肩關節前方松解治療原發性凍結肩的回顧性研究
2015-06-26 13:00:23陳建海劉中邸黨育楊明蘆浩張殿英付中國
中華肩肘外科電子雜志 2015年4期
陳建海 劉中邸 黨育 楊明 蘆浩 張殿英 付中國
?
·論著·
肩關節前方松解治療原發性凍結肩的回顧性研究
陳建海 劉中邸 黨育 楊明 蘆浩 張殿英 付中國
目的 探討肩關節鏡下肩關節前方松解對于原發性凍結肩的治療效果。方法 回顧性分析2011年1月至2012年12月收治并行肩關節鏡下肩關節前方松解的病例資料,共入組26例,男性7例,女性19例,平均年齡55歲(41~69歲)。術前進行Constant評分、簡明肩關節評分(SST)、肩關節活動范圍檢查和疼痛視覺模擬評分(VAS)。肩關節鏡下手術松解范圍包括喙肱韌帶、肩袖間隙、盂肱中韌帶、前方關節囊及盂肱下韌帶前部。術后規范康復鍛煉。在最后一次隨訪時進行肩關節活動范圍、Constant評分、SST評分和疼痛VAS評分。結果 獲得隨訪21例,隨訪率80.8%。平均隨訪時間31個月(29~36個月)。伴有糖尿病患者9例,占全部26例患者的34.6%。術前肩關節前屈上舉71.3°(50°~110°),術后改善至158.9°(150°~170°)。術前體側外旋5.6°(0°~15°),改善至術后57.5°(45°~70°)。術前Constant評分34.9分(13~71分),術后提高到90.4分(81~100分)。術前SST評分2.4分(0~7分)術后提高到10.1分(8~12分)。術前患側肩關節疼痛VAS評分平均7.9分(5~9分),術后提高到1.4分(0~3分)。結論 肩關節鏡下肩關節前方松解對于原發性凍結肩治療效果確切。
關節鏡;凍結肩;松解
肩關節僵硬是導致肩痛,影響患者生活質量的一個常見原因,以前常常稱為“肩周炎”。Rockwood在第4版《肩》中將肩關節僵硬分為原發性凍結肩和繼發性肩關節僵硬兩類[1]。原發性凍結肩是指在沒有肩關節明確疾患的情況下,肩關節出現多平面的主、被動活動受限,可以伴有系統性疾病如糖尿病[1]。原發性凍結肩人群發生率2%~5%,70%為女性,20%~30%會出現對側凍結肩[2]。多數經過保守治療可以獲得滿意的功能恢復,但仍有7%~50%患者殘留疼痛和功能受限[2]。關節鏡下肩關節松解術是對于保守治療無效的原發性凍結肩的有效治療方法[3-5]。與麻醉下手法松解相比,關節鏡下松解可以獲得更好的功能恢復、更好的疼痛緩解和更少的并發癥發生率[6]。關節鏡下松解的手術技術并沒有統一的標準,尤其是對于關節囊應該松解的范圍存在爭議,有的醫生只進行肩袖間隙松解[7],有的進行肩關節前方松解[8],有的進行肩關節前后下方松解[8],還有進行全關節囊松解[9]。本研究探討肩關節前方松解對于原發性凍結肩的治療效果。
資 料 與 方 法
一、一般資料
