特應性皮炎患者皮膚表面真菌定植分析
2016-11-06 15:21:15張秀欽程波紀明開方芳蘇惠春
中華皮膚科雜志 2016年7期
張秀欽 程波 紀明開 方芳 蘇惠春
361026廈門市海滄醫院皮膚科(張秀欽);福建醫科大學附屬第一醫院皮膚科(程波、紀明開、方芳、蘇惠春)
特應性皮炎患者皮膚表面真菌定植分析
張秀欽 程波 紀明開 方芳 蘇惠春
361026廈門市海滄醫院皮膚科(張秀欽);福建醫科大學附屬第一醫院皮膚科(程波、紀明開、方芳、蘇惠春)
目的觀察念珠菌、紅酵母、青霉、曲霉在特應性皮炎患者皮膚表面定植情況,分析這4種常見致敏真菌與特應性皮炎癥狀嚴重程度的相關性。方法特應性皮炎患者50例,健康對照組20例。刮取特應性皮炎患者皮損部位及非皮損部位的鱗屑(以四肢屈側為主)、健康對照組肘關節屈側皮屑行真菌鏡檢,無1例發現菌絲或假菌絲;將皮屑標本接種于沙氏葡萄糖培養基,置25℃恒溫箱內培養,發現真菌及酵母樣可疑菌落,轉種沙氏葡萄糖培養基斜面,獲得純培養后,根據菌落形態特征及顏色、菌落生長的快慢、鏡下孢子及菌絲的特征進行菌種鑒定。結果特應性皮炎組50例,皮損表面檢出念珠菌29例(58%)、紅酵母17例(34%);健康對照組20例,檢出念珠菌5例(25%)、紅酵母2例(10%),特應性皮炎組念珠菌、紅酵母檢出率明顯高于健康對照組(χ2值分別為6.23、4.10,均P< 0.05)。重度患者25例,檢出念珠菌19例(76%)、紅酵母12例(48%);中度患者25例,檢出念珠菌10例(40%)、紅酵母5例(20%),重度患者皮損表面念珠菌、紅酵母檢出率明顯高于中度患者(χ2值分別為6.65、4.37,均P<0.05)。患者組與對照組青霉、曲霉檢出率差異無統計學意義。結論特應性皮炎患者皮膚表面念珠菌、紅酵母定植明顯高于健康對照組,且重度患者定植率高于中度患者,表明真菌定植的種類與皮膚的健康狀況相關,與特應性皮炎患者癥狀的嚴重程度相關。
皮炎,特應性;白色念珠菌;紅酵母屬;產黃青霉;曲霉菌屬
特應性皮炎(AD)是一種遺傳過敏性疾病,除了對食物和吸入物過敏外,其血清對微生物的sIgE抗體升高,包括金黃色葡萄球菌、馬拉色菌、白念珠菌[1]。最近的研究表明,真菌致敏原在遺傳過敏性疾病中也發揮重要作用。我們采用常規真菌培養方法,觀察白念珠菌、紅酵母、青霉、曲霉在AD患者皮損和非皮損部位,以及中度及重度患者皮膚表面的定植情況。
一、對象與方法
1.對象:2012年6-12月,福建醫科大學附屬第一醫院皮膚科門診AD患者50例,均符合Williams提出的AD診斷標準[2],所有受試者2周內均未使用抗真菌藥、糖皮質激素或免疫抑制劑治療,無其他免疫及炎癥性疾病等病史。其中男28例,女22例;年齡2~45歲,平均15歲;病程2個月至18年,平均7年。伴過敏性鼻炎或哮喘20例。AD病情嚴重程度評分(SCORAD)為26~84.5分,平均(57±16)分;中、重度患者各25例。對照組20例,女8例,男12例,年齡2~40歲,平均12歲,均為健康體檢者,無過敏性疾病及家族過敏史,無免疫及炎癥性疾病等病史,兩組在年齡及性別方面差異無統計學意義,具有可比性。