PCI術后血清細胞因子改變對冠心病患者預后的預測價值*
2016-12-27 00:55:38盛曉東周建龍
貴州醫科大學學報 2016年11期
金 靜, 盛曉東, 周建龍, 范 韜
(常熟市第二人民醫院 心血管內科, 江蘇 常熟 215500)
?
PCI術后血清細胞因子改變對冠心病患者預后的預測價值*
金 靜, 盛曉東, 周建龍, 范 韜
(常熟市第二人民醫院 心血管內科, 江蘇 常熟 215500)
目的: 分析冠心病(CAD)介入治療(PCI)術后血清細胞因子與術后心臟不良事件(MACE) 及預后的相關性。方法:觀察78例CAD患者PCI手術治療效果,比較PCI手術前及術后24 h患者血清C-反應蛋白(CRP)、腫瘤壞死因子-α(TNF-α)、白介素(IL)-6、轉化生長因子-β(TGF-β)及 IL-10水平,采用pearson分析與術前比較有差異的細胞因子間的相關性,用受試者工作曲線(ROC)分析術后具有相關性細胞因子對PCI預后的診斷價值;以PCI預后的診斷價值高的細胞因子水平中位數進行分組,比較該細胞因子與PCI術后12周累積MACE發生率的關系。結果:78例CAD患者均成功進行PCI手術,術后12周內有18例并發MACE,未出現術后死亡病例;與術前比較,術后CAD患者CRP及TNF-α水平較治療前顯著升高(P<0.05);術后CAD患者血清TNF-α與CRP呈現顯著正相關(r=0.813,P<0.001); ROC曲線分析顯示, CRP以 18.73 mg/L為截點值,CRP預測PCI術后并發MACE的敏感性、特異性及曲線下面積均優于20.35 ng/L的 TNF-α;高水平CRP患者術后12周累積MACE發生率顯著高于低水平患者(P=0.038)。結論:CAD患者PCI術后血清CRP水平檢測對患者預后的診斷均有一定價值。
冠狀動脈疾病; 經皮冠狀動脈介入; 炎癥; 預后; 治療結果; 心臟不良事件
冠狀動脈粥樣硬化性心臟病(coronary atherosclerotic heart disease,CAD)與遺傳易感、環境污染及代謝紊亂等因素相關,CAD具有較高的致殘及致死性,經皮冠狀動脈介入(percutaneous coronary intervention,PCI)是治療CAD的主要方式,雖然效果較佳,但仍有部分患者術后并發心臟不良事件(major adverse cardiac events,MACE)[1-2]。CAD的基本病理改變主要為冠狀動脈粥樣硬化,但慢性炎癥在動脈粥樣硬化過程中也發揮了關鍵的作用[3]。本研究通過分析PCI術后的CAD患者外周血血清C-反應蛋白(C-reactive protein,CRP)、腫瘤壞死因子-α(tumor necrosis factor-α,TNF-α)、白介素-6(interleukin-6,IL-6)、轉化生長因子-β(transforming growth factor-β, TGF-β)及白介素-10interleukin-10,IL-10)水平等外周血細胞因子水平變化,探索其用于判斷PCI預后的可行性。
1 資料與方法
1.1 臨床資料
