國人喙突的解剖特點及在Latarjet術的應用
2015-06-26 13:00:23連建強董樂樂魏海濤張文龍賈建新
中華肩肘外科電子雜志 2015年4期
連建強 董樂樂 魏海濤 張文龍 賈建新
?
·論著·
國人喙突的解剖特點及在Latarjet術的應用
連建強1董樂樂1魏海濤1張文龍1賈建新2
目的 通過尸體解剖研究喙突及其韌帶附著點的特點,了解在行Latarjet術時,國人喙突的截骨量、喙突解剖與體長的關系。方法 解剖15具30肩男性防腐成人尸體,測量喙突長度,喙突尖寬度、高度,喙突尖到中點距離,喙突中點寬度、高度,喙突尖到胸小肌前界、后界距離,胸小肌喙突止點寬度,喙突尖到喙肩韌帶前界、后界距離,喙肩韌帶喙突止點寬度,喙突尖到斜方韌帶與錐狀韌帶最大距離(安全區域),然后進行統計學處理。結果 (1)喙突平均長度(42.10±2.3) mm,喙突中點平均寬度(15.29±1.70) mm,中點平均高度(11.61±1.98) mm,“安全區域”平均距離(23.93±2.32) mm;(2)內踝尖到同側眉弓距離的線性回歸方程Y=-16.747+4.971喙突尖到斜方韌帶與錐狀韌帶的最大距離-3.469喙突中點高度-0.536喙突尖高度;(3)胸小肌止點變異率為23.33%,變異可為單側或雙側,無規律性。結論 (1)行Latarjet術時,國人喙突截骨量應小于西方文獻報道量;剝離喙突上胸小肌止點時,應關注其解剖變異;(2)患者身高與喙突可截骨量成正比,與喙突高度成反比,故身高越高,越不宜行Latarjet改良手術。
肩關節;喙突;解剖學;關節鏡
肩關節前方不穩定是常見的肩關節運動損傷,肩關節鏡下關節囊盂唇修復術仍是肩關節前方不穩定的常用手術方式,但文獻報道其復發率較高,尤其是肩盂前緣嚴重骨質缺損的患者[1]。對于這一類患者,關節鏡下Latarjet手術可獲得良好的效果[2]。Latarjet手術喙突截骨時,不同的人種,喙突截骨量大小不同,最新美國一篇文獻報道其平均截骨量28.5 mm[3],巴西的一篇文獻報道為26.4 mm[4]。查閱國內文獻,僅發現一篇關于國人喙突的解剖研究[5],但此文獻研究對象為干燥肩胛骨標本,對臨床關節鏡下喙突截骨指導有限。本文通過防腐尸體解剖主要研究:(1)喙突上附著韌帶止點的解剖特點;(2)Latarjet手術時,國人喙突的截骨量;(3)喙突解剖與體長的關系。