自2011年1月至2012年12月,共有37例患者以原發性凍結肩入院行肩關節鏡下松解術,患者入院前均經過保守治療,每位患者采用的保守治療方法可能有一種或幾種,如生活方式調整、休息、激素注射、口服抗炎止痛藥物、物理治療、康復鍛煉等。保守治療無效的標準:(1) 經上述保守方法治療后疼痛或者活動范圍沒有明顯改善;(2) 患者因疼痛或者嚴重的功能受限無法接受長期的保守治療。本研究入選標準:(1) 診斷為原發性凍結肩;(2) 術中松解范圍為肩袖間隙至6點位置;(3) 關節鏡松解前后均沒有進行麻醉下手法松解。排除標準:(1) 術中發現關節內合并其他損傷;(2) 松解范圍包含了后方關節囊;(3)同時進行了手法松解。共有26例患者符合入選標準,其中男性7例,女性19例,平均年齡55歲(41~69歲)。
二、手術方法
手術均在全身麻醉下進行,患者取沙灘椅體位,常規標畫體表標記。關節鏡常規經后入路插入盂肱關節腔,可見關節腔容積較小,關節囊內壁充血,滑膜增生;找到長頭肌腱后在其下方經體外進行針頭穿刺,建立前方工作入路。可見肩袖間隙、關節囊明顯增厚(圖1),使用射頻松解肩袖間隙,松解范圍包括長頭肌腱前緣、喙肱韌帶、肩袖間隙增生的滑膜組織(圖2);清晰顯露出肩胛下肌腱上緣,然后將肩關節輕度外旋,可見增厚的盂肱中韌帶(圖3),予以切斷;沿肩胛下肌后方從上到下切斷前方關節囊(圖4)和盂肱下韌帶前部(圖5,6)。確保前方關節囊松解徹底的標準是肩胛下肌在肩關節前方可以獲得清楚地顯示,一般下方松解到5-6點位置,關節鏡鞘可以順利通過盂肱關節間隙即可。下方關節囊和后方關節囊均不進行松解。使用射頻清理關節腔內壁充血增生的滑膜組織,并止血。將關節鏡轉入到肩峰下間隙,直視下建立前外側工作通道和后外側關節鏡第二觀察通道,進行肩峰下滑膜清掃,均不進行喙肩韌帶松解和肩峰前下緣成形,徹底止血。常規在盂肱關節腔和肩峰下間隙各注入復方倍他米松2 ml和利多卡因3 ml。術后康復:常規肩關節吊帶保護4周。術后第1周,進行肩關節被動上舉、外旋活動。第2周開始,在患者可以耐受的范圍內進行加強的關節上舉、外旋、內收的被動牽拉練習,患者可以在可耐受范圍內進行患肢的主動活動。術后1個月繼續關節牽拉練習,肩袖肌肉抗阻力鍛煉,肩胛帶肌肉抗阻力鍛煉,逐漸恢復日常使用。隨訪指標:患者在術前記錄患肩被動上舉、外旋范圍,術前Constant評分和簡明肩關節評分(simple shoulder test, SST),疼痛視覺模擬評分(Visual analogue scale,VAS)。在最后一次隨訪時進行肩關節活動范圍、Constant評分、SST評分和疼痛VAS評分。

圖1 肩袖間隙攣縮并滑膜增生
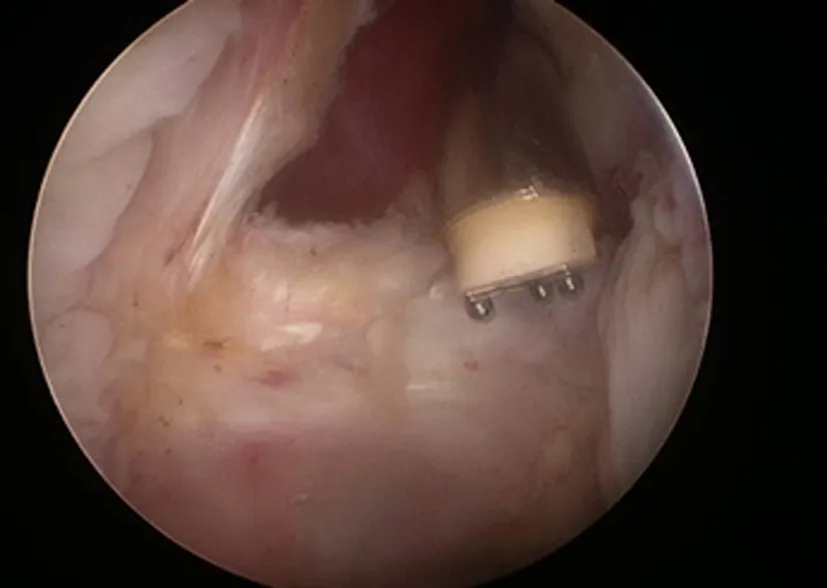
圖2 松解肩袖間隙及喙肱韌帶
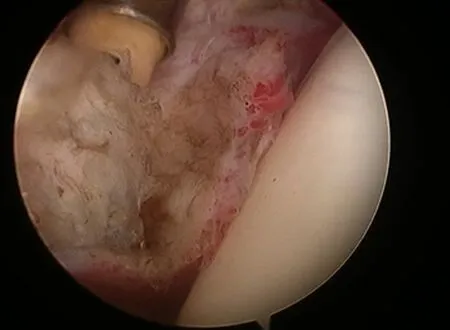
