不同吸痰深度密閉式吸痰法在外科ICU機械通氣患者中的應用效果比較
2017-05-11 07:02:05梁娟胡雪慧
中國醫藥導報 2017年7期
梁娟+胡雪慧
[摘要] 目的 探討不同吸痰深度密閉式吸痰法在外科ICU機械通氣患者中的應用效果。 方法 選擇2015年5月~2016年12月于第四軍醫大學西京醫院外科綜合ICU接受機械通氣治療的患者150例,采取隨機數字表法分為三組,每組50例。A組吸痰管插入深度等于氣管插管長度;B組吸痰管插入氣道遇阻力后上提1~2 cm;C組吸痰管插入深度達氣管插管長度后再插入1 cm,比較三組患者24 h吸痰次數、血氧飽和度恢復時間、痰鳴音改善評分及并發癥發生情況。 結果 三組患者24 h吸痰次數、血氧飽和度恢復時間、痰鳴音改善評分比較,差異有統計學意義(P < 0.05)。三組患者心率變化、嗆咳及痰中帶血發生率比較,差異有統計學意義(P < 0.05)。 結論 吸痰管置入深度達氣管插管刻度后繼續深入1 cm可有效清除接受機械通氣治療患者的氣道分泌物,對氣道黏膜損傷小,安全性高。
[關鍵詞] 機械通氣患者;密閉式吸痰護理;吸痰深度;吸痰并發癥
[中圖分類號] R473.5 [文獻標識碼] A [文章編號] 1673-7210(2017)03(a)-0159-04
Application effect comparison of different sputum suction methods in ICU patients with mechanical ventilation
LIANG Juan1 HU Xuehui2
1.Department of Pediatrics, Xijing Hospital of the Fourth Military Medical University, Shaanxi Province, Xi′an 710032, China; 2.Department of Nursing, Xijing Hospital of the Fourth Military Medical University, Shaanxi Province, Xi′an 710032, China
[Abstract] Objective To investigate application effect of different sputum suction methods in ICU patients with mechanical ventilation. Methods 150 patients with mechanical ventilation in Surgical Intensive Care Unit of Xijing Hospital of the Fourth Military Medical University from May 2015 to December 2016 were selected. All patients were divided into three groups by using random number table method. Each group of 50 cases. The depth of sputum suction tube was equal to the length of tracheal intubation in group A, the sputum suction tube was inserted into the airway for 1 to 2 cm in group B, the depth of the sputum suction tube was inserted to 1 cm after tracheal intubation in group C. The number of 24 h sputum suction, the recovery time