材 料 與 方 法
15具30肩防腐成人尸體標本,全部為男性,取肩關節倒“7”型切口,切口跨過喙突尖,切除局部皮膚、皮下組織,并切斷部分三角肌充分顯露喙突、鎖骨外段及肩峰。仔細解剖喙突上附著的聯合腱、喙肩韌帶止點、胸小肌止點及喙鎖韌帶的前界,并用標記筆標記。用精度為0.02 mm的游標卡尺,由課題組任意2名成員完成, 每人分別兩次測量喙突長度:(1)喙突尖的寬度。(2)喙突尖的高度。(3)喙突尖中點距離。(4)喙突中點寬度。(5)喙突中點高度。(6)喙突尖到胸小肌前界(A),喙突尖到胸小肌后界(B),胸小肌喙突止點寬度(C),喙突尖到喙肩韌帶前界(D),喙突尖到喙肩韌帶后界(E),喙肩韌帶喙突止點寬度(F),喙突尖到斜方韌帶與錐狀韌帶的最大距離(G,安全區域),見圖1~5,取其平均值,如果任意兩次測量數值差別較大,則由第三人重新測量,測量者互盲。
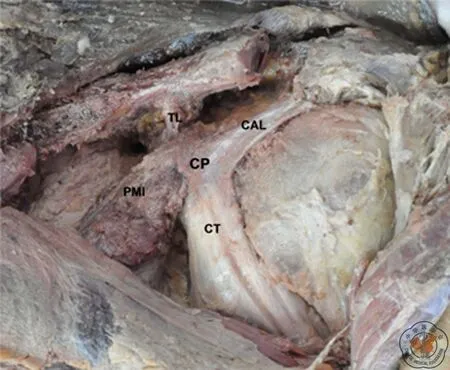
圖1 左肩關節喙突的解剖結構 CAL:喙肩韌帶,CT:聯合腱,CP:喙突尖,PMI:胸小肌,TL:錐狀韌帶
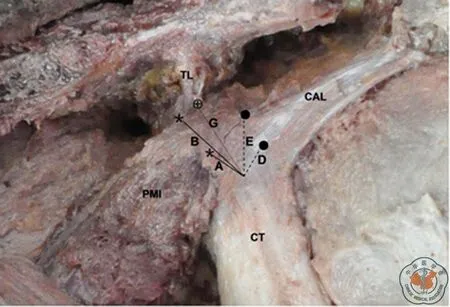
圖2 左肩關節喙突的解剖結構 CAL:喙肩韌帶,CT:聯合腱, PMI:胸小肌,TL:錐狀韌帶,A:喙突尖到胸小肌前界,B:喙突尖到胸小肌后界,D:喙突尖到喙肩韌帶前界,E:喙突尖到喙肩韌帶后界,G:喙突尖到斜方韌帶與錐狀韌帶的最大距離(安全區域),兩*之間:胸小肌喙突止點寬度(C),兩●之間:喙肩韌帶喙突止點寬度(F)
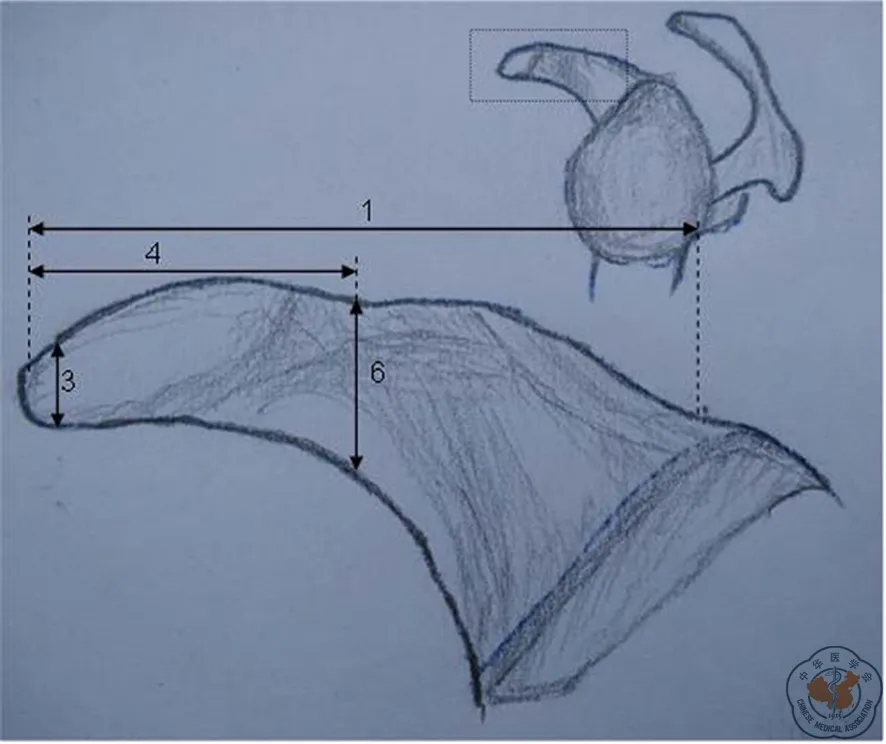
圖3 左喙突外側面觀模式圖 1:喙突長度,3:喙突高度,4:喙突尖中點距離, 6:中點高度