圖3 松解盂肱中韌帶
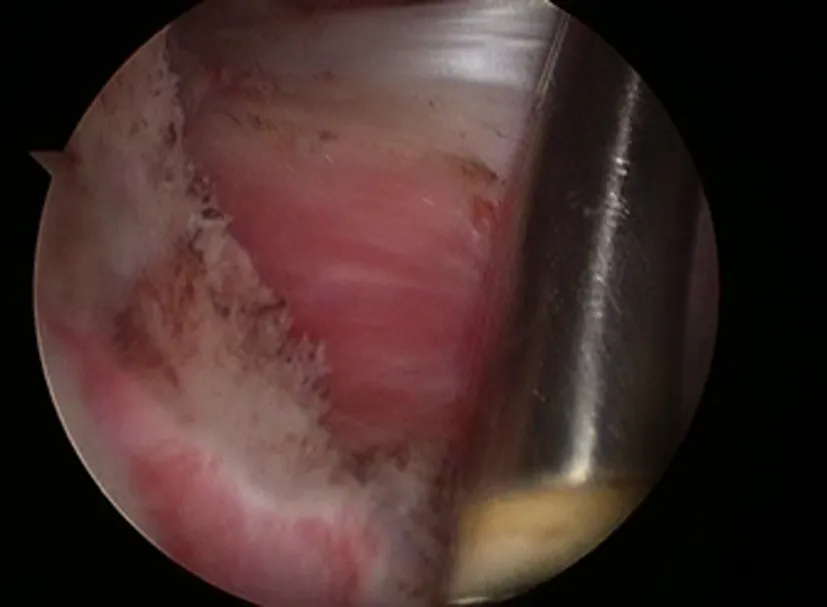
圖4 松解前方關節囊,盂肱中韌帶已經被切斷
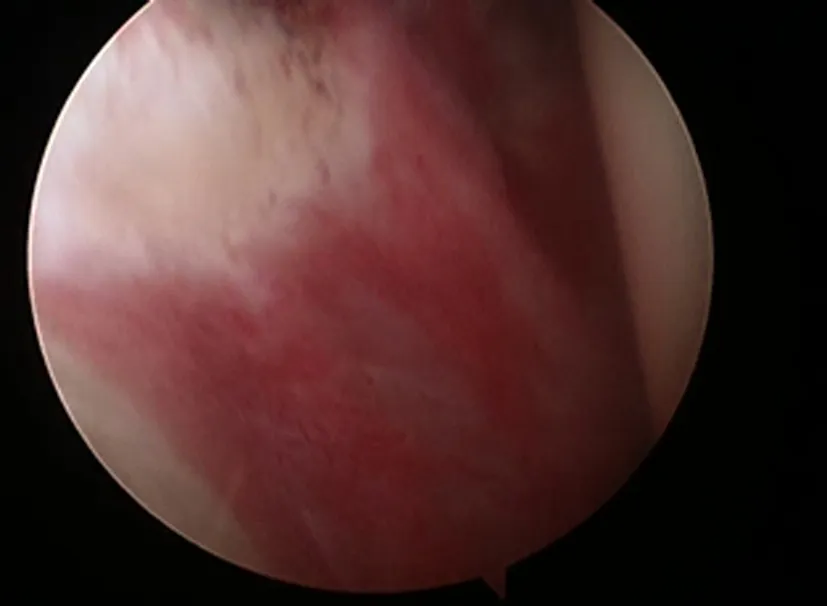
圖5 盂肱下韌帶前部充血并攣縮

圖6 盂肱下韌帶前部已經松解
三、統計學方法
計數資料均按照平均值和最大最小值范圍描述。
結 果
26例中獲得隨訪21例,隨訪率80.8%。平均隨訪時間31個月(29~36個月)。伴有糖尿病患者9例,占26例患者的34.6%。患者術前患側肩關節前屈上舉平均71.3°(50°~110°),到最后一次隨訪時平均158.9°(150°~170°)。術前體側外旋平均5.6°(0°~15°),到最后一次隨訪時平均57.5°(45°~70°)。患者術前患側肩關節Constant評分平均34.9分(13~71分),健側肩關節Constant評分92.8分(57~100分);到最后一次隨訪時患側肩關節Constant評分達到90.4分(81~100分),健側肩關節Constant評分95.6分(80~100分)。患者術前SST評分平均2.4分(0~7分),健側平均11分(4~12分);到最后一次隨訪時患側SST平均10.1分(8~12)分,健側平均11.6分(10~12)分。患者術前患側肩關節疼痛VAS評分平均7.9分(5~9分),到最后一次隨訪時平均1.4分(0~3分)。
討 論
原發性凍結肩是中老年人群肩痛的常見原因,Binder等[2]報道人群發生率達到2%~5%。以往常常認為原發性凍結肩是自限性疾病,但Binder等[2]的研究顯示有7%~50%存在不同程度的疼痛和功能受限。肩關節鏡下松解術是對于保守治療無效患者的一種有效治療手段[3-7,9-10]。
肩關節鏡在凍結肩治療中的應用最初還僅是用于關節腔檢查,Neviaser根據關節鏡觀察的結果將凍結肩分為4期[11-12]。Pollock等[7]較早報道通過關節鏡對凍結肩進行檢查,合并損傷的治療以及鏡下關節囊松解。在他的這組病例中,均是先進行手法松解,然后再進行關節鏡檢查和喙肱韌帶、肩袖間隙和前方關節囊松解,下方和后方關節囊都不進行松解。Ogilvie-Harris等[6]最早報道了肩關節鏡下松解與手法松解的臨床效果,關節鏡下松解范圍包括肩袖間隙、盂肱上韌帶、肩胛下肌腱的一部分、盂肱下韌帶前部及下方關節囊。結果顯示關節鏡松解在疼痛緩解和功能恢復上都明顯優于手法松解。Segmüller等[3]報道的關節鏡松解范圍又與前面不同,他先建立一個后下通道,進行關節囊從前方3點到后方9點的關節囊松解,如果外旋仍有受限,繼續松解盂肱中韌帶和肩袖間隙的有限清理。Bennett[13]報道的松解范圍則從前方的肩袖間隙,喙肱韌帶,盂肱上韌帶,盂肱中韌帶,到前方關節囊,盂肱下韌帶前后部,下方關節囊直至后上方關節囊。他認為如此廣泛的松解對原發性和繼發性凍結肩都有良好的松解效果。
