RASSF10基因啟動子區甲基化狀態在宮頸癌中的臨床應用
2019-09-29 06:54:17汪學昌段婧
中國現代醫生 2019年21期
汪學昌 段婧
[摘要] 目的 探討RASSF10基因啟動子區甲基化狀態在宮頸癌中的臨床意義。 方法 收集本院2005年6月~2013年12月經術后病理證實的70例宮頸癌患者,取其經手術切除癌組織70例和配對癌旁組織標本70例,采用甲基化特異性PCR(MSP)分析法檢測RASSF10基因啟動子區DNA甲基化狀態,分析RASSF10基因啟動子區甲基化狀態與臨床病理特征(年齡、腫瘤大小、頸深部間質侵犯、盆腔淋巴結轉移、FIGO分期及腫瘤分級程度)的關系及宮頸癌預后的相關性因素分析。 結果 MSP檢測發現宮頸癌組織中RASSF10基因啟動子區甲基化為38.6%,未甲基化為43例(61.4%),而正常宮頸組織未見甲基化;宮頸癌中RASSF10基因啟動子甲基化狀態與年齡、腫瘤大小、頸深部間質侵犯及盆腔淋巴結轉移無關(P>0.05),而與FIGO分期及腫瘤分化程度有關。70例宮頸癌患者的中位生存期與年齡、腫瘤大小及頸深部間質侵犯無關,但與FIGO分期、腫瘤分化程度、盆腔淋巴結轉移及RASSF10基因啟動子區甲基化有關,其中RASSF10基因啟動子區甲基化者5年生存率為66.7%,未甲基化者的5年生存率為88.4%,差異具有統計學意義(P<0.05)。多因素分析結果顯示FIGO 分期、腫瘤分化程度、盆腔淋巴結轉移和RASSF10基因啟動子區甲基化狀態為本組宮頸癌患者預后獨立因素。 結論 RASSF10基因啟動子區甲基化在宮頸癌中高表達,且與FIGO分期、腫瘤分化程度及預后有關,可作為宮頸癌預后的參考指標。
[關鍵詞] 宮頸癌;RASSF10;甲基化狀態;MSP分析法
[中圖分類號] R737.33? ? ? ? ? [文獻標識碼] B? ? ? ? ? [文章編號] 1673-9701(2019)21-0082-04
Clinical application of methylation status of RASSF10 gene promoter region in cervical cancer
WANG Xuechang1? ?DUAN Jing2
1.Department of Oncology, the Fifth People's Hospital of Qinghai Province(Qinghai Cancer Hospital), Xining? ?810007, China; 2.Department of Ultrasound, the Fifth People's Hospital of Qinghai Province(Qinghai Cancer Hospital), Xining 810007, China
[Abstract] Objective To investigate the clinical significance of methylation status of RASSF10 gene promoter region in cervical cancer. Methods Seventy patients with cervical cancer who were confirmed by postoperative pathology from June 2005 to December 2013 were enrolled. 70 cases of surgically resected cancer tissues and 70 matched paracancerous tissues were selected for methylation-specific PCR. Methylation specific PCR(MSP) assay was used for DNA methylation status in the promoter region of RASSF10 gene. The relationship between the methylation status of RASSF10 gene promoter region and clinicopathological features(age, tumor size, deep cervical interstitial invasion, pelvic lymph node metastasis, FIGO stage and tumor grade) was analyzed. And the correlation factors of cervical cancer prognosis were analyzed. Results MSP assay showed that the methylation rate of promoter region of RASSF10 gene was 38.6% in cervical cancer tissues, and 43 cases(61.4%) were unmethylated, while no methylation was observed in normal cervical tissues. Methylation status of RASSF10 gene promoter in cervical cancer was not associated with age, tumor size, deep cervical interstitial invasion and pelvic lymph node metastasis(P>0.05), but was related to FIGO stage and tumor grade. The median survival of 70 patients with cervical cancer was not associated with age, tumor size, and deep interstitial invasion of the neck, but was associated with FIGO stage, tumor grade, pelvic lymph node metastasis, and methylation of the RASSF10 gene promoter region, in which the 5-year survival rate of RASSF10 gene promoter region was 66.7%, and the 5-year survival rate of unmethylated patients was 88.4%. The difference was statistically significant(P<0.05). Multivariate analysis showed that FIGO stage, tumor differentiation, pelvic lymph node metastasis and methylation status of RASSF10 gene promoter region were independent prognostic factors for cervical cancer patients. Conclusion The promoter methylation of RASSF10 gene is highly expressed in cervical cancer, and it is related to FIGO stage, tumor differentiation and prognosis. It can be used as a reference index for prognosis of cervical cancer.