of blood oxygen saturation, the improvement score of sputum sound and incidence of complication among three groups were compared. Results The number of 24 h sputum suction, the recovery time of blood oxygen saturation, the improvement score of sputum sound among three groups were compared, with statistical differences (P < 0.05). Incidence rate of heart rate change, cough and sputum with blood among three groups were compared, with statistical differences (P < 0.05). Conclusion The depth of suction tube is extended to 1 cm after intubation can effective removal of airway secretion in patients receiving mechanical ventilation, has small airway mucosal damage and high safety.
[Key words] Patients with mechanical ventilation; Closed tracheal suction; Depth of sputum suction; Complication caused by sputum suction
1979年機械通氣技術首先應用于患者至今已40年,隨著機械通氣技術的跨越發展,這一技術對護理人員的職業要求越來越高[1]。氣管內吸痰(ETS)是對已經建立機械通氣患者最常見的護理方法之一,ETS包含支氣管治療和防止機械通氣引起的肺部阻塞[2]。美國呼吸護理學會(AARC)發表的氣管內吸痰指南中對吸痰操作規范與實際臨床護理應用存在較大差異,且具體吸痰深度界定模糊[3-4]。如何能夠根據患者情況明確吸痰管深度范圍,保證氣道通暢的同時最大程度減少吸痰帶來的一系列不良反應,最終提高機械通氣患者臨床護理質量十分重要[5-6]。本研究調查對象為外科ICU機械通氣患者,采用三種臨床常用密閉式吸痰方法,比較不同吸痰深度的吸痰效果及并發癥發生情況,明確最佳吸痰方法及深度范圍,在保證安全性的前提下提高機械通氣患者護理質量。
1 資料與方法
1.1 一般資料
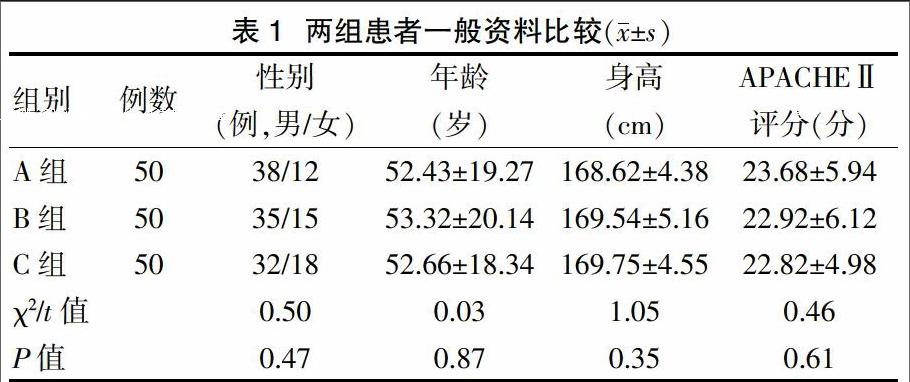
選取西京醫院外科綜合ICU 2015年5月~2016年12月需接受機械通氣治療患者150例為研究對象,采取密閉式吸痰護理方法,其中男114例,女36例;平均年齡(52.1±1.5)歲;基本情況為呼吸窘迫綜合征66例,窒息48例,昏迷36例。所有患者按照隨機數字表法分為A、B、C組,各50例。三組患者性別、年齡、身高、急性生理學及慢性健康狀況(APACHEⅡ)評分比較,差異無統計學意義 (P > 0.05),具有可比性。見表1。本研究經西京醫院倫理委員會討論通過,所有入選患者均簽署知情同意書。
1.2 方法
所有患者采用密閉式吸痰護理[7]。吸痰操作由經過培訓的ICU護理人員進行。吸痰前先評估患者氣道的一般情況[8]。臨床選擇常用規格為12~14號吸痰管。吸痰負壓為200~300 mmHg[9]。具體操作方法為護理人員一手握住可旋轉接頭,另一手拇指及食指將吸痰管緩慢插入患者氣管套管內達到所需深度后,按下負壓閥進行吸痰[10],吸痰時間不超過15 s[11]。如患者氣道內分泌物較黏稠,可經沖水孔注入2~3 mL的無菌生理鹽水,再實施上述吸痰操作[12]。三組患者選擇不同的吸痰深度:A組吸痰管插入深度與氣管插管刻度保持一致;B組吸痰管插入氣管插管深部,遇阻力后上提1~2 cm;C組吸痰管置入深度達氣管插管刻度后繼續深入1 cm。吸痰前后分別提高呼吸機氧濃度10%,時間持續1~2 min,提升患者的血氧飽和度(SpO2)[13]。