對于凍結肩的手術治療,關節鏡技術已經占據主導地位,但手術松解范圍沒有統一的標準,從局限的前方松解直至關節囊360°松解均有大量報道[14]。Chen等[8]比較了前方關節囊松解與270°關節囊松解的手術效果,其中前方關節囊松解范圍與本研究相同,結果發現270°松解在術后3個月時關節活動范圍優于前方松解,在術后6個月時兩組病例關節功能沒有明顯區別。本研究結果顯示前方關節囊松解,肩關節功能可以獲得可靠的恢復。
原發性凍結肩往往表現為多個運動平面的活動范圍受限,如外旋、上舉和內收。前方關節囊的松解可以顯著改善外旋,包括體側外旋和外展外旋的角度。后方關節囊松解有利于改善內旋功能,但Snow等[15]比較前方松解與前方+后方松解的效果,并沒有發現對于內旋功能恢復的差異。本項回顧性研究僅進行前方關節囊松解,術中松解范圍從肩袖間隙到盂肱下韌帶前部,術中即可恢復正常范圍的上舉、體側外旋和外展外旋。我們選擇僅進行前方松解的主要原因在于:(1)外旋功能受限主要由于喙肱韌帶、肩袖間隙、盂肱上、中韌帶及盂肱下韌帶前部所致,松解此范圍即可獲得術中良好的外旋恢復;(2) 從臨床指導患者康復訓練來看,后方關節囊所致的水平內收和內旋可以比較容易通過康復鍛煉改善,術中松解后方關節囊的必要性小。
本項研究存在不足之處。首先這是一項回顧性研究,難免存在病例選擇的偏差。其次,缺乏臨床對照,前瞻性對照研究是我們下步研究的重點。有較多文獻報道糖尿病患者術后恢復效果差于普通患者,但本研究糖尿病患者病例數僅9例,不足以進行有效地統計學比較。對于糖尿病患者術后恢復效果的研究有待開展。
結論:原發性凍結肩經過規范保守治療無效的患者可以通過肩關節鏡松解手術獲得良好的功能恢復,肩關節前方松解可以獲得滿意療效。
[1] Rockwood CA, Matsen FA, Wirth MA, et al. The shoulder[M]. 4th ed.Philadelphia:Saunders Elsevier,2009:1405-1406.
[2] Binder AI, Bulgen DY, Hazleman BL,et al. Frozen shoulder: a long-term prospective study[J]. Ann Rheum Dis,1984,43(3):361-364.
[3] Segmüller HE, Taylor DE, Hogan CS, et al. Arthroscopic treatment of adhesive capsulitis[J]. J Shoulder Elbow Surg,1995,4(6):403-408.