2012年1月~2016年1月采用股動脈或橈動脈路徑常規方法行PCI術治療的CAD患者78例,所有患者均符合世界衛生組織(WHO)冠心病的診斷標準[4],并經冠狀動脈造影明確診斷為CAD。男性45例,女性33例;年齡65~80歲,平均(70.8±5.8歲),平均病程(9.1±2.6)年;心絞痛48例、心肌梗死27例、缺血性心力衰竭3例。排除合并其它心血管器質性病變、外周血管疾病、糖尿病等嚴重代謝性疾病、自身免疫性疾病及既往有心臟手術史或臨床資料缺失者。
1.2 觀察指標
細胞因子:于PCI術前及術后24 h抽取靜脈血5 mL,采用酶聯免疫吸附法(ELISA)檢測患者血清CRP、TNF-α、IL-6、TGF-β及IL-10水平,分析與術前比較有差異的術后各細胞因子間的相關性;分析有相關性細胞因子對PCI預后的診斷價值;以PCI預后的診斷價值高的細胞因子中位數進行分組,觀察PCI術后12周累積MACE發生率。PCI治療效果的判斷參照文獻[5-6]。術后病變血管:殘余狹窄<20 %、心肌梗死溶栓試驗(TIMI)血流3級、無圍術期嚴重并發癥(死亡、急性心肌梗死、急性冠狀動脈旁路移植術),定義為治療有效;患者發生心絞痛、心源性休克、心肌梗死及心力衰竭,定義為MACE。
1.3 統計學方法
2 結果
2.1 手術效果
本研究納入的78例CAD患者均成功進行PCI手術,術后12周內有18例患者并發MACE,其中心絞痛12例、心源性休克1例、心肌梗死3例及心力衰竭2例。未出現術后死亡病例。
2.2 血清CRP、TNF-α、IL-6、TGF-β及IL-10
如表1所示,與術前比較,PCI手術治療后CAD患者CRP及TNF-α水平較治療前顯著升高,差異有統計學意義(P<0.05);IL-6、TGF-β及IL-10水平變化差異無統計學意義(P>0.05)。
2.3 PCI術后CRP與TNF-α的相關性
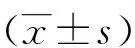
如圖1所示,PCI術后患者外周血TNF-α與CRP呈現顯著正相關(r=0.813,P<0.001)。2.4 PCI術后CRP、TNF-α水平對PCI預后的診斷價值
如圖2,ROC曲線分析顯示, CRP以 18.73 mg/L為截點值,CRP預測PCI術后并發MACE的敏感性(94.44%)、特異性(95.00%)及曲線下面積(0.93)均優于TNF-α(83.33%、81.67%、0.87)。
表1 PCI手術前后患者血清CRP、TNF-α、IL-6、TGF-β及IL-10水平
Tab.1 Serum levels of CRP, TNF-α, IL-6, TGF-β and IL-10 before and after PCI surgery

細胞因子治療前治療后24htPTNF-α(ng/L)13.1±3.618.5±5.17.640<0.001TGF-β(ng/L)216.9±35.7223.8±38.21.1660.246CRP(mg/L)3.9±1.515.6±4.223.170<0.001IL-10(ng/L)11.3±3.711.8±3.90.8210.413IL-6(ng/L)10.6±2.111.3±3.21.6150.108
