GS, Reardon CA. Do the-/-and-/-mice yield the same insight on atherogenesis?[J]. Arterioscler Thromb Vasc Biol, 2016, 36(9):1734-1741.
[32] 于永慧,董瑞紅,劉劍剛,等. 不同階段-/-小鼠動脈粥樣硬化炎癥差異基因表達的比較研究[J]. 中國病理生理雜志, 2019, 35(9):1694-1699.
Yu YH, Dong RH, Liu JG, et al. Preliminary comparison of inflammatory differential gene expression during atherosclerosis in-/-mice[J]. Chin J Pathophysiol, 2019, 35(9):1694-1699.
[33] Yellon DM, Hausenloy DJ. Myocardial reperfusion injury[J]. N Engl J Med, 2007, 357(11):1121-1135.
[34] Chadet S, Ivanes F, Benoist L, et al. Hypoxia/reoxygenation inhibits P2Y11 receptor expression and its immunosuppressive activity in human dendritic cells[J]. J Immunol, 2015, 195(2):651-660.
[35] Xue J, Ge H, Lin Z, et al. The role of dendritic cells regulated by HMGB1/TLR4 signalling pathway in myocardial ischaemia reperfusion injury[J]. J Cell Mol Med, 2019, 23(4):2849-2862.
[36] Boag SE, Das R, Shmeleva EV, et al. T lymphocytes and fractalkine contribute to myocardial ischemia/reperfusion injury in patients[J]. J Clin Invest, 2015, 125(8):3063-3076.
[37] Hoffmann J, Shmeleva EV, Boag SE, et al. Myocardial ischemia and reperfusion leads to transient CD8 immune deficiency and accelerated immunosenescence in CMV-seropositive patients[J]. Circ Res, 2015, 116(1):87-98.
[38] Funken D, Ishikawa-Ankerhold H, Uhl B, et al.targeting of dendritic cells sets tolerogenic environment and ameliorates CD4+T-cell response in the postischemic liver[J]. FASEB J, 2017, 31(11):4796-4808.
[39] Ozaki KS, Kimura S, Nalesnik MA, et al. The loss of renal dendritic cells and activation of host adaptive immunity are long-term effects of ischemia/reperfusion injury following syngeneic kidney transplantation[J]. Kidney Int, 2012, 81(10):1015-1025.
[40] Anzai A, Anzai T, Nagai S, et al. Regulatory role of dendritic cells in postinfarction healing and left ventricular remodeling[J]. Circulation, 2012, 125(10):1234-1245.
[41] Santos-Zas I, Lemarié J, Tedgui A, et al. Adaptive immune responses contribute to post-ischemic cardiac remodeling[J]. Front Cardiovasc Med, 2018, 5:198.
[42] Rhee AJ, Lavine KJ. New approaches to target inflammation in heart failure: harnessing insights from studies of immune cell diversity[J]. Annu Rev Physiol, 2020, 82:1-20.
[43] Anzai A, Anzai T, Nagai S, et al. Regulatory role of dendritic cells in postinfarction healing and left ventricular remodeling[J]. Circulation, 2012, 125(10):1234-1245.
[44] Nagai T, Honda S, Sugano Y, et al. Decreased myocardial dendritic cells is associated with impaired reparative fibrosis and development of cardiac rupture after myocardial infarction in humans[J]. J Am Heart Assoc, 2014, 3(3):e000839.
[45] Liu H, Gao W, Yuan J, et al. Exosomes derived from dendritic cells improve cardiac function via activation of CD4+T lymphocytes after myocardial infarction[J]. J Mol Cell Cardiol, 2016, 91:123-133.
[46] Lee JS, Jeong SJ, Kim S, et al. Conventional dendritic cells impair recovery after myocardial infarction[J]. J Immunol, 2018, 201(6):1784-1798.
[47] Van der Borght K, Scott CL, Nindl V, et al. Myocardial infarction primes autoreactive T cells through activation of dendritic cells[J]. Cell Rep, 2017, 18(12):3005-3017.
[48] Weirather J, Hofmann UD, Beyersdorf N, et al. Foxp3+CD4+T cells improve healing after myocardial infarction by modulating monocyte/macrophage differentiation[J]. Circ Res, 2014, 115(1):55-67.
[49] Saxena A, Dobaczewski M, Rai V, et al. Regulatory T cells are recruited in the infarcted mouse myocardium and may modulate fibroblast phenotype and function[J]. Am J Physiol Heart Circ Physiol, 2014, 307(8):H1233-H1242.
