脊柱側凸患者站立位與平臥位脊柱骨盆矢狀面序列差異
2015-03-21 02:44:31李杰靜郭鴻飛張永剛唐翔宇蘇曉靜
解放軍醫學院學報 2015年6期
李杰靜,郭鴻飛,趙 陸,張永剛,宋 凱,唐翔宇,蘇曉靜
解放軍總醫院 骨科專科醫院脊柱外科,北京 100853
脊柱側凸患者站立位與平臥位脊柱骨盆矢狀面序列差異
李杰靜,郭鴻飛,趙 陸,張永剛,宋 凱,唐翔宇,蘇曉靜
解放軍總醫院 骨科專科醫院脊柱外科,北京 100853
目的比較不同體位和不同病因分型對脊柱骨盆矢狀面序列的影響。方法選取我科2010年2月- 2014年6月110例脊柱側凸患者,按病因分為特發性脊柱側凸(31例)、先天性脊柱側凸(36例)、神經肌肉型脊柱側凸(32例)、退行性脊柱側凸(11例)4組。分別行自然站立位全脊柱骨盆側位X線和平臥位低劑量三維CT重建檢查,分別測量脊柱側凸患者矢狀面平衡距離(sagittal vertical axis,SVA)、胸后凸角(Cobb T5-T12,TK)、胸腰段后凸角(Cobb T11-L2,TLK)、腰前凸角(Cobb L1-S1,LL)、骨盆入射角(pelvic incidence,PI)、骨盆傾斜角(pelvic tilt,PT)、骶骨傾斜角(sacral slope,SS),比較各組站立位與平臥位參數差異。結果從站立位到平臥位,4組TK和PT均減小(P<0.05),SS均增大(P<0.05)。退行性脊柱側凸組SVA、LL、PI和PT與其他3組差異均有統計學意義。當從站立位變換為平臥位時,退行性脊柱側凸組LL增大(P<0.05),而特發性脊柱側凸組和神經肌肉型脊柱側凸組LL均減小(P<0.05);先天性脊柱側凸組LL差異無統計學意義。結論脊柱側凸患者的站立位與平臥位的脊柱骨盆矢狀面序列存在差異。無論站立位還是平臥位,退行性脊柱側凸患者與特發性、先天性和神經肌肉型脊柱側凸患者的脊柱骨盆矢狀面序列明顯不同。
脊柱側凸;脊柱;骨盆;矢狀面序列
脊柱側凸是一種脊柱三維結構畸形疾病,包括結構性冠狀面側凸畸形、軸位椎體旋轉和矢狀面前凸的丟失。目前公認將自然站立位影像作為評價脊柱側凸的“金標準”,但臨床工作中仍會有患者攜帶平臥位X線或CT影像片前來就診,這與患者初診的醫療機構不能行站立位脊柱全長片檢查或接診醫生缺乏脊柱側凸知識有關。一些學者已經證實,冠狀面的Cobb角和軸位的椎體旋轉可能因為姿勢的改變而發生變化[1-6]。但是對于姿勢導致脊柱骨盆矢狀面參數變化的研究很少。脊柱矢狀面序列與臨床癥狀有明顯相關性[7-9]。因此,本研究比較不同姿勢和不同病因分類對脊柱骨盆矢狀面序列的影響,為沒有條件行站立位的脊柱全長片檢查的醫療機構醫生評估脊柱側凸時提供參考。
資料和方法
1 資料 回顧我科2010年2月- 2014年6月脊柱側凸(包括特發性脊柱側凸、先天性脊柱側凸、神經肌肉型脊柱側凸、退行性脊柱側凸)患者的資料,均符合脊柱側凸學會對特發性、先天性、神經肌肉型、退行性脊柱側凸的定義。本研究中神經肌肉型脊柱側凸的誘因僅是脊髓空洞,而不是肌無力、共濟失調、感覺喪失或者其他病因導致的神經肌肉型脊柱側凸。入選患者需要有完整的臨床和影像檢查資料。排除標準:肌力異常,下肢不等長,既往有脊柱或髖關節的手術史,代謝性骨病,結締組織疾病,脊柱的骨折、感染或腫瘤等病史。最終110例入選,根據病因分類將其分為特發性脊柱側凸、先天性脊柱側凸、神經肌肉型脊柱側凸、退行性脊柱側凸4組。4組脊柱側凸患者一般資料見表1。