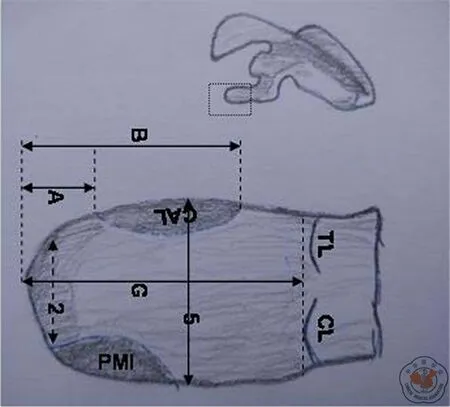
圖4 左喙突上面觀模式圖 2:喙突尖的寬度,5:喙突尖中點距離,CAL:喙肩韌帶,PMI:胸小肌,TL:錐狀韌帶,CL:斜方韌帶,A:喙突尖到胸小肌前界,B:喙突尖到胸小肌后界, G:喙突尖到斜方韌帶與錐狀韌帶的最大距離(安全區域)
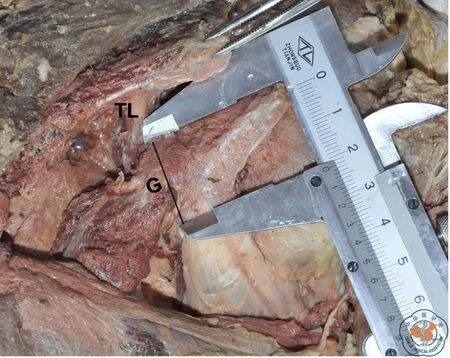
圖5 左肩關節喙突的解剖結構 G:喙突尖到斜方韌帶與錐狀韌帶的最大距離(安全區域)
本實驗中,因為錐狀韌帶喙突止點前于斜方韌帶,故“安全區域”是指喙突尖到喙鎖韌帶的錐狀韌帶的前界(即“喙突肘部”)的距離。并且測量每具尸體內踝尖到同側眉弓的距離。所得數據采用SPSS 13.0軟件分析,分別求證均數、標準差、極大值、極小值、99%有效區間,及體長與上述測量值的相關性。
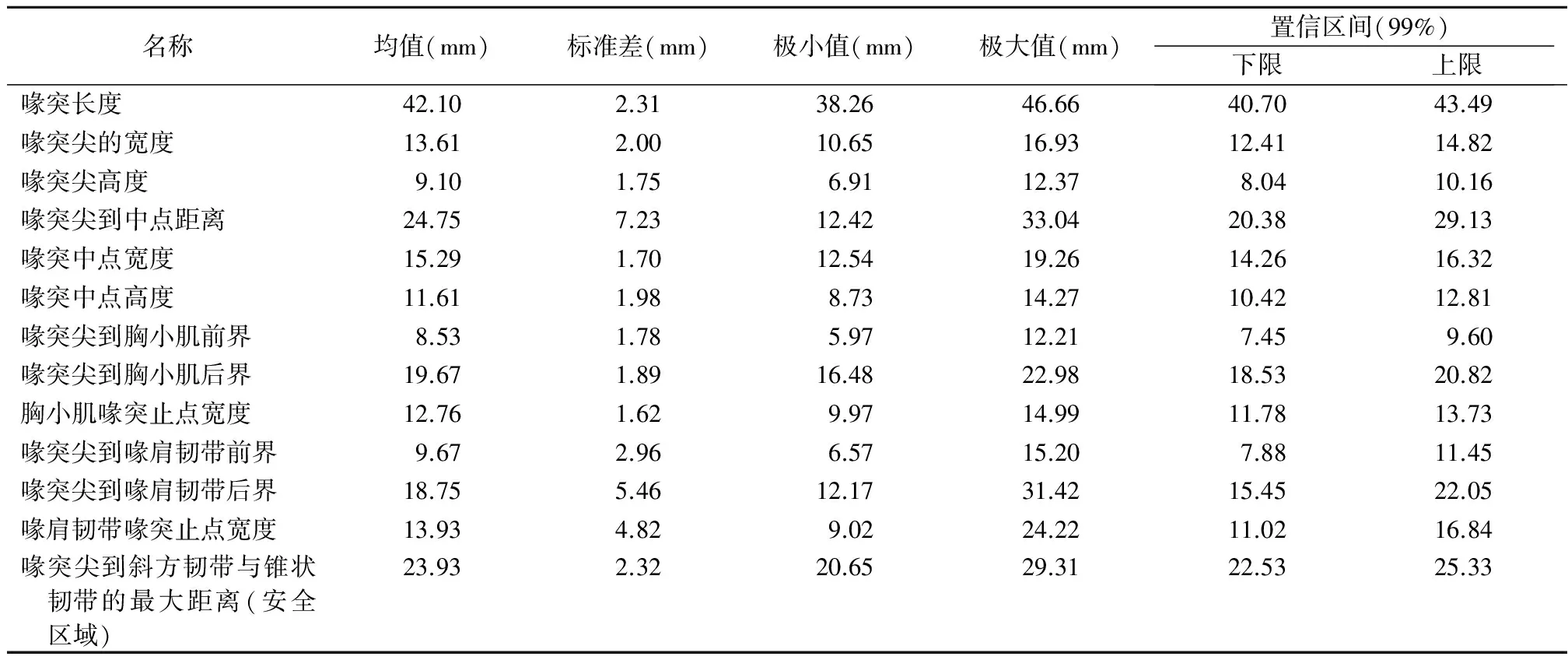
表1 喙突骨性結構及其韌帶止點的解剖測量
結 果
喙突解剖數據見表1。喙突的平均長度(42.10±2.3) mm,喙突尖平均寬度(13.61±2.00) mm、平均高度(9.10±1.75) mm,喙突尖到中點的平均距離(24.75±7.23) mm,喙突中點的平均寬度(15.29±1.70) mm,中點平均高度(11.61±1.98) mm,喙突尖到胸小肌前界平均距離(8.53±1.78) mm,喙突尖到胸小肌后界平均距離(19.67±1.89) mm,胸小肌喙突止點平均寬度(12.76±1.62) mm,喙突尖到喙肩韌帶前界平均距離(9.67±2.96) mm,喙突尖到喙肩韌帶后界平均距離(18.75±5.46) mm,喙肩韌帶喙突止點平均寬度(13.93±4.82) mm,喙突尖到斜方韌帶與錐狀韌帶的最大距離的平均距離(23.93±2.32) mm。
多元線性回歸方程如:Y(內踝尖到同側眉弓的距離)=-16.747+4.971左側喙突尖到斜方韌帶與錐狀韌帶的最大距離-3.469喙突中點高度-0.536喙突尖的高度。
討 論