[50] Rymer JA, Newby LK. Failure to launch: targeting inflammation in acute coronary syndromes[J]. JACC Basic Transl Sci, 2017, 2(4):484-497.
[51] Adamo L, Staloch LJ, Rocha-Resende C, et al. Modulation of subsets of cardiac B lymphocytes improves cardiac function after acute injury[J]. JCI Insight, 2018, 3(11):e120137.
[52] Choo EH, Lee JH, Park EH, et al. Infarcted myocardium-primed dendritic cells improve remodeling and cardiac function after myocardial infarction by modulating the regulatory T cell and macrophage polarization[J]. Circulation, 2017, 135(15):1444-1457.
[53] Hermansson A, Johansson DK, Ketelhuth DF, et al. Immunotherapy with tolerogenic apolipoprotein B-100-loaded dendritic cells attenuates atherosclerosis in hypercholesterolemic mice[J]. Circulation, 2011, 123(10):1083-1091.
[54] 李大主,周游,吳偉,等. 負載熱休克蛋白60的致耐受性樹突狀細胞疫苗對小鼠動脈粥樣硬化斑塊的影響[J]. 中國病理生理雜志, 2006, 22(6):1079-1082.
Li DZ, Zhou Y, Wu W, et al. Effects of rapamycin-treated HSP60-pulsed dendritic cells on the progression of the atherosclerotic plaque in mice[J]. Chin J Pathophysiol, 2006, 22(6):1079-1082.
[55] Frostegard J, Zhang Y, Sun J, et al. Oxidized low-density lipoprotein (OxLDL)-treated dendritic cells promote activation of T cells in human atherosclerotic plaque and blood, which is repressed by statins: microRNA let-7c is integral to the effect[J]. J Am Heart Assoc, 2016, 5(9):e003976.
[56] Zhou JJ, Wang YM, Lee VWS, et al. DEC205-DC targeted DNA vaccine against CX3CR1 protects against atherogenesis in mice[J]. PLoS One, 2018, 13(4):e0195657.
[57] Maekawa Y, Mizue N, Chan A, et al. Survival and cardiac remodeling after myocardial infarction are critically dependent on the host innate immune interleukin-1 receptor-associated kinase-4 signaling: a regulator of bone marrow-derived dendritic cells[J]. Circulation, 2009, 120(14): 1401-1414.
[58] Ma Y, Yuan J, Hu J, et al. ACE inhibitor suppresses cardiac remodeling after myocardial infarction by regulating dendritic cells and AT2 receptor-mediated mechanism in mice[J]. Biomed Pharmacother, 2019, 114:108660.
Role of dendritic cells in myocardial infarction and cardiac remodeling
ZHANG You-ming1, LIU hai-bo1,2△
(1,,,200120,;2,,,201700,)
Myocardial infarction (MI) is one of the leading causes of death worldwide. One of the primary reasons is that the rupture of atherosclerotic plaque leads to the formation of thrombosis, and then interrupts the coronary blood flow, thus finally causing the death of myocardial cells and cardiac dysfunction. A large number of researches have revealed that dendritic cells (DCs) play an essential role in immune inflammatory responses in the occurrence and development of atherosclerosis and MI. This article reviews the role of DCs in atherosclerosis, myocardial ischemia/reperfusion injury and cardiac remodeling after MI, and shows the potential values of DCs as an immunotherapeutic strategy for MI.
Dendritic cells; Myocardial infarction; Atherosclerosis; Ischemia/reperfusion injury; Myocardial remodeling
R542.2+1; R363.2
A
10.3969/j.issn.1000-4718.2020.11.025
1000-4718(2020)11-2093-06
2020-04-12
2020-05-21
國家自然科學基金資助項目(No.81770350)
Tel: 021-67009999; E-mail: haiboliu13@fudan.edu.cn
(責任編輯:宋延君,羅森)
猜你喜歡
興趣閱讀·興趣作文與閱讀(低年級)(2025年8期)2025-08-18 00:00:00
體育科技文獻通報(2022年3期)2022-05-23 13:46:54
天津外國語大學學報(2021年3期)2021-08-13 08:32:18
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
學苑創造·A版(2020年9期)2020-10-13 09:41:02
科技傳播(2019年22期)2020-01-14 03:06:54
民用飛機設計與研究(2019年4期)2019-05-21 07:21:24
小學生學習指導(低年級)(2017年10期)2017-10-10 01:00:05
汽車工程學報(2017年2期)2017-07-05 08:13:02
云南中醫學院學報(2014年3期)2014-07-31 18:57:34