[Key words] Cervical cancer; RASSF10; Methylation status; MSP analysis
宮頸癌是婦科常見的惡性腫瘤,位居女性惡性腫瘤第3位,死亡率和發病率較高[1-2]。近些年隨著診斷技術和治療方法的不斷改進,宮頸癌預后明顯改善,但遠期療效仍較差[3]。分子生物學研究發現HPV感染、環境、遺傳和表觀遺傳因素在宮頸癌發生過程中起重要作用[4]。表觀遺傳學是指基因表達的遺傳發生變化而本身的DNA并未發生變化。組蛋白甲基化是表觀遺傳學的重要組成之一,目前已經證明甲基化在染色體穩定性、基因表達、基因組印跡和轉錄沉默中起著關鍵作用,同樣也與腫瘤的發生密切相關[3]。研究表明RASSF10(Ras-association domain family 10,RASSF 10)基因在腫瘤發生過程中調節細胞周期及細胞凋亡,進而影響腫瘤分子生物學。目前發現RASSF10基因在多種腫瘤中例如食管鱗癌、結腸癌、肺癌等表達降低,究其原因與RASSF10基因啟動子區甲基化密切相關[5],RASSF10基因甲基化與腫瘤診斷和預后密切相關[6,7]。然而在宮頸癌中RASSF10基因表達及其甲基化狀態文獻研究相對較少。本研究探討RASSF10基因啟動子區甲基化狀態在宮頸癌中的臨床意義。
1 資料與方法
1.1一般資料
選擇青海省第五人民醫院2005年6月~2013年12月經術后病理證實為宮頸癌患者70例,組織類型均為鱗狀細胞癌,FIGO分期為Ⅰ~Ⅱa,年齡35~77歲,平均(52.12±4.12)歲;ECOG評分0~2分。本研究通過醫院倫理委員會審批通過,所有患者入組前均簽署知情同意書。
1.2 入組標準
(1)術后病理證實為FIGO Ⅰ~Ⅱa宮頸癌患者;(2)行根治性子宮切除術和雙側盆腔淋巴結清掃術的患者;(3)匹配手術標本和鄰近正常宮頸組織的患者;(4)臨床資料及隨訪資料完整。
1.3 排除標準
(1)姑息性手術患者;(2)術中證實有遠處轉移或腹膜播散的患者;(3)術后住院期間或術后1個月內死亡的患者。
1.4 甲基化特異性PCR