[4] Warner JJ, Allen A, Marks PH, et al. Arthroscopic release for chronic, refractory adhesive capsulitis of the shoulder[J]. J Bone Joint Surg Am,1996,78(12): 1808-1816.
[5] Ogilvie-Harris DJ, Myerthall S. The diabetic frozen shoulder: arthroscopic release[J].Arthroscopy,1997,13(1):1-8.
[6] Ogilvie-Harris DJ, Biggs DJ, Fitsialos DP, et al. The resistant frozen shoulder: manipulation versus arthroscopic release[J]. Clin Orthop Relat Res, 1995,(319):238-248.
[7] Pollock RG, Duralde XA, Flatow EL, et al. The use of arthroscopy in the treatment of resistant frozen shoulder[J]. Clin Orthop Relat Res,1994,(304):30-36.
[8] Chen J, Chen S, Li Y, et al. Is the extended release of the inferior glenohumeral ligament necessary for frozen shoulder? [J]. Arthroscopy,2010,26(4):529-535.
[9] Jerosch J. 360 degrees arthroscopic capsular release in patients with adhesive capsulitis of the glenohumeral joint--indication, surgical technique, results[J]. Knee Surg Sports Traumatol Arthrosc, 2001,9(3):178-186.
[10] 鄭江.凍結肩[J/CD].中華肩肘外科電子雜志,2014, 2(3):191-195.
[11] Neviaser RJ, Neviaser TJ. The frozen shoulder. Diagnosis and management[J]. Clin Orthop Relat Res, 1987,(223):59-64.
[12] Neviaser TJ. Adhesive capsulitis[J]. Orthop Clin North Am,1987,18(3):439-443.