1954年,Latarjet[6]報道了Latarjet術式,該術式將喙突由基底部截斷,穿過沿肌纖維走行縱劈的肩胛下肌,移位固定至肩盂前緣2點到6點的位置。同年,Helfet[7]指出喙突截骨量為尖部以近10 mm。May[8]提出喙突截骨量為喙突尖到喙肱韌帶起始部。Mead主張截骨量為喙突尖以近10~30 mm。Freehill等[9]指出截骨量約為25 mm,截骨塊附帶部分喙鎖韌帶。Burkhart等[10]提出截骨點為喙突“肘部”,但未明確“肘部”的準確概念。目前,大部分肩肘外科專家行喙突截骨時,嚴格遵從“安全區域”原則,“安全區域”是指喙突尖到喙鎖韌帶的錐狀韌帶的前界(即“喙突肘部”)的距離。最近美國一篇文章報道:“安全區域”平均距離為28.5 mm[3],巴西一篇文獻報道為26.4 mm[4]。本實驗結果:“安全區域”為(23.93±2.32) mm,與國外兩篇報道數據相比較小,但這一點與姜春巖教授的報道相符[1]。
2010年由Beer等[11]改良的Latarjet手術,建議喙突截骨塊沿其長軸內旋90°轉位,再移植到關節盂前下方,使喙突下緣和關節面平齊。2013年Boons等[12]指出傳統術式與改良術式在肩關節的活動度、僵硬程度無明顯差別,改良術式可增加肱骨頭在關節內向前滑動的范圍,但還需進一步研究,哪一種術式占絕對優勢。2012年Giles等[13]指出改良術式骨塊固定穩定性明顯差于傳統術式,但與關節盂前緣密切結合,可能會產生良好的遠期療效。就目前國外文獻報道,還沒有明確指出Latarjet術式的選擇受喙突寬高比的影響。國內向明等[2]教授也報道了傳統Latarjet手術與改良術式的比較研究,他認為喙突骨塊寬度大于厚度,平行轉位時與肩盂的接觸面積較大,能用兩枚3.5 mm皮質骨螺絲釘固定,可提供更高的強度;相反內旋90°轉位喙突骨塊與肩盂的接觸面積較小,只能用兩枚3.0 mm中空螺絲釘固定,因此,喙突骨塊平行轉位時較內旋90°轉位有更大的接觸面積和生物力學強度,從而提高骨塊愈合率。但內旋90°轉位可提供更大的關節面安全范圍,有利于肩盂骨缺損較大的患者[2]。
