膝關(guān)節(jié)置換術(shù)術(shù)中與術(shù)后脛骨平臺假體后傾角差異分析
2015-03-21 03:27:19吳廈,蔡谞,劉璞,羅楊
解放軍醫(yī)學院學報 2015年3期
吳 廈,蔡 谞,劉 璞,羅 楊
解放軍總醫(yī)院 骨科,北京 100853
膝關(guān)節(jié)置換術(shù)術(shù)中與術(shù)后脛骨平臺假體后傾角差異分析
吳 廈,蔡 谞,劉 璞,羅 楊
解放軍總醫(yī)院 骨科,北京 100853
目的分析膝關(guān)節(jié)置換術(shù)脛骨平臺假體后傾角度在術(shù)中與術(shù)后的差異,為術(shù)中調(diào)整后傾角度提供理論依據(jù)。方法選取本院2013年6月1日- 2014年9月2日行關(guān)節(jié)置換術(shù)病例44例,按照選用假體的不同分為保留后交叉韌帶組(22例,33膝)及不保留后交叉韌帶組(22例,31膝)。分析兩組術(shù)中與術(shù)后后傾角度的差異。結(jié)果保留后交叉韌帶組術(shù)后的后傾角度比術(shù)中的后傾角度大5.73°±2.81°(P=0.00);不保留后交叉韌帶組術(shù)后的后傾角度比術(shù)中的后傾角度大1.66°±1.43°(P=0.00)。結(jié)論在保留后交叉韌帶組中,術(shù)后獲得的后傾角度大于術(shù)中測量的度數(shù),因此當術(shù)中后傾角度過小時,可不必調(diào)整。不保留后交叉韌帶組術(shù)后獲得的后傾角度與術(shù)中測得的度數(shù)差異并不大,可基本按照術(shù)中角度預測術(shù)后的后傾角度。
關(guān)節(jié)成形術(shù),置換,膝;脛骨平臺;后傾角
人工全膝關(guān)節(jié)置換術(shù)(total knee arthroplasty,TKA)旨在切除機體已損傷、無法自行修復的關(guān)節(jié)面,用人工關(guān)節(jié)部件替代損壞的關(guān)節(jié),恢復膝關(guān)節(jié)功能。可以有效地矯正畸形、緩解疼痛、增強患肢功能,維持關(guān)節(jié)穩(wěn)定性[1]。在人工關(guān)節(jié)置換術(shù)中,脛骨平臺假體后傾角度(Posterior slope angle,PSA)的選擇往往會影響到術(shù)后膝關(guān)節(jié)的屈伸功能、關(guān)節(jié)穩(wěn)定性及假體使用壽命,因此,PSA對TKA的影響逐漸得到重視[2-3]。如何準確地選擇后傾角度就成為了主刀醫(yī)生在術(shù)中要面臨的問題。本研究通過分析膝關(guān)節(jié)置換術(shù)術(shù)中與術(shù)后假體后傾角度的差異,以期指導醫(yī)生手術(shù)和判斷術(shù)后脛骨平臺后傾角度。
資料和方法
1 患者資料 本研究所有病例均為本院2013年6月1日- 2014年9月2日的住院手術(shù)病例。納入標準:1)手術(shù)均由同一位主刀醫(yī)生完成;2)均為初次膝關(guān)節(jié)置換;3)診斷均為膝關(guān)節(jié)骨性關(guān)節(jié)炎。排除標準:1)膝關(guān)節(jié)翻修術(shù);2)類風濕關(guān)節(jié)炎及其他類型關(guān)節(jié)炎。