2 影像學資料 包括手術前自然站立位全脊柱骨盆側位X線和平臥位的低劑量CT掃描重建的二維矢狀面脊柱骨盆影像。CT掃描時保持患者的髖、膝關節伸直。用Image-Pro Plus 6.0影像分析軟件測量自然站立位的影像,用西門子CT工作站測量臥位的CT影像。測量脊柱側凸患者以下幾何參數:矢狀面平衡距離(sagittal vertical axis,SVA)、胸后凸角(Cobb T5-T12,TK)、胸腰段后凸角(Cobb T11-L2,TLK)、腰前凸角(Cobb L1-S1,LL)、骨盆入射角(pelvic incidence,PI)、骨盆傾斜角(pelvic tilt,PT)、骶骨傾斜角(sacral slope,SS)。其中,頸7鉛垂線落在骶1上終板后緣前方時SVA取值為正數,在后方時取值為負數。當骶1上終板中點在髖軸連線中點后方時PT取值為正數,在前方時取值為負數。當弧度為后凸時TK、TLK、LL取值為正數,前凸時取值為負數。為了減少組間和組內差異,由2名脊柱外科醫生分別測量3次,各次測量間隔時間為2周,取6次測量的均值用于最終結果分析。
結 果
1 測量參數的可靠性 各參數ICC組內差異和組間差異均值為0.952和0.858,所有ICC值均>0.8。
2 站立位與平臥位參數比較 4組脊柱側凸患者平臥位TK較站立位均顯著減小(P=0.000,0.013, 0.000,0.002)。4組脊柱側凸患者的骨盆參數PT和SS站立位與平臥位,差異有統計學意義。從站立位到平臥位,4組脊柱側凸患者PT明顯減小,而SS明顯增大(圖1)。4組TLK和PI差異無統計學意義。見表2。
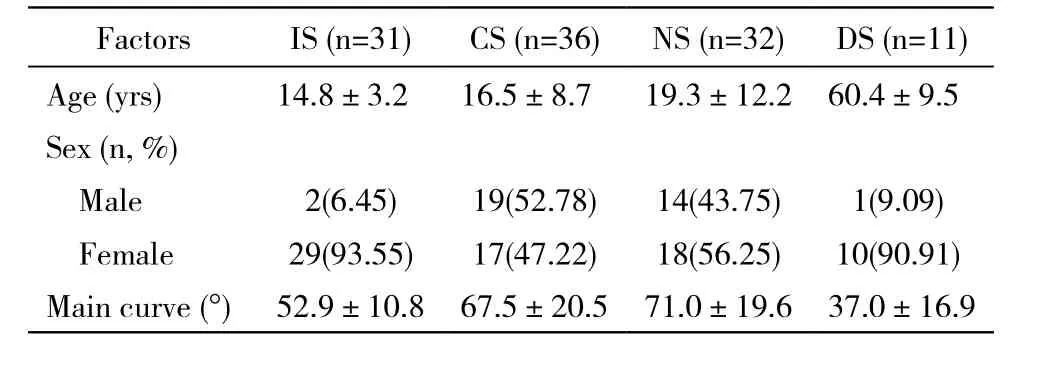
表1 特發性、先天性、神經肌肉型、退行性脊柱側凸各組的一般資料Tab. 1 General data of idiopathic, congenital,neuromuscular and degenerative scoliosis groups
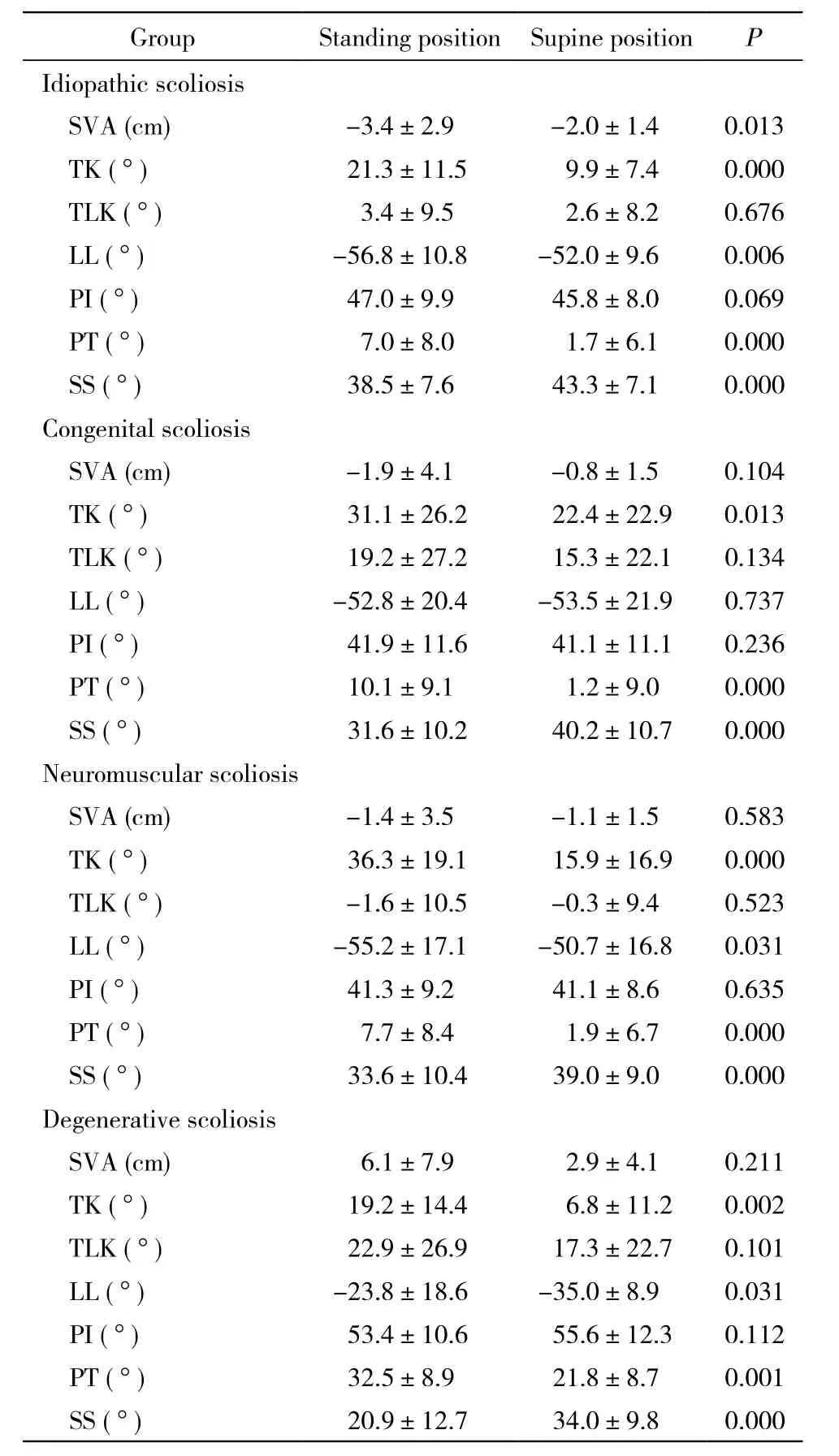
表2 4組脊柱側凸患者站立位和平臥位矢狀面脊柱骨盆參數比較Tab. 2 Comparison of standing and supine position of sagittal and pelvic parameters in four groups
3 4組間參數比較 無論站立位還是平臥位,退行性脊柱側凸組SVA、LL、PI和PT與其他3組比較,差異均有統計學意義。退行性脊柱側凸組SVA站立位和平臥位均數為正數,其他3組SVA站立位和平臥位均數為負數。退行性脊柱側凸組LL與其他3組明顯不同。從站立位到平臥位,退行性脊柱側凸組LL從-23.8°±18.6°增大至-35.0°±8.9°(P=0.031)(圖2),而特發性和神經肌肉型脊柱側凸兩組LL分別從-56.8°±10.8°、-55.2°±17.1°減小到-52.0°±9.6°、-50.7°±16.8° (P=0.006,0.031),先天性脊柱側凸組LL差異無統計學意義。見表2。
討 論
隨著研究的深入,學者們證實了脊柱骨盆矢狀面平衡的重要性[7-13]。一些學者推薦使用三維CT重建或MRI來評估脊柱側凸畸形,甚至使用CT重建或MRI影像來制訂治療方案或者評價治療效果[14-16]。許多醫療機構由于醫療條件有限,仍然使用平臥位X線來評估病情,這會影響醫生對畸形嚴重程度的判斷。學者們已經證實冠狀面Cobb角和椎體旋轉畸形由于檢查姿勢的不同而發生改變。也有報道證明,正常人群或者腰痛患者的腰椎形態,由于站立位、坐位或者平臥位等檢查姿勢的不同而發生變化[16-20]。