本實驗研究發現喙突寬度大于高度,這與向明教授的觀點一致。多元線性回歸方程指出內踝尖到同側眉弓的距離與“安全區域”成正比,與喙突尖高度、喙突中點高度成反比,這一點說明患者的身高越高,“安全區域”越大,喙突截骨量越大,但喙突高度越小,越不宜行Latarjet改良手術。Terra等[4]還指出喙突尖到胸小肌止點后界每增加10 mm,“安全區域”增大8.5 mm,但本實驗未發現喙突尖到胸小肌后界距離與“安全區域”有相關性。
國外文獻報道:胸小肌止點變異率為15%,胸小肌異常附著點引起的功能障礙時,需要將其移位致喙突[14]。2000年張增方等[15]報道:胸小肌止點變異率為19.38%,變異者均為雙側對稱一致的,并將其分為單腱型及雙腱型,雙腱型又分為兩亞型。同年,孟文件等[16]報道胸小肌止點跨過喙突止于關節囊內層一病例,本實驗可見胸小肌止點跨過喙突尖止于上關節囊4側(圖6),胸小肌小部分止于喙突而大部分止于上關節囊3側,胸小肌止點總變異率為23.33%,且變異者可雙側不對稱,無規律性。這一解剖變異提示肩肘外科醫生臨床行Latarjet手術時,剝離喙突上胸小肌止點時,還需進一步關注其解剖變異,以免造成上關節囊松弛,導致醫源性關節疾病。
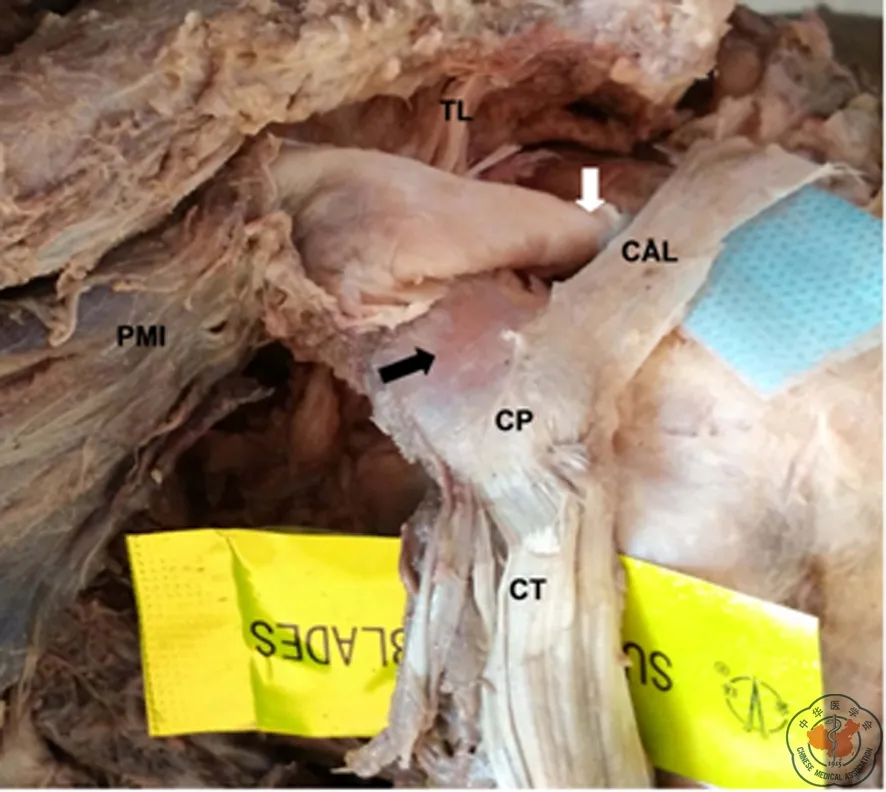
圖6 左肩關節胸小肌喙突止點變異解剖結構 CAL:喙肩韌帶,CT:聯合腱,CP:喙突尖,PMI:胸小肌,TL:錐狀韌帶,“”:胸小肌止點入關節囊點,“”胸小肌止點喙突壓跡
不足之處:本實驗測量三維結構標本,建立一個標準的測量點較困難,為了減小此誤差,由任意兩名熟悉測量的成員完成測量,每人分別兩次測量同一部位,取其平均值,若兩人數值差距較大時,由第三人重新測量。另外,本實驗數據基于尸體解剖,受試者一般資料不全,且均為成年男性,實驗數據存在偏倚。下一步計劃增加樣本量,使實驗數據更具代表性。
[1] 姜春巖,吳關,魯誼,等.關節鏡下喙突移位術:手術技術與早期隨訪探討[J].中國運動醫學雜志,2014,33(4):297-302, 311.