共納入44例64膝,其中應用保留后交叉韌帶(cruciate-retaining,CR)假體行膝關(guān)節(jié)置換22例,共行關(guān)節(jié)置換33膝,其中男2膝、女31膝,平均年齡63.95歲;應用不保留后交叉韌帶(posterior-stabilized,PS)假體行膝關(guān)節(jié)置換22例,共行關(guān)節(jié)置換31膝,其中男5膝、女26膝,平均年齡65.52歲。比較CR假體組及PS假體組患者基線資料,包括性別,年齡及術(shù)前KSS評分,組間基線資料無統(tǒng)計學差異。見表1。
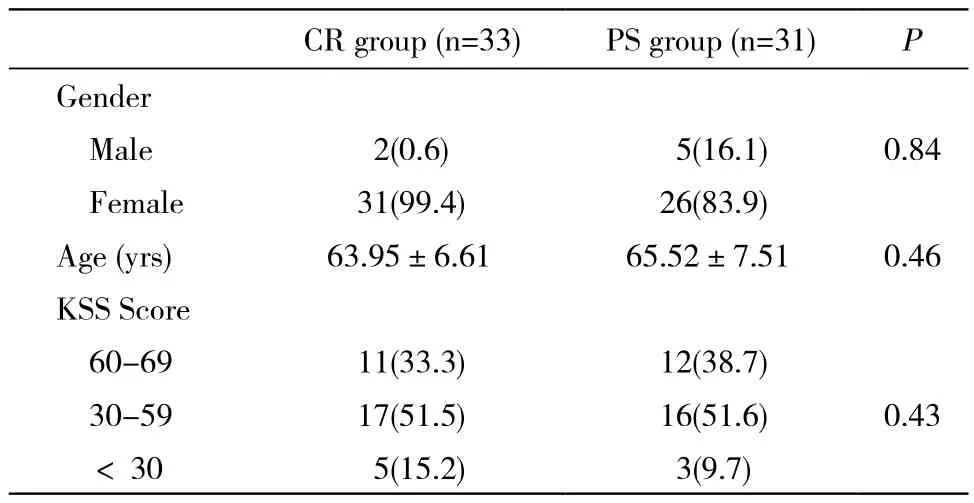
表1 兩組膝關(guān)節(jié)置換患者術(shù)前基線資料比較Tab. 1 Comparison of preoperative basic data between two TKA groups (n, %)
2 手術(shù)方法 所有病例均由同一主刀醫(yī)生完成。常規(guī)術(shù)前準備后,取膝前正中切口,長約15 cm。切開皮膚、皮下組織,切除滑膜及髕下部分脂肪墊,于脛骨結(jié)節(jié)內(nèi)側(cè)1 cm處切開骨膜,沿骨膜下銳性剝離,初步松解內(nèi)側(cè)關(guān)節(jié)囊。將髕骨外翻,屈膝關(guān)節(jié),切除股骨及脛骨骨贅,切除增生滑膜、半月板及前韌帶前止點。板鉤撬出脛骨平臺,安裝脛骨髓外定位器,于脛骨近端安裝脛骨截骨器,垂直脛骨力線沿外側(cè)平臺低點定位,為還原患者本身后傾,采用擺鋸剛好截掉脛骨平臺后方軟骨為準,并記錄術(shù)中后傾角度,股骨側(cè)采用髓外定位,截骨后分別用過氧化氫溶液及0.9%氯化鈉注射液沖洗,安裝假體。膝關(guān)節(jié)中立位依次縫合傷口。術(shù)后行膝關(guān)節(jié)側(cè)位X線測量術(shù)后脛骨平臺假體后傾角度。術(shù)中CR組采用Gemini假體(LINK公司),PS組采用RP-F假體(強生公司)。
3 后傾角度測量方法 術(shù)中后傾角度采用假體廠家配套的脛骨髓外定位器測量,以剛好截掉脛骨平臺后方軟骨為標準,固定截骨板,記錄術(shù)中后傾角度。在術(shù)前與術(shù)后膝關(guān)節(jié)X線側(cè)位片上分別測量術(shù)前與術(shù)后后傾角度,X線片選擇以無明顯脛骨旋轉(zhuǎn)及脛骨平臺輪廓清晰為準。后傾角的測量以脛骨結(jié)節(jié)下、脛骨的中上端的軸線為脛骨解剖軸,參照線垂直于該軸線,脛骨平臺前角與后角的連線與參照線的夾角記錄為術(shù)后假體的后傾角度[4-8]。見圖1。
4 分組 依據(jù)所用假體的不同分為CR組與PS組,分別記錄兩組術(shù)前、術(shù)中和術(shù)后脛骨平臺PSA。比較各組內(nèi)術(shù)前與術(shù)后PSA差異,以證實術(shù)后假體所獲得PSA是否還原到術(shù)前的解剖PSA;比較術(shù)中與術(shù)后PSA差異,以證實術(shù)后PSA與術(shù)中PSA的關(guān)系。
5 統(tǒng)計學方法 采用SPSS19.0軟件進行分析,計量資料數(shù)據(jù)均以±s表示;組間差異分析均采用t檢驗,P<0.05為差異有統(tǒng)計學意義。