[13] Bennett WF. Addressing glenohumeral stiffness while treating the painful and stiff shoulder arthroscopically[J]. Arthroscopy, 2000,16(2):142-150.
[14] Jerosch J. 360 degrees arthroscopic capsular release in patients with adhesive capsulitis of the glenohumeral joint--indication, surgical technique, results[J]. Knee Surg Sports Traumatol Arthrosc, 2001,9(3):178-186.
[15] Snow M, Boutros I, Funk L. Posterior arthroscopic capsular release in frozen shoulder[J]. Arthroscopy,2009,25(1):19-23.
(本文編輯:胡桂英)
陳建海,劉中邸,黨育,等.肩關節前方松解治療原發性凍結肩的回顧性研究[J/CD]. 中華肩肘外科電子雜志,2015,3(4):227-232.
Aretrospectivestudyofanteriorarthroscopicarthrolysisfortreatmentofprimaryfrozenshoulder
ChenJianhai,LiuZhongdi,DangYu,YangMing,LuHao,ZhangDianying,FuZhongguo.
DepartmentofTraumaandOrthopaedics,PekingUniversityPeople′sHospital,PekingUniversityTrafficMedicineCenter,Beijing100044,China
Correspondingauthor:FuZhongguo,Email:fuzhongguo@vip.sina.com
Background Frozen shoulder is a common cause for shoulder pain and reduced quality of life in affected patients, which is formerly referred to as “peri-arthritis of shoulder." Rockwood divided frozen shoulder cases into primary and secondary categories in the fourth edition of "The Shoulder". Primary frozen shoulder refers to the presence of active and passive activity limitation at multiple planes without clear history of shoulder disorders, which maybe accompanied by systemic diseases such as diabetes. The incidence of primary frozen shoulder is 2%-5%, with 70% of female patients and contralateral shoulder stiffness in 20%-30% of the patients. Most patients have satisfactory functional recovery after conservative treatment, but residual pain and functional limitation may remain in 7%-50% of the patients. Arthroscopic arthrolysis is an effective treatment for primary frozen shoulder with failed conservative therapies. Compared with manipulation under anesthesia, arthroscopic arthrolysis can achieve better functional recovery, pain-relief and has fewer complications. The surgical techniques for arthroscopic arthrolysis do not have uniform standards. There are controversies especially for the range of joint capsular release, while some doctors only do rotator interval release, some release anterior shoulder, some release anterior, posterior and inferior shoulder and some do a full capsular release. This study investigated the efficacy of anterior shoulder release for the treatment of primary frozen shoulder.Methods From January 2011 to December 2012, a total of 37 patients with primary frozen shoulders were hospitalized to receive arthroscopic anthrolysis. Patients all
conservative therapy before hospitalization, the main content of which include: life style adjustment, rest, steroid injection, oral non-steroid anti-inflamatory medications, physical therapy, rehabilitation and so on. Each patient may receive one or more of the above conservative therapies. Criteria for conservative therapy failure: (1) no significant improvement in pain and motion limitation after the above conservative therapies; (2) patients cannot receive long-term conservative therapy due to pain or severe functional limitations. Inclusion criteria of this study: (1) Diagnosed of primary frozen shoulder; (2) Range of surgical release is from rotator interval to 6:00 position; (3) Haven′t received manual release under anesthesia before or after arthroscopic release. Exclusion criteria: (1) intraoperative finding of other combined intra-articular injuries; (2) release range included posterior joint capsule; (3) combined with closed manipulation. A total of 26 patients met the inclusion criteria and were included in this retrospective study. Surgical methods: Surgery was performed under general anesthesia. The patient was placed at beach chair position and shoulder landmarks are marked. Arthroscopy was inserted via posterior portal into the glenohumeral joint through conventional technique, viewing small articular cavity, visible congestive synovial hyperplasia on interior walls of the joint capsule. The long head of biceps tendon was located and needle was punctured beneath from outside of the body into the joint cavity. An anterior working portal was established and radio frequency was