SCORAD評分標準為,①皮膚病變范圍:以占1%體表面積為1分;成人頭頸部、臂部各占9%,軀干前后各占13.5%,下肢各占22.5%;<14歲兒童頭頸部、臂部各9%,軀干前后及下肢各18%;②皮損嚴重度:包括6項體征:a紅斑,b丘疹/水腫,c糜爛、滲出(或)結痂,d角化脫屑,e浸潤與苔蘚化,f皮膚干燥(評價未受累皮膚);用3分4級法:0分為無,1分為輕度,2分為中度,3分為重度;③瘙癢及影響睡眠程度:應用視覺模擬評分法(VAS),VAS標尺由0分(無瘙癢)至10分(患者所能想象最嚴重的瘙癢),患者在標尺上標出最能代表其瘙癢強度的點;評價睡眠的方法同瘙癢一樣。SCORAD=①/5+②×7/2+③,總分范圍0~103分。SCORAD評分分級為:輕度<15分;中度15~40分;重度>40分。
2.試驗材料:沙氏葡萄糖培養基根據《全國臨床檢驗操作規程》配制,法國柯瑪嘉顯色培養基(廣州益滿生物科技有限公司)。
3.方法:取患者皮損部位的鱗屑及非皮損部位的皮屑(均以四肢屈側為主),健康對照組刮取肘關節屈側的皮屑。所有標本均先行鏡檢,無1例發現菌絲或假菌絲。將標本接種于沙氏葡萄糖培養基,置25℃恒溫箱內連續培養5 d,逐日觀察,2周內不生長,判斷為陰性;發現真菌及酵母樣可疑菌落,轉種沙氏葡萄糖培養基斜面,獲得純培養后鑒定。根據菌落形態特征及顏色、菌落生長的快慢、鏡下孢子及菌絲的特征鑒定。念珠菌加用法國柯瑪嘉顯色培養基,30~37℃培養48 h,根據念珠菌顯色培養說明書判斷結果,綠色、翠綠色菌落判斷為白念珠菌;藍灰色、鐵灰色為熱帶念珠菌;紫紅色邊緣模糊,有微毛,判斷為克柔念珠菌;整個菌落紫紅色判斷為光滑念珠菌;白色菌落判斷為其他念珠菌。AD患者皮損及非皮損部位共培養出念珠菌48株,其中白念珠菌16株,熱帶念珠菌11株,克柔念珠菌9株,光滑念珠菌5株,其他念珠菌7株。
4.統計方法:用SPSS13.0統計軟件,χ2檢驗分析陽性率差異,P<0.05為差異有統計學意義。
二、結果
見表1。AD患者皮損部位念珠菌、紅酵母定植陽性率明顯高于健康對照組,χ2值分別為6.23、4.10,均P< 0.05;兩組間曲霉、青霉陽性率差異無統計學意義,χ2值分別為1.17、0.17,均P>0.05。AD患者非皮損部位念珠菌、紅酵母、曲霉、青霉定植陽性率與健康對照組比較,差異均無統計學意義,χ2值分別為1.07、1.70、0.58、0.30,P> 0.05。AD患者皮損部位念珠菌陽性率明顯高于非皮損部位(χ2=4.00,P<0.05);而紅酵母、曲霉、青霉兩組間差異無統計學意義,χ2值分別為0.42、0.17、1.56,均P> 0.05。
重度AD患者皮損部位念珠菌、紅酵母定植陽性率明顯高于中度患者,χ2值分別為6.65、4.37,均P< 0.05;青霉、曲霉兩組間差異無統計學意義,χ2值分別為0.35、0.86,均P>0.05。重度AD患者非皮損部位念珠菌陽性率明顯高于中度患者,χ2=4.16,P<0.05;紅酵母、曲霉、青霉兩組間差異無統計學意義,χ2值分別為1.59、0.33、2.05,P> 0.05。見表1。
三、討論
皮膚屏障功能障礙可能是引起AD等干燥性皮膚病的主要原因,皮膚屏障功能破壞,增加了對外界不同刺激的敏感性,使環境的過敏原,如花粉、屋塵螨和微生物等容易穿透皮膚,產生sIgE抗體,使AD患者的病情加重。真菌在皮膚表面的定植情況與皮膚的生理條件及健康狀況相關[3],真菌致敏原在遺傳過敏性疾病中發揮重要作用[4],AD患者的汗液中有一種主要變應原,是由球形馬拉色菌產生的真菌蛋白mgl?1304,可引起Ⅰ型變態反應[5];超過三分之二以頭頸部為主要表現的成人特應性皮炎患者對伊曲康唑和其他唑類抗真菌藥物有明顯的療效[6]。