本研究發現,4組脊柱側凸患者站立位PT均比平臥位大,相反站立位SS均較平臥位小,且差異均有統計學意義,這一結果在之前的脊柱側凸研究中未見報道。Eddine等[21]報道了一組24名健康人的研究,得出了類似結果。他們發現當姿勢從平臥變為站立時,骨盆位置參數發生明顯變化,22名研究對象的骨盆平均后旋了7°,另外2名研究對象的骨盆平均前旋了3°。Legaye等[11]發現無論是正常人群或是側凸患者,PI與SS明顯相關,而SS又決定了LL。椎體和骨盆是通過椎間盤、小關節和肌肉軟組織連接在一起的。以上均提示從站立位到平臥位時,骨盆的旋轉使LL增大。
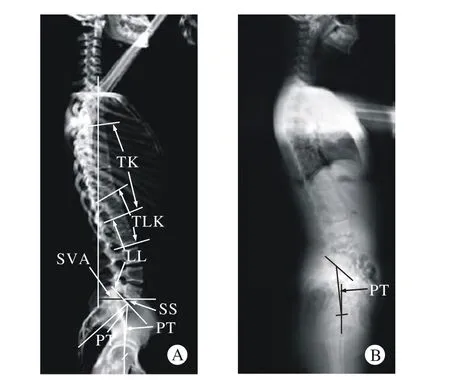
圖 1 特發性脊柱側凸患者平臥位和站立位影像的脊柱骨盆矢狀面序列比較A:特發性脊柱側凸患者術前CT掃描重建的平臥位矢狀面二維影像; B:同一患者術前自然站立位側位全長片Fig. 1 Radiographic example of a patient with idiopathic scoliosis in supine and standing position. The PT of supine position is obviously different with the PT of standing positionA: Preoperative supine sagittal two dimensional images reconstructed from CT scan using a low-dose scanning protocol; B: Preoperative natural standing sagittal plain radiographs of the same patient
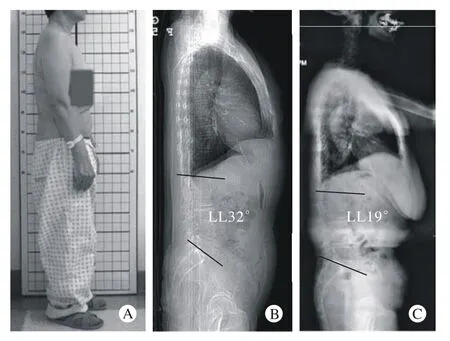
圖 2 退行性脊柱側凸患者站立側位外觀照及平臥位和站立位影像的脊柱骨盆矢狀面序列比較A:退行性脊柱側凸患者術前外院平臥位矢狀位X線提示腰前凸32°;B:該患者的側位外觀照;C:該患者術前我院站立位脊柱全長片提示19°Fig. 2 The patient’s appearance and supine lateral radiographs may confuse the doctor’s judgment of the severity of scoliosisA: The appearance of a patient with degenerative scoliosis. B: Supine lateral radiograph of this patient shows that lumbar lordosis is 32° in another hospital. C: Upright long cassette lateral radiograph of the same patient shows that lumbar lordosis is 19° in our hospital
Lee等[19]認為年輕人從站立變為平臥時,上腰椎對LL影響要比下腰椎對LL影響大,但是該研究未考慮到姿勢變換時胸椎和骶骨對LL的作用。胸腰段椎體像紐帶一樣連接著胸后凸和腰前凸,并且維系著它們之間的平衡。從站立位到平臥位,由于TK減小,胸椎的終板更接近于垂直于人體的長軸,進而導致上腰椎的前凸變小。Wood等[17]證實了站立位的腰前凸和胸腰段后凸明顯比平臥位的大。本研究同樣顯示,特發性和神經肌肉型脊柱側凸患者從站立到平臥LL明顯變小,表明特發性和神經肌肉型脊柱側凸患者,當姿勢從站立位變為平臥位時,TK減小導致LL減小的度數大于骨盆前旋導致LL增大的度數。