applied to release the rotator interval. Visible thickening was seen at the joint capsule rotator interval. Arthrolysis covered leading edge of the long head tendon, coracohumeral ligament and thickened synovial tissue at the rotator interval until the edge of the subscapularis tendon could be clearly revealed, laterally rotated the shoulder joint, exposed visible thickening of the glenohumeral ligament, cut off the ligament, and cut off the anterior joint capsule and anterior glenohumeral ligament from top down along the posterior subscapularis muscles. Criteria for complete anterior joint capsule is that subscapularis muscle can be clearly seen in front of the shoulder joint. Generally, release extends downward to 5-6 o'clock position till arthroscope can pass through the glenohumeral joint smoothly. Neither the inferior nor the posterior capsule was released. Radio frequency was applied to cleanup the hyperemic and hyperplasic synovial tissue on the capsular walls and for hemostasis. Arthroscope was then moved to the subacromial space. An anterolateral working portal and a posterolateral secondary arthroscopic observation portal were established under direct vision, the subacromial space was decompressed.Coracoacromial ligament release and anterior acromioplasty were not performed. Complete hemostasis was conducted. Following routine procedure, 2 ml compound betamethasone and 3 ml lidocaine were injected into the glenohumeral joint and subacromial space, respectively. Postoperative rehabilitation: Shoulder was protected by an immobilizer for 4 weeks, passive abduction and external rotation of the shoulder was allowed in the first postoperative week. Starting from the second week, patients can perform aggressive passive stretching exercises of abduction, external rotation and adduction within a tolerable range. Patients can also perform active exercises of the shoulder within tolerable range. Capsular stretching exercises were continued since one month after operation. Anti-resistant exercises of the rotator cuff and shoulder girdle muscles were begun at 1 month after operation. Activities of daily living should be regained gradually. Follow-up indicators: Passive abduction and external rotation of the shoulder was evaluated preoperatively. Constant score, Simple Shoulder Test (SST) and VAS score were also evaluated before surgery. At the time of the last follow-up, passive range of shoulder motion,Constant score, SST score and VAS score were evaluated again.Results There were total of 26 patients in this study, among which 21 cases were followed up, accounting for a follow-up rate of 80.8%, with an average follow-up time of 31 months (29-36 months). Nine patients had concurrent diabetes, accounting for 34.6% of all 26 patients. Anterior elevation of the index shoulder was averaged in 71.3°(50°-110°) preoperatively, which was improved to an average of 158.9°(150°-170°) at the last follow-up. Preoperative average of 5.6°(0°-15°) external rotation was improved to an average of 57.5°(45°-70°) at the last follow-up. Preoperative Constant score was 34.9 points (13-71 points), and that of the contralateral shoulder was 92.8 points (57-100 points); by the time of the last follow-up, operated shoulder Constant score reached 90.4 points (81 to 100 points) while that of the contralateral shoulder was 95.6 points (80 to 100 points).Patients had a preoperative average SST score of 2.4 points (0-7 points) and contralateral shoulder average score of 11 points (4-12 points); by the time of the last follow-up, SST score of the operated shoulder was averaged in 10.1 points (8-12 points) and the contralateral side was 11.6 points (10-12 points). Preoperative VAS pain score was 7.9 points (5-9 points), which was reduced to 4 points (0-3 points) at the last follow-up.Conclusions Patients with primary frozen shoulders benefit from good functional recovery through arthroscopic release surgery after failed conservative treatment. Anterior shoulder release achieves satisfactory results.
Arthroscopy;Frozen shoulder;Arthrolysis
10.3877/cma.j.issn.2095-5790.2015.04.006
教育部創新團隊項目(IRT1201);衛生公益性行業科研專項(201002014)
100044北京大學人民醫院創傷骨科 北京大學交通醫學中心
付中國,Email:fuzhongguo@vip.sina.com
2015-10-10)