AD患者皮膚表面定植的真菌包括念珠菌、馬拉色菌、青霉、曲霉[7],SCORAD評分與曲霉、馬拉色菌、青霉、念珠菌的sIgE水平有顯著相關性[8]。本研究中,AD患者皮損部位念珠菌定植陽性率為58%。一項關于AD患者念珠菌的皮膚點刺試驗中,70%發生速發型過敏反應[9];而Chang等[10]報道,81.2%的AD患者血清中檢測到念珠菌特異性IgE。真菌孢子在環境中普遍存在,室外最常見的真菌致敏原是枝孢菌和鏈格孢,室內最常見的是曲霉和青霉,它們的存在不受季節影響。本試驗中曲霉、青霉皮膚表面定植陽性率與健康對照沒有顯著差別。
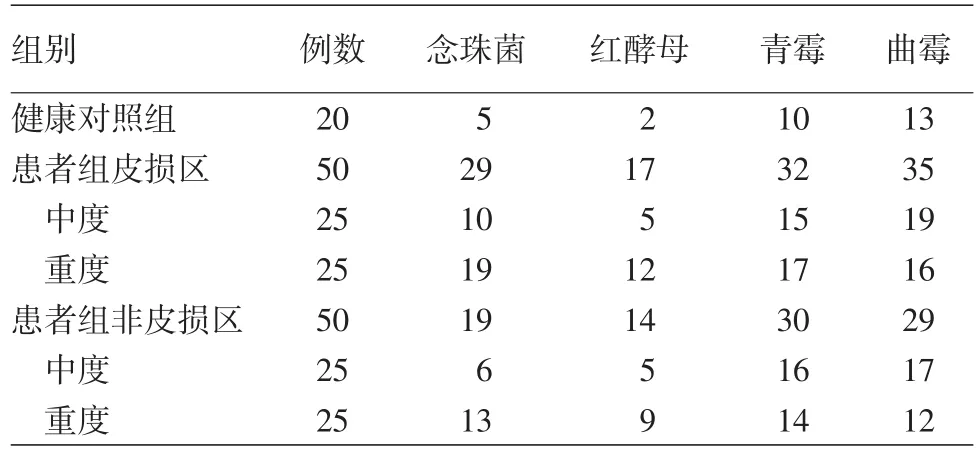
表1 特應性皮炎患者皮損及非皮損部位4種真菌培養結果(例)
[1]Sonesson A,Bartosik J,Christiansen J,et al.Sensitization to skin?associated microorganisms in adult patients with atopic dermatitis is of importance for disease severity[J].Acta Derm Venereol,2013,93(3):340?345.DOI:10.2340/00015555?1465.
[2] Williams HC.Diagnostic criteria for atopic dermatitis[J].Lancet,1996,348(9038):1391 ?1392.DOI:10.1016/S0140 ?6736(05)65466?9.
[3] Zhang E,Tanaka T,Tajima M,et al.Characterization of the skin fungal microbiota in patients with atopic dermatitis and in healthy subjects[J].Microbiol Immunol,2011,55(9):625 ?632.DOI:10.1111/j.1348?0421.2011.00364.x.
[4]劉芳,桑紅,胡文星,等.淺部真菌感染和變態反應性皮膚病相關性研究[J].中國真菌學雜志,2011,6(6):344?349.DOI:10.3969/j.issn.1673?3827.2011.06.007.Liu F,Sang H,Hu WX,et al.Correlation of superficial fungal infections and allergic skin diseases[J].Chin J Mycol,2011,6(6):344?349.DOI:10.3969/j.issn.1673?3827.2011.06.007.
[5]Hiragun T,Ishii K,Hiragun M,et al.Fungal protein MGL_1304 in sweat is an allergen for atopic dermatitis patients[J].J Allergy Clin Immunol,2013,132(3):608 ?615e4.DOI:10.1016/j.jaci.2013.03.047.