圖 1 術(shù)后X線測量PS假體(左)與CR假體(右)后傾角度示意圖Fig. 1 Posterior slop angle of post-operation in PS group (left); Posterior slop angle of post-operation in CR group (right)
結(jié) 果
CR組術(shù)后PSA為9.66°±1.32°,術(shù)中PSA為3.94°±2.24°,術(shù)后比術(shù)前大5.73°±2.81°,PS組術(shù)后PSA為9.81°±1.54°,術(shù)中PSA為8.10°±1.27°,術(shù)后比術(shù)前大1.66°±1.43°,兩組術(shù)后與術(shù)中的差異均有統(tǒng)計學意義(CR組:P=0.00;PS組:P=0.00)。CR組與PS組術(shù)后假體后傾角度與術(shù)前脛骨平臺后傾角度差異無統(tǒng)計學意義(CR組:P=0.57;PS組:P=0.29),這表明兩組術(shù)后脛骨平臺后傾角度基本還原術(shù)前患者的解剖后傾角度,見圖2。
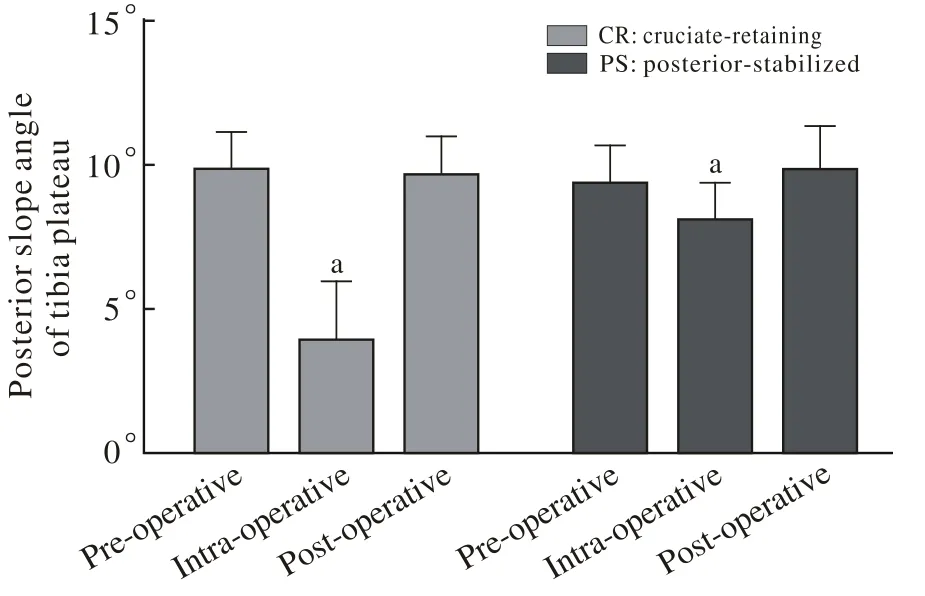
圖 2 兩組術(shù)前、術(shù)中及術(shù)后脛骨平臺后傾角度比較 (與術(shù)后相比,aP<0.05)Fig. 2 Comparison of posterior slope angle of pre- and postoperative between two groups (aP<0.05, vs post-operative)
討 論
隨著中國老齡化及骨關(guān)節(jié)炎的增多,關(guān)節(jié)置換手術(shù)在國內(nèi)進入快速發(fā)展的時期。目前膝關(guān)節(jié)置換術(shù)中力線糾正及軟組織平衡仍是手術(shù)難點之一,脛骨平臺假體的后傾角度也逐漸被臨床醫(yī)生所重視[9]。
目前多項國內(nèi)外研究報道顯示,個體間PSA差異較大,本次研究所得PSA為9.85°±1.25°。Kuwano等[10]使用CT三維重建導入計算機系統(tǒng)進行PSA測量,結(jié)果為8.1°±4.0°;Yoo等[11]使用5種不同的參考標準對脛骨側(cè)位片進行測量,平均為10.6°±3.5°;Khattak等[12]報道脛骨后傾角10°±4°;黃文華等[13]使用成人膝關(guān)節(jié)標本、干燥性脛骨標本及成人膝關(guān)節(jié)MRI測量PSA,結(jié)果為14°±3.6°;杜文延等[14]在膝關(guān)節(jié)側(cè)位片上測量的平均值11.3°±4.4°;張樹棟等[15]報道的脛骨平臺內(nèi)側(cè)后傾角為15.02°±4.2°。此外,目前關(guān)于TKA術(shù)中脛骨截骨也尚無統(tǒng)一標準。王業(yè)華等[16]認為脛骨平臺后傾角個體差異較大,應該測量術(shù)前后傾角,使脛骨后傾截骨個體化;Kansara和Markel[17]認為0°截骨和5°后傾截骨對膝關(guān)節(jié)術(shù)后的關(guān)節(jié)活動范圍無明顯影響,然而0°截骨后少數(shù)病例會出現(xiàn)前傾角,而5°后傾截骨病例則不會出現(xiàn)前傾角,故認為5°后傾截骨更安全。