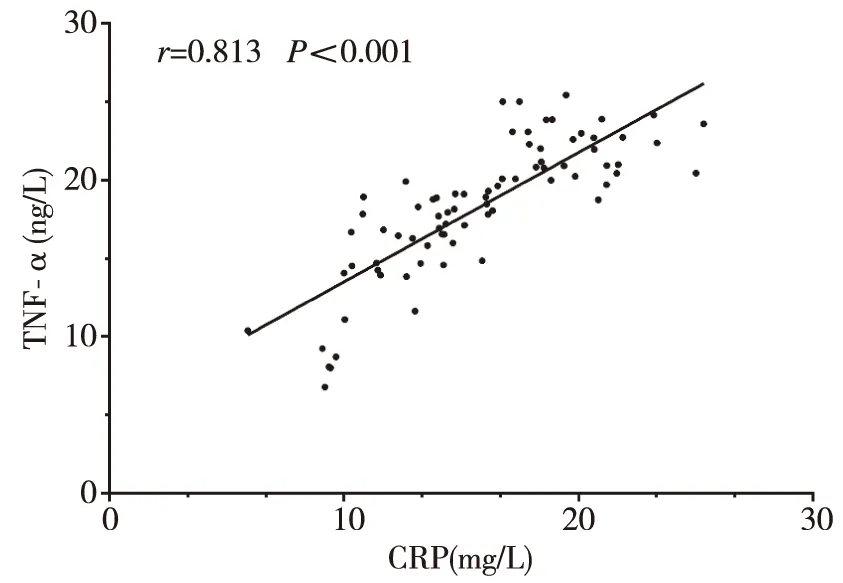
圖1 PCI術后外周血TNF與CRP的相關性分析
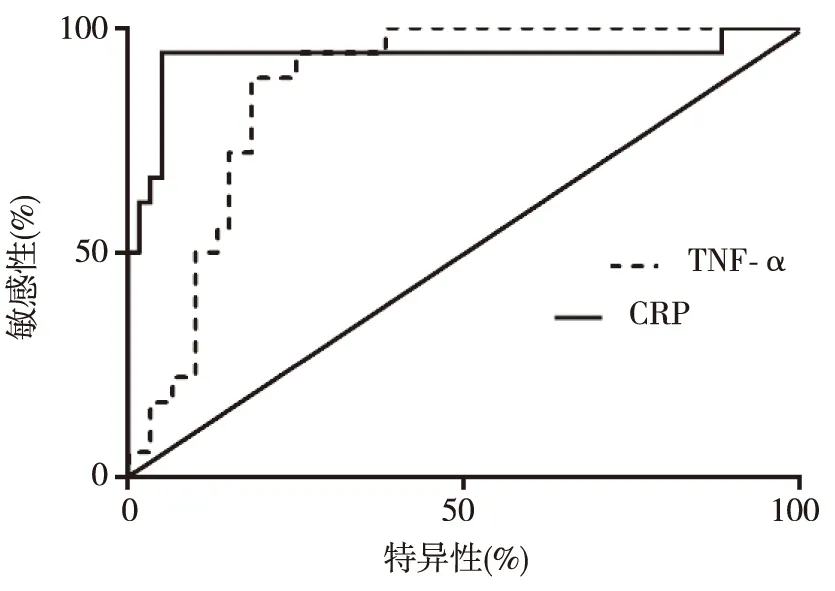
圖2 外周血CRP、TNF-α水平對PCI
2.5 PCI術后不同水平CRP患者的預后比較
如圖3所示,以PCI術后CRP水平中位數為界將患者分為高水平組(n=39,>15.1 mg/L)及低水平組(n=39,≤15.1 mg/L),K-M生存分析顯示,高水平患者PCI術后12周累積MACE發生率12.82%(5/39)顯著高于低水平患者33.33%(13/39),差異有統計學意義(Log-rankχ2=4.303,P=0.038)。
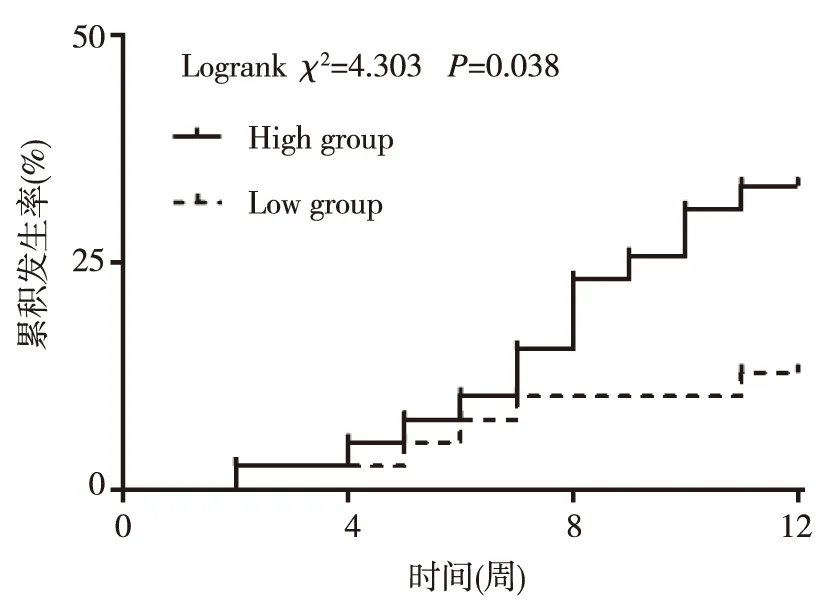
圖3 PCI術后不同CRP水平患者的預后比較
3 討論
CAD主要累及老年人群,是一種嚴重威脅人類生命健康的心血管疾病。隨著我國人口老齡化加速發展、西方化的生活飲食方式及環境污染等諸多因素的共同影響,我國CAD的發病率呈現逐年增多的趨勢[7-8]。雖然PCI對CAD的治療效果已得到認可,但因其屬于有創治療,PCI手術會刺激患者局部血管從而引發全身性炎癥反應[9-10]。有研究報道血管壁內炎癥不僅是動脈粥樣硬化發生發展的關鍵因素之一,也是導致血管收縮或損傷的主要原因[11]。因次,PCI術后引發的炎癥反應可能是患者術后發生MACE的可能機制之一,而MACE是導致患者手術失敗甚至是死亡的主要術后并發癥[12-13]。本研究嘗試從對比分析患者PCI手術前后外周血細胞因子的改變著手,以期發現可用于臨床判斷PCI預后的實驗室指標。
CRP可在感染、應激等情況下升高,但升高水平會有差異[14]。TNF-α是經典的促炎因子,在冠狀動脈粥樣硬化過程中發揮關鍵作用,是破壞血管內皮細胞的主要細胞因子,在感染及應激情況下表達也可增加[15]。本研究發現,接受PCI治療的CAD患者術后TNF-α及CRP水平均呈現顯著升高。提示PCI手術可導致患者出現系統性炎癥反應;進一步分析發現PCI術后患者外周血CRP與TNF-α呈現顯著正相關,而CRP是臨床常用指標,檢測方便、價格低廉,提示CRP檢測對TNF-α檢測具有一定的可替代性。為了分析患者外周血細胞因子對患者預后的預測價值,本文采用ROC曲線分析了TNF-α及CRP對PCI術后12周是否發生MACE的預測診斷價值。結果顯示,CRP的預測診斷敏感性及特異性均超過90%,優于TNF-α。在此基礎上,本研究以患者術后CRP中位數進行分組比較,結果發現術后高水平CRP患者術后12周累積MACE發生率顯著高于術后低水平的CRP患者,提示CRP對PCI手術的預后有一定預測價值,且CRP在臨床使用廣泛,說明該結果具有一定臨床實用價值。但由于本次研究樣本量有限,所得結果尚需進一步研究證實。綜上, CAD患者PCI術后血清CRP水平檢測對患者預后的診斷均有一定價值。