使用TrIZOL試劑盒(Invitrogen,Carlsbad,CA)從宮頸癌組織和正常宮頸組織中提取RNA。引物用于檢測RASSF10啟動子的甲基化(M)或未甲基化(U)等位基因:甲基化等位基因RASSF10 forwar(5-GGG-TATTTTGGGTAGAGTTAGAGC-3′),和reverse(5-AAACAAACTAAAAAACGACTACGAC - 3′);未甲基化等位基因RASSF10 forward(5′-GGGTATTTTGGGTAGAGTTAGAGTG-3′,reverse(5-AAAACAAACTAAAA-AACAACTACAAC-3′)。使用擴增產物TAGQ(甲基化特異性引物、退火溫度600°C、非甲基化特異性引物、退火溫度580℃)對MSP進行25個循環。后對MSP引物進行鑒定,以確定是否擴增出任何未飽和DNA,并通過直接測序某些PCR產物進一步證實MSP的特異性。用2%瓊脂糖凝膠進行PCR檢測。用Image J軟件計算宮頸腺癌組織中RASSF10基因啟動子區甲基化的相對值。RASSF10啟動子的甲基化被定義為宮頸腺癌組織的甲基化值不低于陽性對照值。
1.5 隨訪
對患者定期復查,術后第1年每3個月1次,第2年每6個月1次,以后每年1次。復查時記錄患者有無復發、轉移事件。隨訪方式為電話隨訪,隨訪截止時間2019年1月8日或總體生存期60個月(超過60個月按60個月計算)。總體生存期(OS)定義為從隨機化到任何原因的死亡時間或者最后隨訪時間。
1.6 統計學分析
采用SPSS20.0統計軟件包進行分析。計量資料以均數±標準差表示,計數資料采用率表示并行χ2檢驗,預后因素分析采用 Cox風險比例回歸模型。P<0.05為差異有統計學意義。
2 結果
2.1 本組宮頸癌組織中RASSF10基因啟動子區甲基化狀態表達
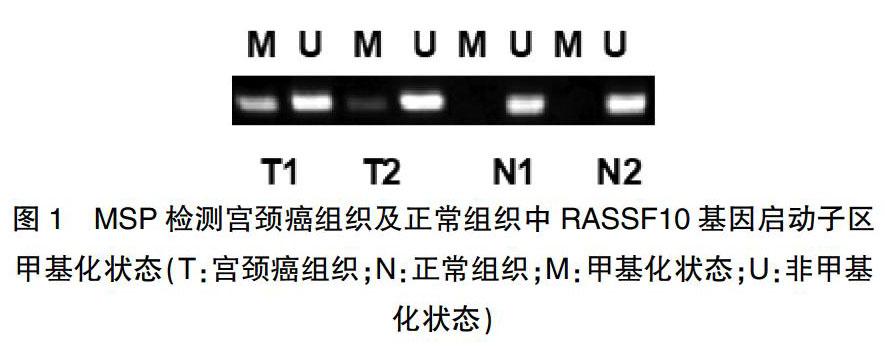
MSP法檢測發現本組宮頸癌組織中RASSF10基因啟動子區甲基化為27例(38.6%),未甲基化為43例(61.4%),而正常宮頸組織未見甲基化,差異具有統計學意義(P<0.05)(圖1)。
2.2 RASSF10基因啟動子區甲基化狀態與臨床因素相關性
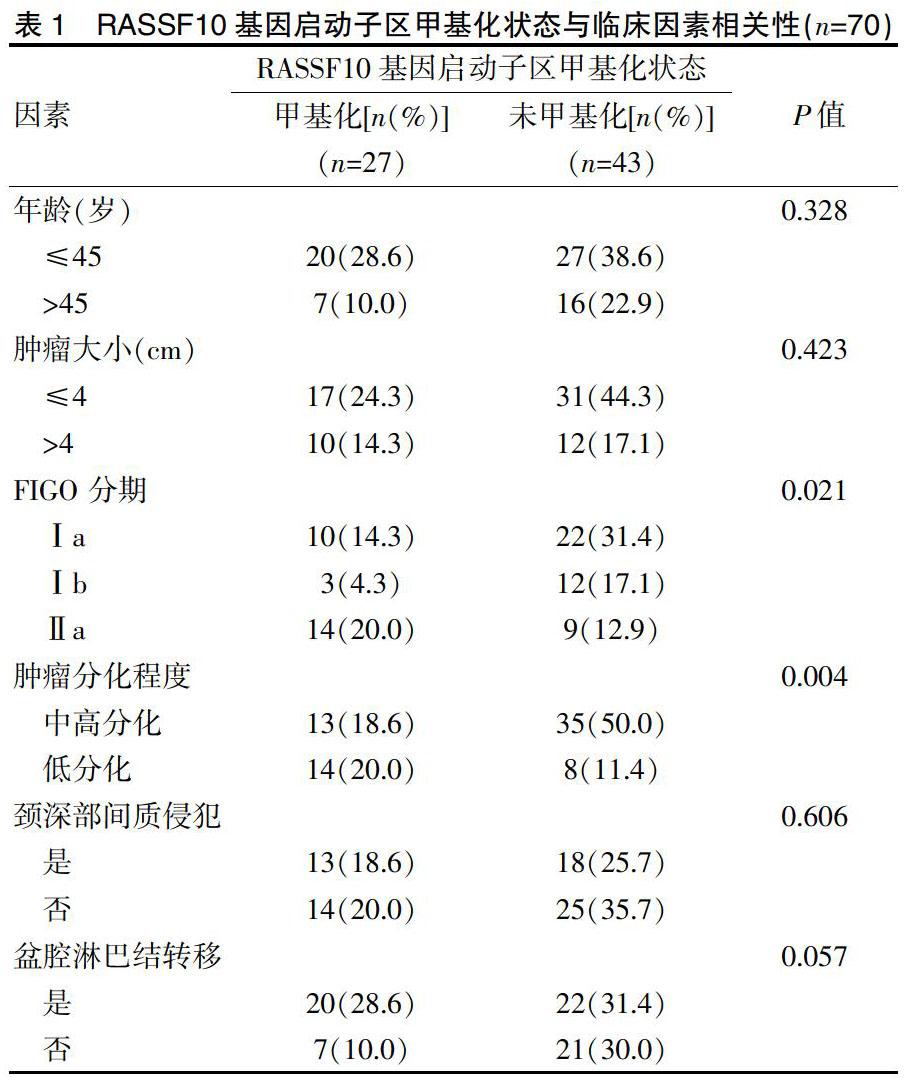