[2] 向明,楊國勇,陳杭,等.Latarjet兩種術式治療肩關節復發性前脫位伴重度骨缺損3~5年隨訪的比較研究[J/CD].中華肩肘外科電子雜志,2014,2(1):33-40.
[3] Dolan CM, Hariri S, Hart ND, et al. An anatomic study of the coracoid process as it relates to bone transfer procedures[J]. J Shoulder Elbow Surg, 2011, 20(3): 497-501.
[4] Terra BB, Ejnisman B, De Figueiredo EA, et al. Anatomic study of the coracoid process: safety margin and practical implications[J]. Arthroscopy, 2013, 29(1): 25-30.
[5] 馮沃君,楊會營,王軍.喙突的解剖學測量及其臨床意義[J].中醫外治雜志,2011,20(5):7-8.
[6] Latarjet M. Treatment of recurrent dislocation of the shoulder[J]. Lyon Chir,1954,49(8):994-997.
[7] Helfet AJ. Coracoid transplantation for recurring dislocation of the shoulder[J]. J Bone Joint Surg Br, 1958, 40B(2): 198-202.
[8] May VR. A modified Bristow operation for anterior recurrent dislocation of the shoulder[J]. J Bone Joint Surg Am, 1970, 52(5): 1010-1016.
[9] Freehill MT, Srikumaran U, Archer KR, et al. The latarjet coracoid process transfer procedure: alterations in the neurovascular structures[J]. J Shoulder Elbow Surg, 2013, 22(5): 695-700.
[10] Burkhart SS, De Beer JF, Barth JR, et al. Results of modified Latarjet Reconstruction in patients with anteroinferior instability and significant bone loss[J]. Arthroscopy, 2007, 23(10): 1033-1041.
[11] De Beer JF, Roberts C. Glenoid bone defects--open latarjet with congruent arc modification[J]. Orthop Clin North Am, 2010, 41(3): 407-415.
[12] Boons HW, Giles JW, Elkinson I, et al. Classic versus congruent coracoid positioning during the Latarjet procedure: an in vitro biomechanical comparison[J]. Arthroscopy, 2013, 29(2): 309-316.
[13] Giles JW, Puskas G, Welsh M, et al. Do the traditional and modified latarjet techniques produce equivalent Reconstruction stability and strength?[J]. Am J Sports Med, 2012, 40(12): 2801-2807.
[14] Rockwood CA.肩關節外科學[M].北京:人民軍醫出版社,2012:51.
[15] 張增方,杜建春,張巖,等.胸小肌止點變異的解剖學研究[J].中華創傷骨科雜志,2004,6(9):1080.
[16] 孟文件,常寶林,劉漢鋒,等.雙側胸小肌止點變異1例[J].中國臨床解剖學雜志,2000,18(1):67.
(本文編輯:李靜)
連建強,董樂樂,魏海濤,等.國人喙突的解剖特點及在Latarjet術的應用[J/CD]. 中華肩肘外科電子雜志,2015,3(4):233-237.
The anatomical features of coracoid of Chinese population as well as their applications in Latarjet operation
LianJianqiang1,DongLele1,WeiHaitao1,ZhangWenlong1,JiaJianxin2.