本研究中先天性脊柱側凸組患者大部分是楔形椎或半椎體畸形,并且這些畸形椎體多數都位于胸腰段,多數半椎體都在上下椎體間的后外側。這一結構改變可能會影響局部椎體的活動度,并且可能增加胸腰段后凸。這可能是姿勢改變時,先天性脊柱側凸組LL沒有顯著變化的原因。
許多研究已經證明腰椎退行性脊柱側凸患者的腰前凸較小。Jackson等[22]發現在成年志愿者、有癥狀的腰椎間盤退變患者、特發性或者退行性脊柱側凸患者中,如果腰前凸較小,會表現出典型的SVA很大的前傾站立姿勢。本研究中退行性脊柱側凸組也表現出LL較小、SVA較大的站立姿勢,同時骨盆后旋來保持脊柱矢狀面序列的平衡。因此站立位時退行性脊柱側凸組SS比其他3組大,而PT比其他3組小。當退行性脊柱側凸患者從站立到平臥時,脊柱會后移并且骨盆會前旋。Lee等[19]證明了當姿勢從站立到平臥時,老年人上腰椎的活動度較青年人小。因此當姿勢從站立到平臥時,骨盆前旋導致了退行性脊柱側凸患者LL的增大。
Harimaya等[23]發現,手術前腰前凸不足的成年脊柱畸形患者平臥或者術中俯臥位時,他們的腰前凸較術前站立位大,術前平臥位腰前凸與術中俯臥位腰前凸沒有顯著差異。
綜上,我們推斷脊柱側凸患者平臥位的脊柱骨盆矢狀面整體形態和平衡可能與術中俯臥位相似。鑒于收集俯臥位整體的脊柱骨盆影像資料比較困難,目前這一假設未能得到證實,還需進一步研究論證。由于X線暴露等原因,一般在脊柱側凸患者達到手術標準,需要進一步評估病情時才有針對性地對患者行脊柱CT檢查,故本研究樣本量有限,暫不能針對不同嚴重程度脊柱側凸是否會對脊柱骨盆矢狀面序列各參數產生影響進行更加深入的研究,需要在今后進一步完善。
1 Lee MC, Solomito M, Patel A. Supine magnetic resonance imaging Cobb measurements for idiopathic scoliosis are linearly related to measurements from standing plain radiographs[J]. Spine (Phila Pa 1976), 2013, 38(11): E656-E661.
2 Wessberg P, Danielson BI, Willen J. Comparison of Cobb angles in idiopathic scoliosis on standing radiographs and supine axially loaded MRI[J]. Spine (Phila Pa 1976), 2006, 31(26): 3039-3044.
3 Torell G, Nachemson A, Haderspeck-Grib K, et al. Standing and supine Cobb measures in girls with idiopathic scoliosis[J]. Spine(Phila Pa 1976), 1985, 10(5):425-427.
4 Keenan BE, Izatt MT, Askin GN, et al. Supine to standing Cobb angle change in idiopathic scoliosis: the effect of endplate preselection[J]. Scoliosis, 2014, 9:16.
5 Lee CS, Hwang CJ, Lee SW, et al. Changes of deformity due to the position and anesthesia in adolescent idiopathic scoliosis[J]. J Spinal Disord Tech, 2010, 23(6): 377-382.