RASSF10基因啟動子區甲基化狀態表達與FIGO分期(P=0.021)和腫瘤分化程度(P=0.004)密切相關,而年齡、腫瘤大小、頸深部間質侵犯及盆腔淋巴結轉移與RASSF10基因啟動子區甲基化狀態無關(P>0.05)(表1)。
2.3 RASSF10基因啟動子區甲基化狀態與宮頸癌預后的關系
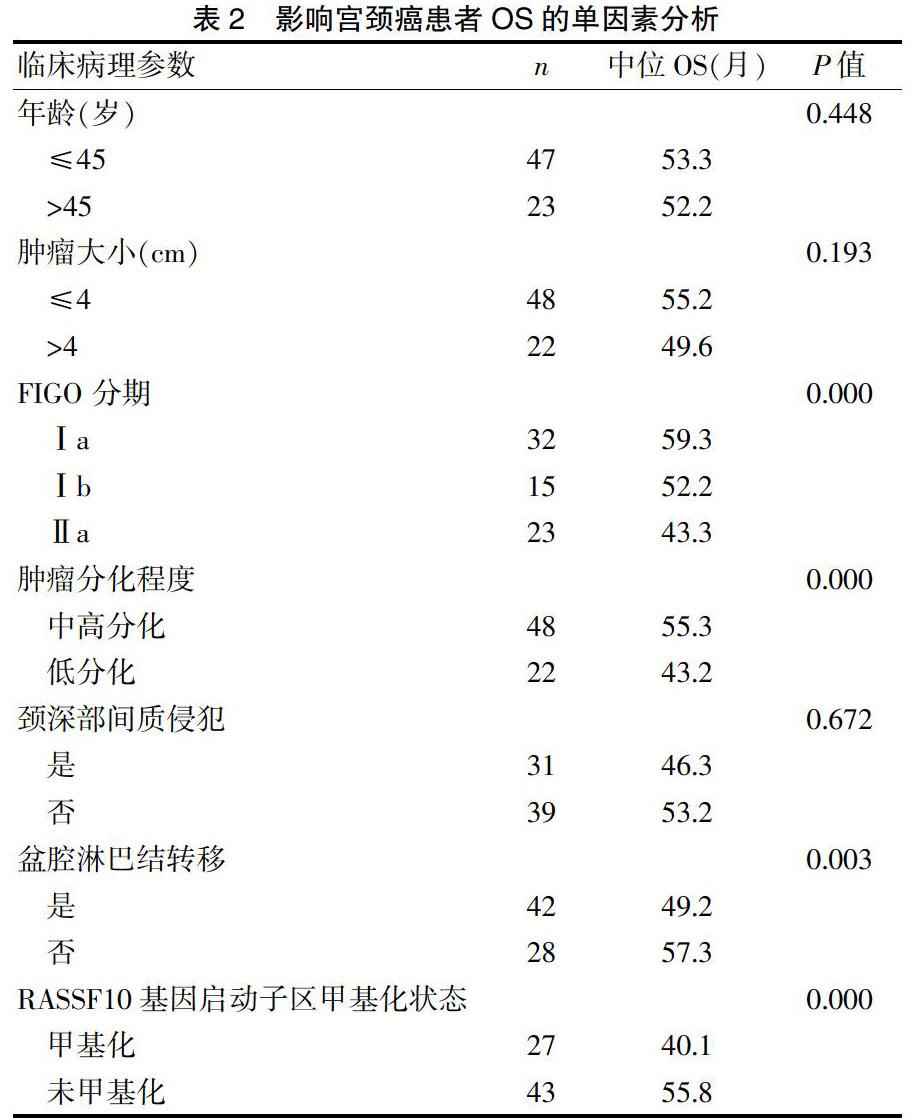
全組獲隨訪時間48~60個月,中位生存期與年齡、腫瘤大小及頸深部間質侵犯無關,但與FIGO分期、腫瘤分化程度、盆腔淋巴結轉移及RASSF10基因啟動子區甲基化有關(表2)。
2.4影響宮頸癌患者OS的多因素分析
將單因素分析中影響OS的4個因素納入多因素分析,結果顯示FIGO 分期、腫瘤分化程度、盆腔淋巴結轉移和RASSF10基因啟動子區甲基化狀態為本組宮頸癌患者的預后獨立因素(表3)。
2.5 生存分析
本組宮頸癌患者中RASSF10基因啟動子區甲基化的5年生存率為66.7%,未甲基化者88.4%,差異具有統計學意義(P<0.05)(表4)。
3討論
Ras相關域家族共包含10個成員[8]。RASSF10基因屬于N-端家族成員之一,編碼N-端RA相關域。該基因為單一外顯子基因,編碼507個氨基酸,定位于染色體11p15.2,位置上靠近RRAS2基因。RASSF10基因啟動子區含有CpG島,RASSF10在癌癥中的低表達與啟動子區CpG島的甲基化相關[9-10]。DNA甲基化通常是DNA的CG兩個核苷酸的胞嘧啶被選擇性地添加甲基,形成5-甲基胞嘧啶,這常見于基因的5'-CG-3'序列,DNA甲基化主要形成5-甲基胞嘧啶(5-mC)和少量的N6-甲基嘌呤(N6-mA)及7-甲基鳥嘌呤(7-mG)[11]。RASSF10基因在多種腫瘤中發生甲基化導致表達降低。Lu等[12]在食管癌細胞系中檢測RASSF10基因mRNA表達水平的缺失或降低,并發現啟動子甲基化的發生,用去甲基化藥物5-aza-dC處理后,其表達得以恢復或提高。此研究證明RASSF10基因CpG島的甲基化可導致該基因在腫瘤中的沉默。在甲狀腺癌中有學者研究發現RASSF10基因在原發性甲狀腺癌中甲基化率為高于濾泡狀腺瘤中甲基化率,而正常甲狀腺組織中均未發現甲基化,說明RASS F10基因甲基化可能與腫瘤發生密切相關[13]。