1TheSecondEndemicArea,DepartmentofOrthopedics,theFirstAffiliatedHospitalofBaotouMedicalCollege,Baotou014010,China;2DepartmentofAnatomy,BaotouMedicalCollege,Baotou014010,China
Correspondingauthor:DongLele,Email:dong_le_le@126.com
Background Anterior shoulder instability is a common sport injury of shoulder joint, and bankart repair under shoulder arthroscopy is still common operation method for anterior shoulder instability. However, some literatures report this operation method has high recurrence rate, in particular for the patients with serious bony defect at anteior glenoid rim. For the treatment of such patients, arthroscopic Latarjet operation can achieve satisfactory effects. In Latarjet coracoid osteotomy, different races vary in coracoid osteotomy quantity. Recently, an American literature reported that the average coracoid osteotomy quantity is 28.5 mm, and a Brazilian literature reported it as 26.4 mm. By referring to domestic literatures, we only found one literature regarding the anatomic study on coracoid of Chinese population. However, the research object of this literature is dry scapula specimen, so that this literature has limited instructions on clinical arthroscopic coracoid osteotomy. Through autopsy of Formalined cadaver, this article mainly studies the following:(1) The anatomical features of ligament end point attached on coracoid;(2) In Latarjet operation, the osteotomy quantity of coracoid of Chinese population;(3) The relation between coracoid anatomy and body length.Methods For 15 Formalined male cadaver specimens with 30 shoulders (all male cadaver specimens), take inversed "7" form incision on shoulder joint, with incision crossing coracoid tip, remove local skin and subcutaneous tissues, and cut off partial deltoid, sufficiently exposed coracoid, outer segment of clavicular and acromion. Carefully dissect the conjoint tendon attached on coracoid, the coracoacromial ligament end point, musculus pectoralis minor end point and the anterior hyaloid of coracoclavicular ligament, and use a marker pen to mark these positions;By using vernier caliper with accuracy of 0.02 mm, any two members of research group are assigned to complete this operation. Each member respectively measure the following data twice: coracoid length:(1)width of coracoid tip;(2)height of coracoid tip ;(3) distance from center point of coracoid tip;(4)width of coracoid center point ;(5)height of center point;(6)Coracoid tip to musculus pectoralis minor anterior (A), coracoid tip to musculus pectoralis minor posterior (B), width of musculus pectoralis minor coracoid end point (C), coracoid tip to coracoacromial ligament posterior (D), coracoid tip to coracoacromial ligament posterior (E), width of coracoacromial ligament coracoid end point (F), maximum distance from coracoid tip to trapezoid ligament and conoid ligament (G, safety zone), take the mean value, if there is major difference between values measured at any two times, it is necessary to assign a third person to make measurement again, with measurers being mutually blind. In this test, since the conoid ligament coracoid end point is anterior to trapezoid ligament, the "safety zone" refer to the distance from the coracoid tip to the anterior of the conoid ligament of coracoclavicular ligament (namely "coracoid elbow"). In addition, measure the distance from medial malleolus tip to superciliary arch in each corpse. Use SPSS 13.0 software to analyze the obtained data; respectively verify the correlations among mean, standard deviation, maximum value, minimum value, 99% effective bargaining section and body length with said measured values.Results The average length of coracoid is (42.10±2.3) mm, the average edge line of coracoid tip is (13.61±2.00) mm, average height is (9.10±1.75), the mean distance from coracoid tip to center point is (24.75±7.23) mm, the mean width of coracoid center point is (15.29±1.70) mm, the average height of center point is (11.61±1.98) mm, the mean distance from coracoid tip to musculus pectoralis minor anterior is (8.53±1.78) mm, the mean distance from coracoid tip to musculus pectoralis minor posterior is (19.67±1.89) mm, the mean width of musculus pectoralis minor coracoid end point is (12.76±1.62) mm, the mean distance from coracoid tip to coracoacromial ligament anterior is (9.67±2.96) mm, the mean distance from coracoid tip to coracoacromial ligament posterior is (18.75±5.46) mm, the mean width of coracoacromial ligament coracoid end point is (13.93±4.82) mm, and the mean distance of the maximum distance from coracoid tip to trapezoid ligament and conoid ligament is (23.93±2.32) mm. Multivariate equation of linear regression: Y (distance from medial malleolar tip to superciliary arch on same side)=-16.747+4.971 the maximum distance of left side coracoid tip to trapezoid ligament and conoid ligament -3.469 coracoid center point height -0.536 Height of coracoid tip.Conclusions (1)In Latarjet operation, the coracoid osteotomy quantity of Chinese population shall be less than the quantity reported by western literatures; In the stripping the musculus pectoralis minor end point on coracoid, it is necessary to pay close attention to its anatomic variation;(2) The body height of the patients is proportional to the osteotomy quantity of coracoid and is inversely proportional to the height of coracoid. Therefore, the higher the body height is, Latarjet procedure is even not suitable.
Shoulder;Coracoid;Anatomy;Arthroscopy;Latarjet
10.3877/cma.j.issn.2095-5790.2015.04.007
014010包頭醫學院第一附屬醫院骨科二病區1;014040包頭醫學院解剖教研室2
董樂樂,Email:dong_le_le@126.com
2015-05-04)