[1] Manocha A, Srivastava LM. Lipoprotein (a): a unique independent risk factor for coronary artery disease[J]. Indian J Clin Biochem, 2016 (1):13-20.
[2] Piek JJ, van Lavieren MA. Accelerate and decelerate in primary percutaneous coronary intervention[J]. JACC Cardiovasc Interv, 2016 (3):241-243.
[3] Bezgin CH, Bezgin T, Kesebir S. Temperament and character profiles and psychiatric comorbidities in patients with coronary artery or valvular heart disease: relationship with cardiac disease severity[J]. J Clin Med Res, 2016 (3):202-209.
[4] 任瑋, 申延偉, 左麗. 冠心病患者治療前后血漿白細胞介素-6水平的變化[J]. 貴陽醫學院學報, 2004 (1):28-30.
[5] 張科, 譚紅霞, 盧建剛. 老年冠心病患者PCI后hs-CRP和腦鈉肽水平改變[J]. 貴陽醫學院學報, 2014 (1):67-69.
[6] 周曉瑞, 盧家凱, 陳峣, 等. 妊娠合并心臟病患者心臟不良事件危險因素分析[J]. 中華內科雜志, 2013 (11):966-969.
[7] 王波, 王臨池, 趙翼洪, 等. 2009-2013年蘇州20歲及以上居民冠心病發病率變化趨勢及類型分析[J]. 中國全科醫學, 2015 (24):2952-2956.
[8] 王斌,韓雅玲,荊全民,等.冠狀動脈前降支近段臨界靶病變的血管內超聲影像學特點研究.中國實用內科雜志, 2014(10): 1004-1007.
[9] Won H, Her AY, Kim BK, et al. Percutaneous coronary intervention is more beneficial than optimal medical therapy in elderly patients with angina pectoris[J]. Yonsei Med J, 2016 (2):382-387.
[10]Safranow K, Dziedziejko V, Rzeuski R, et al. Inflammation markers are associated with metabolic syndrome and ventricular arrhythmia in patients with coronary artery disease[J]. Postepy Hig Med Dosw (Online), 2016(11):56-66.