RASSF10基因甲基化狀態可為預后預測指標,Jingyu Deng等[14]在胃癌中發現RASSF10基因啟動子區甲基化患者比RASSF10啟動子未甲基化患者的中位生存期明顯短。并且RASSF10啟動子甲基狀態是胃癌患者預后的獨立預測因子。本研究回顧分析本院收治的宮頸癌患者,探討RASSF10基因啟動子區甲基化狀態在宮頸癌中的臨床價值。
本研究中首先檢測RASSF10基因甲基化狀態。目前檢測DNA甲基化常見的方法主要有酶切法、直接測序法、MSP等,MSP與其他方法相比避免使用限制性內切酶,敏感性高,簡便易行,適用于大樣本檢測,為檢測DNA甲基化較為可信的方法[15]。本研究采用MSP法檢測RASSF10基因啟動子區甲基化狀態。結果顯示,27例患者出現RASSF10基因啟動子區甲基化,而43例患者并未出現RASSF10基因啟動子區甲基化,而正常宮頸組織中未發現RASSF10啟動子區甲基化,這些結果表明RASSF10基因在宮頸癌中低表達與啟動子區甲基化密切相關。進一步探討RASSF10基因啟動子區甲基化狀態與臨床因素之間的相關性發現FIGO分期和腫瘤分化程度等為RASSF10基因啟動子區甲基化狀態密切相關,深入發現Ⅱa期宮頸癌與低分化癌患者RASSF10基因啟動子區甲基化較多,此結果可能暗示RASSF10基因甲基化后表達降低,進而影響下游分子通路導致腫瘤進展。為評價RASSF10基因啟動子區甲基化狀態在宮頸腺癌中的預后價值,本研究采用預后生存分析,結果顯示RASSF10基因啟動子區甲基化狀態為本組患者獨立預后因素,RASSF10基因啟動子區甲基化患者預后比RASSF10基因啟動子區未甲基化患者差。此研究表明RASSF10基因啟動子區甲基化狀態可為宮頸腺癌患者預后預測因子。
綜上所述,宮頸癌中RASSF10基因低表達與啟動子區甲基化相關,RASSF10基因啟動子甲基化狀態與宮頸腺癌患者預后密切相關,可作為宮頸癌預后預測指標。
[參考文獻]
[1] 任康,申良方,周琴,等.局部晚期宮頸癌預后因素的研究進展[J].中國現代醫學雜志,2019,29(2):38-43.