[6]Kaffenberger BH,Mathis J,Zirwas MJ.A retrospective descriptive study of oral azole antifungal agents in patients with patch test?negative head and neck predominant atopic dermatitis[J].J Am Acad Dermatol,2014,71(3):480?483.DOI:10.1016/j.jaad.2014.04.045.
[7]Zhang E,Tanaka T,Tajima M,et al.Characterization of the skin fungal microbiota in patients with atopic dermatitis and healthy subjects[J].Microbiol Immunol,2011,55(9):625?632.DOI:10.1111/j.1348?0421.2011.00364.x.
[8]Ong PY,Ferdman RM,Church JA.Association of microbial IgE sensitizations with asthma in young children with atopic dermatitis[J].Ann Allergy Asthma Immunol,2012,108(3):212?213.DOI:10.1016/j.anai.2011.12.016.
[9]Kobayashi T,Yamada M,Aihara M,et al.Immedeate and delayed?type reactivity to fungi and effects of antifungal drugs on atopic dermatitis[J].Arerugi,2006,55(2):126?133.PMID:16719000.
[10]Chang FY,Lee JH,Yang YH,et al.Analysis of the serum levels of fungi?specific immunoglobulin E in patients with allergic diseases[J].Int Arch Allergy Immunol,2011,154(1):49?56.DOI:10.1159/000319208.
Analysis of fungal colonization in skin surfaces of patients with atopic dermatitis
Zhang Xiuqin,Cheng Bo,Ji Mingkai,Fang Fang,Su Huichun
Department of Dermatology,Xiamen Haicang Hospital,Xiamen 361026,Fujian,China(Zhang XQ);Department of Dermatology,First Affiliated Hospital of Fujian Medical University,Fuzhou 350005,China(Cheng B,Ji MK,Fang F,Su HC)
ObjectiveTo analyze the colonization ofCandida,Rhodotorula,PenicilliumandAspergillusin skin surfaces of patients with atopic dermatitis,and to assess the relationship between the four common fungal allergens and severity of atopic dermatitis.MethodsFifty patients with atopic dermatitis and 20 healthy controls were enrolled.Scales were scraped from lesional and non?lesional skin of flexural extremities of the patients,as well as from normal skin of the flexural elbow of healthy controls,then were subjected to microscopic examination and culture.Scale specimens were inoculated onto Sabouraud dextrose agar medium and cultured at 25℃in a constant temperature incubator.Subsequently,suspected fungal or yeast?like colonies were collected for pure culture.Finally,fungal strains were identified according to colony morphology,color,growth speed,as well as microscopic features of spores and hyphae.ResultsNo hyphae or pseudohyphae were found in any case by microscopic examination.Candida albicansandRhodotorulawere detected in 29(58%)and 17(34%)out of the 50 patients,respectively,and in 5(25%)and 2(10%)out of the 20 healthy controls,respectively.The detection rates ofCandida albicansandRhodotorulawere significantly higher in the patients than in the controls(χ2=6.23,4.10,respectively,bothP< 0.05).Of 25 patients with severe lesions,19(76%)and 12(48%)were colonized byCandida albicansandRhodotorularespectively;among 25 patients with moderate lesions,10(40%)and 5(20%)were colonized byCandida albicansandRhodotorularespectively.An increase was observed in the detection rates ofCandida albicansandRhodotorulain the patients with severe lesions compared with those with moderate lesions(χ2=6.65,4.37,respectively,bothP< 0.05).There was no significant difference in the detection rate ofPenicilliumorAspergillusbetween the patients and health controls.ConclusionThe colonization rates ofCandida albicansandRhodotorulaon skin surfaces were higher in patients with atopic dermatitis than in healthy controls,and higher in patients with severe lesions than in patients with moderate lesions,indicating that the types of colonizing fungi are associated with the health status of skin and severity of symptoms in patients with atopic dermatitis.
Dermatitis,atopic;Candida albicans;Rhodotorula;Penicillium chrysogenum;Aspergillus
Cheng Bo,Email:chengbo630415@126.com
程波,Email:chengbo630415@126.com
10.3760/cma.j.issn.0412?4030.2016.07.015
2015?07?28)
(本文編輯:吳曉初)