1.3 觀察指標
①吸痰效果:24 h吸痰次數、SpO2恢復時間以及痰鳴音改善評分。其中痰鳴音改善情況以評分方式計算[14]:完全消失為3分;明顯減輕為2分;依然存在為1分。②并發癥情況:心率變化、嗆咳以及痰中帶血。吸痰前監測基礎心率,吸痰時如心率加快超過基礎心率的20%,停止吸痰后5 min降至基礎心率,則為心率變化。
1.4 統計學方法
采用SPSS 19.0統計軟件對數據進行分析和處理,計量資料以均數±標準差(x±s)表示,采用單因素方差分析,計數資料采用χ2檢驗,以P < 0.05為差異有統計學意義。
2 結果
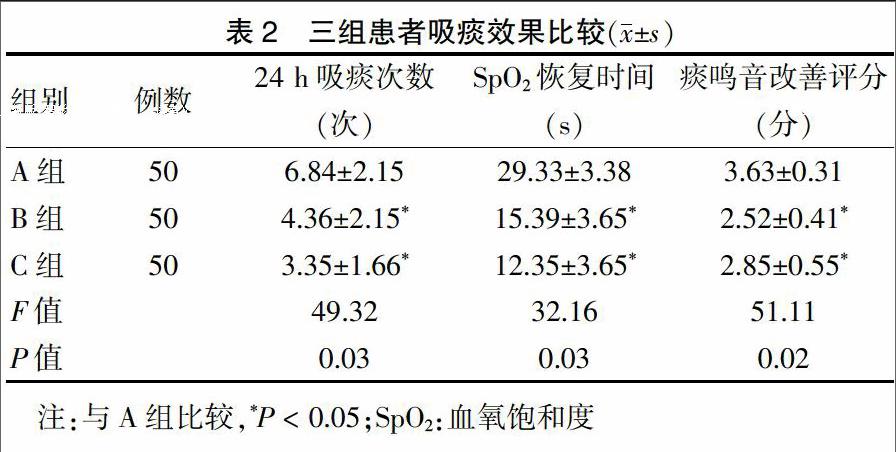
2.1 三組患者吸痰效果比較
三組患者24 h吸痰次數、SpO2恢復時間、痰鳴音改善評分比較,差異有統計學意義(P < 0.05)。見表2。
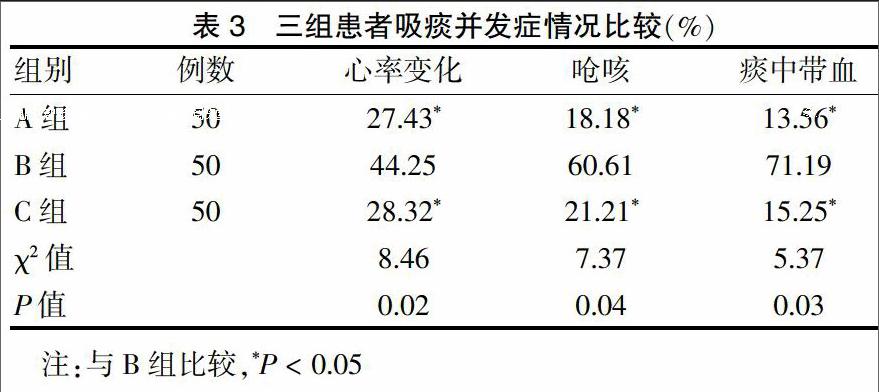
2.2 三組患者吸痰并發癥情況比較
三組患者心率變化、嗆咳及痰中帶血發生率比較,差異有統計學意義(P < 0.05)。見表3。
3 討論
隨著機械通氣技術的跨越式發展,針對外傷患者術后呼吸治療已成為急危重癥患者重要的治療手段[15]。外科ICU患者在呼吸治療過程中,氣道內環境變化較大,分泌物增多,術后傷口疼痛、感染、意識障礙長期臥床等情況的出現易導致咳嗽排痰困難,出現痰液滯留、痰痂堵管等現象,所有這些現象在外科ICU護理工作中十分常見[16]。
2010年AARC發表的氣管內吸痰指南中對吸痰的操作指導與臨床護理操作存在較大不同[17],AARC指南推薦兩種吸痰方法,一種為吸痰管刻度與氣管插管保持一致,另一種為吸痰管在遇阻力后上提1~2 cm[18]。這兩種吸痰方法在臨床工作中十分常見,但該指南并沒有對患者一般情況進行限定,如外科機械通氣患者的吸痰操作是否與內科患者類似[19]。在外科ICU實際工作中,我們發現當吸痰管和氣管導管刻度一致后在深入1 cm可以保證吸痰有效性,同時減少吸痰并發癥的發生,在回顧外文文獻時發現報道多集中于吸痰時機的判斷,而對于吸痰管深度及相關并發癥的報道相對較少[20]。
臨床護理實踐中如果外科機械通氣患者采取指南推薦的第二種方式進行吸痰[21]。患者嗆咳發生率較高,劇烈且持續時間較長,嗆咳導致短時間內氣道壓力急劇上升,特別是在機械通氣患者使用密閉通氣管道,過高的氣道壓損傷氣道黏膜導致血性分泌物增多,最常見的表現為痰中帶血的發生,在吸痰過程中損傷氣道黏膜更加不利于患者呼吸功能的恢復[22-23]。如果使用指南推薦的第一種方法,患者吸痰并發癥發生率明顯降低,但24 h吸痰次數顯著增多和SpO2恢復時間顯著延長,增加了單位時間對患者氣道的侵擾次數及吸痰過程中的缺氧風險。最終使用吸痰管置入深度達氣管插管刻度后繼續深入1 cm的吸痰方法,不但可以減少不良反應的發生,同時24 h吸痰次數、SpO2恢復時間及痰鳴音改善評分得到顯著改善。
綜上所述,吸痰管置入深度達氣管插管刻度后繼續深入1 cm的吸痰方法能夠在有效清除患者呼吸道分泌物的同時,減少對患者氣道的刺激及損傷,減少侵擾次數,同時對患者心率、氣道黏膜影響較小,具有較好的有效性以及安全性。然而本實驗沒有將內科ICU患者納入比較,同時樣本量規模較小,如果能夠在多家醫療機構展開多中心研究及增加樣本量會使本研究更加完善。
[參考文獻]
[1] Tobin MJ. Mechanical ventilation [J]. N Engl J Med,1994, 330(15):1056-1061.