[2] 何瀟.參芪扶正抗癌湯聯合放化療治療宮頸癌的療效觀察及對生存質量的影響[J].中國中醫藥科技,2019, 26(1):80-82.
[3] Feng Y,Zhang Z,Lou T,et al.The safety of fertility preservation for microinvasive cervical adenocarcinoma:A meta-analysis and trial sequential analysis[J].Arch Gynecol Obstet,2018.
[4] Rabelo-Santos SH,Termini L,Boccardo E,et al.Strong SOD2 expression and HPV-16/18 positivity are independent events in cervical cancer[J].Oncotarget,2018,9(31):21630-21640.
[5] Jin Y,Cao B,Zhang M,et al.RASSF10 suppresses hepatocellular carcinoma growth by activating P53 signaling and methylation of RASSF10 is a docetaxel resistant marker[J].Genes Cancer,2015,6(5):231-240.
[6] Ma J,Zhang S,Hu Y,et al. Decreased expression of RASSF10 correlates with poor prognosis in patients with colorectal[J]. Cancer Medicine,2017,96(42):7011.
[7] Wang F,Li P,Feng Y,et al.Low expression of RASSF10 is associated with poor survival in patients with colorectal cancer[J].Hum Pathol,2017,6(2):108-114.
[8] Richter AM,Walesch SK,Dammann RH.Aberrant promoter methylation of the tumour suppressor RASSF10 and its growth inhibitory function in breast cancer[J].Cancers (Basel),2016,8(3):221-230.
[9] 崔建利,郭煒,郭艷麗,等. RASSF10基因在賁門腺癌組織中的甲基化狀態及表達[J].中國癌癥雜志,2014, 24(8):568-574.
[10] Dong T,Zhang Y. Methylation of RASSF10 promotes cell proliferation and serves as a docetaxel resistant marker in human breast cancer[J].Discover Med,2015,20(111):261-271.
[11] Li X,Liang Q,Liu W,et al.Ras association domain family member 10 suppresses gastric cancer growth by cooperating with GSTP1 to regulate JNK/c-Jun/AP-1 pathway[J].Oncogene,2016,35(19):2453-2464.
[12] Lu D,Ma J,Zhan Q,et al.Epigenetic silencing of RASSF10 promotes tumor growth in esophageal squamous cell carcinoma[J].Discov Med,2014,17(94):169-178.
[13] Schagdarsurengin U,Richter AM,W?觟hler C,et al.Frequent epigenetic inactivation of RASSF10 in thyroid cancer[J].Epigenetics,2009,4(8):571-576.
[14] Jingyu Deng,Han Liang,Guoguang Ying,et al.Methylation of ras association domain protein 10 (RASSF10) promoter negative association with the survival of gastric cancer[J].Am J Cancer Res,2014,4(6):916-923.
[15] Richter AM,Zimmermann T,Haag T,et al.Promoter methylation status of Ras-association domain family members in pheochromocytoma[J].Front Endocrinol(Lausanne),2015,6(1):21-24.