6 Yazici M, Acaroglu ER, Alanay A, et al. Measurement of vertebral rotation in standing versus supine position in adolescent idiopathic scoliosis[J]. J Pediatr Orthop, 2001, 21(2): 252-256.
7 Lagrone MO, Bradford DS, Moe JH, et al. Treatment of symptomatic flatback after spinal fusion[J]. J Bone Joint Surg Am, 1988, 70(4):569-580.
8 Chaléat-Valayer E, Mac-Thiong JM, Paquet J, et al. Sagittal spino-pelvic alignment in chronic low back pain[J]. Eur Spine J,2011, 20(Suppl 5): 634-640.
9 Bernstein P, Hentschel S, Platzek I, et al. Thoracal flat back is a risk factor for lumbar disc degeneration after scoliosis surgery[J]. Spine J, 2014, 14(6): 925-932.
10 Vedantam R, Lenke LG, Keeney JA, et al. Comparison of standing sagittal spinal alignment in asymptomatic adolescents and adults[J]. Spine (Phila Pa 1976), 1998, 23(2):211-215.
11 Legaye J, Duval-Beaupère G, Hecquet J, et al. Pelvic incidence:a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves[J]. Eur Spine J, 1998, 7(2):99-103.
12 Roussouly P, Gollogly S, Berthonnaud E, et al. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position[J]. Spine (Phila Pa 1976),2005, 30(3): 346-353.
13 Glassman SD, Bridwell K, Dimar JR, et al. The impact of positive sagittal balance in adult spinal deformity[J]. Spine (Phila Pa 1976), 2005, 30(18): 2024-2029.
14 Guarino J, Tennyson S, McCain G, et al. Rapid prototyping technology for surgeries of the pediatric spine and pelvis: benefits analysis[J]. J Pediatr Orthop, 2007, 27(8):955-960.