[2] Stone KS,Turner B. Endotracheal suctioning [J]. Annu Rev Nurs Res,1989,7:27-49.
[3] Care AA. AARC clinical practice guidelines. Endotracheal suctioning of mechanically ventilated patients with artificial airways 2010 [J]. Respir Care,2010,55(6):758-764.
[4] 陳清秀,蔡榕.機械通氣患兒氣管內開放式與密閉式吸痰的效果觀察[J].實用醫學雜志,2012,28(10):1736-1738.
[5] 譚海云,祝妍華,劉喜梅.密閉式吸痰方法對機械通氣患者的效果分析[J].當代醫學,2010,16(19):34-35.
[6] 相生躍,班努·庫肯.機械通氣時不同深度密閉式吸痰的效果評價[J].當代醫學,2015,21(22):78-79.
[7] Varghese S,Moly KT. Exploratory study on the knowledge and skill of critical care nurses on endotracheal suctioning [J]. Nat Accred Board Hosp Healthcare Providers,2016,3:13-19.
[8] Bülbül MG,Koca?觭al GE,E?鬤er ■,et al. Knowledge and practice of intensive care nurses for endotracheal suctioning in a teaching hospital in western Turkey [J]. Intensive Crit Care Nurs,2017,39:45-54.
[9] Dastdadeh R,Ebadi A,Vahedian-Azimi A. Comparison of the effect of open and closed endotracheal suctioning methods on pain and agitation in medical ICU patients:a clinical trial [J]. Anesth Pain Med,2016,6(5):e38337.
[10] Heybeli C. Tracheal suctioning in ventilatory-associated pneumoniae:is saline the best choice? [J]. Med Hypotheses,2016,92:74.
[11] Ackerman M,Gugerty B. The effect of normal saline bolus instillationin artificial airways [J]. J ORL Head Neck Nurs,1996,14(1):17-21.
[12] Sadowitz B,Jain S,Kollisch-Singule M,et al. Preemptive mechanical ventilation can block progressive acute lung injury [J]. World J Crit Care Med,2016,5(1):74-82.
[13] Yoshida T,Roldan R,Beraldo MA,et al. Spontaneous effort during mechanical ventilation:maximal injury with less positive end-expiratory pressure [J]. Crit Care Med,2016,44(8):e678-e688.
[14] Silva PL,Pelosi P,Rocco PR. Optimal mechanical ventilation strategies to minimize ventilator-induced lung injury in non-injured and injured lungs [J]. Expert Rev Respir Med,2016,10(12):1243-1245.
[15] Restrepo RD,Hirst KR,Wittnebel L,et al. AARC clinical practice guideline:transcutaneous monitoring of carbon dioxide and oxygen:2012 [J]. Respir Care,2012,57(11):1955-1962.
[16] Saddy F,Sutherasan Y,Rocco PR,et al. Ventilator-associated lung injury during assisted mechanical ventilation [J]. Semin Respir Crit Care Med,2014,35(4):409-417.
[17] Cataldi M,Sblendorio V,Leo A,et al. Biofilm-dependent airway infections:a role for ambroxol? [J]. Pulm Pharmacol Ther,2014,28(2):98-108.
[18] American Association for Respiratory Care. Endotracheal Suctioning of Mechanically Ventilated Patients With Artificial Airways 2010. [J]. Respir Care,2010,55(6):758-764.
[19] Sole ML,Bennett M,Ashworth S. Clinical indicators for endotracheal suctioning in adult patients receiving mechanical ventilation [J]. Am J Crit Care,2015,24(4):318-324.
[20] Jansson M,Alakokko T,Ylipalosaari P,et al. Critical care nurses' knowledge of,adherence to and barriers towards evidence-based guidelines for the prevention of ventilator-associated pneumonia—a survey study [J]. Intensive Crit Care Nurs,2013,29(4):216-227.
[21] Caruso P,Denari S,Ruiz SAL,et al. Saline instillation before tracheal suctioning decreases the incidence of ventilator-associated pneumonia [J]. J Crit Care,2009, 37(1):32-38.
[22] Stéphan F,Barrucand B,Petit P,et al. High-flow nasal oxygen vs noninvasive positive airway pressure in hypoxemic patients after cardiothoracic surgery:a randomized clinical trial [J]. J Evid Based Dent Prac,2015,313(23):2331-2339.
[23] Sztrymf B,Messika J,Bertrand F,et al. Beneficial effects of humidified high flow nasal oxygen in critical care patients:a prospective pilot study [J]. Intensive Care Med,2011,37(11):1780-1786.