[11]Grines CL, Harjai KJ, Schreiber TL. Percutaneous coronary intervention: 2015 in review[J]. J Interv Cardiol, 2016 (1):11-26.
[12]Fiedler KA, Ndrepepa G, Schulz S, et al. Impact of bivalirudin on post-procedural epicardial blood flow, risk of stent thrombosis and mortality after percutaneous coronary intervention[J]. EuroIntervention, 2016 (11):1275-1282.
[13]韓雅玲.冠心病阿司匹林抵抗的研究與對策[J].中國實用內科雜志, 2015 (1): 3-7.
[14]Cutando A, Montero J, Gómez-de DR, et al. Effect of topical application of melatonin on serum levels of C-reactive protein (CRP), interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α) in patients with type 1 or type 2 diabetes and periodontal disease[J]. J Clin Exp Dent, 2015 (5):628-633.
[15]Teplan V, Senolt L, Hulejova H, et al. Early changes in serum visfatin after abdominal surgery: a new pro-inflammatory marker in diagnosis[J]. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub, 2015 (3):489-496.
(2016-08-10收稿,2016-11-04修回)
中文編輯: 吳昌學; 英文編輯: 劉 華
Prognostic Value of Serum Cytokine Changes after PCI in Patients with CAD
JIN Jing, SHENG Xiaodong, ZHOU Jianlong, FAN Tao
(DepartmentofCardiology,ChangshuSecondPeople'sHospital,Changshu215500,Jiangsu,China)
Objective: To analyze the correlation between serum cytokines and postoperative adverse cardiac events (MACE) and prognosis in patients with coronary heart disease (CAD) after PCI interventional therapy. Methods: The curative effect was observed in 78 cases of CAD patients with PCI interventional treatment. The serum level of CRP, TNF-α, IL-6, TGF-β and IL-10 were compared between before PCI surgery and 24 h after PCI surgery. Pearson analysis was used to compare the correlation between different cytokines and MACE, and the receiver operating curve (ROC) was used to analyze the prognostic value of PCI. The median level of cytokine levels with high diagnostic value in the PCI prognosis was grouped, and the relationship between the cytokine and the cumulative incidence of MACE 12 weeks after PCI was compared. Results: PCI surgery was successfully performed in 78 cases of CAD patients, of whom 18 cases were complicated with MACE within 12 weeks, and there were no postoperative deaths. Compared with preoperative, the level of CRP and TNF-α in patients with CAD was significantly increased after PCI surgery (P<0.05). The serum level of TNF-α was significantly positively correlated with and CRP level in postoperative patients with CAD (r=0.813,P<0.001). ROC curve analysis showed that under the condition of CRP 18.73 mg/L as the cut-off point, the sensitivity, specificity and area under the curve of CRP's prediction of MACE after PCI were better than their counterparts of TNF-α with 20.35 ng/L. The cumulative incidence of MACE was significantly higher in patients with high level of CRP 12 weeks after surgery than those patients with low levels of (P=0.038). Conclusion: Detection of serum CRP level after PCI in patients with CAD has a certain value in diagnosis and prognosis.
coronary artery disease; percutaneous coronary intervention; inflammation; prognosis; treatment outcome; major adverse cardiac events
常熟市衛生局課題項目(cs201117)
時間:2016-11-15 網絡出版地址:http://www.cnki.net/kcms/detail/52.1164.R.20161115.1757.011.html
R541.4
A
1000-2707(2016)11-1322-04
10.19367/j.cnki.1000-2707.2016.11.019
猜你喜歡
中老年保健(2021年3期)2021-08-22 06:50:04
天津醫科大學學報(2021年4期)2021-08-21 02:14:32
天津醫科大學學報(2021年2期)2021-03-29 05:31:08
現代臨床醫學(2021年1期)2021-01-26 00:56:02
基層中醫藥(2020年10期)2020-11-27 01:58:58
智慧健康(2019年36期)2020-01-14 15:22:58
文理導航·科普童話(2016年7期)2017-02-04 15:09:20
小天使·四年級語數英綜合(2016年11期)2016-11-29 22:37:30
中國衛生標準管理(2015年3期)2016-01-14 03:41:45
現代檢驗醫學雜志(2014年4期)2014-02-02 02:44:59