15 Mao K, Wang Y, Xiao S, et al. Clinical application of computerdesigned polystyrene models in complex severe spinal deformities: a pilot study[J]. Eur Spine J, 2010, 19(5): 797-802.
16 Scheufler KM, Cyron D, Dohmen HA. Less invasive surgical correction of adult degenerative scoliosis, part I: technique and radiographic results[J]. Neurosurgery, 2010, 67(3): 696-710.
17 Wood KB, Kos P, Schendel M, et al. Effect of patient position on the sagittal-plane profile of the thoracolumbar spine[J]. J Spinal Disord, 1996, 9(2):165-169.
18 Mauch F, Jung C, Huth J, et al. Changes in the lumbar spine of athletes from supine to the True-Standing position in magnetic resonance imaging[J]. Spine (Phila Pa 1976), 2010, 35(9):1002-1007.
19 Lee ES, Ko CW, Suh SW, et al. The effect of age on sagittal plane profile of the lumbar spine according to standing, supine, and various sitting positions[J]. J Orthop Surg Res, 2014, 9(1): 11.
20 Dolan P, Adams MA, Hutton WC. Commonly adopted postures and their effect on the lumbar spine[J]. Spine (Phila Pa 1976), 1988,13(2): 197-201.
21 Eddine TA, Migaud H, Chantelot C, et al. Variations of pelvic anteversion in the lying and standing positions: analysis of 24 control subjects and implications for CT measurement of position of a prosthetic cup[J]. Surg Radiol Anat, 2001, 23(2):105-110.
22 Jackson RP, Peterson MD, McManus AC, et al. Compensatory spinopelvic balance over the hip axis and better reliability in measuring lordosis to the pelvic radius on standing lateral radiographs of adult volunteers and patients[J]. Spine (Phila Pa 1976), 1998,23(16):1750-1767.
23 Harimaya K, Lenke LG, Mishiro TA, et al. Increasing lumbar lordosis of adult spinal deformity patients via intraoperative prone positioning[J]. Spine (Phila Pa 1976), 2009, 34(22): 2406-2412.
Changes of sagittal spino-pelvic alignment in scoliosis patients in standing and supine position
LI Jiejing, GUO Hongfei, ZHAO Lu, ZHANG Yonggang, SONG Kai, TANG Xiangyu, SU Xiaojing
Department of Orthopedics, Chinese PLA General Hospital, Beijing 100853, China
ZHANG Yonggang. Email: zhangyg301@hotmail.com
ObjectiveTo compare the influence of different position and diverse pathogeny in patients on sagittal spino-pelvic balance.MethodsOne hundred and ten patients with scoliosis were included in this retrospective study. They were divided into four groups according to pathogeny: idiopathic scoliosis group (n=31), congenital scoliosis group (n=36), neuromuscular scoliosis group (n=32) and degenerative scoliosis group (n=11). Sagittal vertical axis (SVA), thoracic kyphosis (TK), thoracolumbar kyphosis (TLK), lumbar lordosis (LL), pelvic incidence (PI), pelvic tilt (PT), and sacral slope (SS) were measured on preoperative upright and supine lateral radiographs.ResultsThe TK and PT decreased, and SS increased when the position changed from standing to supine in the four groups (P<0.05). Compared with the other three groups, the SVA, LL, PI and PT of degenerative scoliosis group showed statistically significant difference no matter in which positions. The LL of degenerative scoliosis group increased (P<0.05) when the position changed from standing to supine. In contrast, the LL of idiopathic and neuromuscular scoliosis group decreased (P<0.05). However, the congenital scoliosis group showed no significant difference in LL.ConclusionThis study shows that the sagittal alignment of scoliosis in standing position is different with which in supine position. And neither in upright nor in supine position, the sagittal parameters of degenerative scoliosis is different with the idiopathic, congenital and neuromuscular scoliosis.
scoliosis; spine; pelvis; sagittal alignment
R 682.3
A
2095-5227(2015)06-0603-04
10.3969/j.issn.2095-5227.2015.06.022
時間:2015-03-20 10:11
http://www.cnki.net/kcms/detail/11.3275.R.20150320.1011.002.html
2015-01-22
李杰靜,男,在讀碩士,醫師。研究方向:脊柱畸形的診治。Email: 89721610@qq.com
張永剛,男,博士,主任醫師,博士生導師,解放軍總醫院骨科醫院副院長兼脊柱外科主任。Email: zhangyg301@hotmail. com