另有研究證實,TKA術(shù)后當脛骨假體后傾角度處于7°~9°時,患者膝關(guān)節(jié)屈曲功能最好[18]。但是我院在行膝關(guān)節(jié)置換時,術(shù)中往往造成0°后傾已可以較完整地截去整個脛骨平臺軟骨的情況,并且術(shù)后X線測量顯示后傾角度仍在正常生理范圍之內(nèi)。面對這一尷尬局面,我們納入LINK公司的CR假體(Gemini)及強生公司的PS假體(RP-F)作研究,可以看出,無論是PS組還是CR組,術(shù)中與術(shù)后脛骨平臺后傾角的差異都有顯著統(tǒng)計學意義(CR組:P=0.00;PS組:P=0.00),這意味著術(shù)中所取后傾角度基本不能代表術(shù)后所得到的后傾角度。
就本次實驗所納入的兩款假體而言,術(shù)后假體的后傾角度都可基本還原至術(shù)前的解剖后傾角度(CR組:P=0.57;PS組:P=0.29),由此可以斷定,術(shù)中所取的實際后傾角是基本準確的,對于測量出的后傾角度偏小的情況,筆者同時分析兩款假體,主要手術(shù)步驟后初步分析認為,其主要原因:1)手術(shù)器材中脛骨段采用髓外固定,后傾角的選擇不夠直觀,造成術(shù)中后傾角選擇誤差;2)術(shù)中后傾角選擇以完全截取脛骨平臺軟骨面為標準,使主刀醫(yī)生的主觀因素影響更多,造成術(shù)中后傾角選擇誤差;3)脛骨段髓外固定的器材本身存在誤差,致使術(shù)中測得的后傾角并非實際的后傾角。
由于本院其他膝關(guān)節(jié)假體應用較少,難以達到一定程度的樣本量,所以本實驗所有病例只采用Gemini及RP-F兩款假體,雖然本研究有此局限性,但基本不影響本次研究所要達到的目標,即研究術(shù)中與術(shù)后脛骨平臺后傾角度的差異,為術(shù)中術(shù)者選取后傾角度時提供理論支持。與此同時,本實驗作為單中心前瞻性研究,還存在著樣本量較少等局限性,仍需要國內(nèi)進一步的大樣本、多中心、多假體模型的研究,為膝關(guān)節(jié)置換術(shù)中假體后傾的選擇提供強有力的理論支持。
1 孫煒.湖南(邵陽、婁底)地區(qū)人群膝關(guān)節(jié)解剖參數(shù)的測量[D].長沙:中南大學,2013.
2 Shi XJ, Shen B, Kang PD, et al. The effect of posterior tibial slope on knee flexion in posterior-stabilized total knee arthroplasty[J]. Knee Surg Sports Traumatol Arthrosc, 2013, 21(12): 2696-2703.
3 李軍,荊玨華,史占軍,等.華南人脛骨平臺后傾角的三維測量及臨床意義[J].中國臨床解剖學雜志,2013,31(4):411-413.
4 李健,吳溢峰,趙洪普,等.脛骨后傾角在膝關(guān)節(jié)置換術(shù)后的改變及意義[J].中國矯形外科雜志,2010,18(19):1588-1591.
5 Oka S, Matsumoto T, Muratsu H, et al. The influence of the tibial slope on intra-operative soft tissue balance in cruciate-retaining and posterior-stabilized total knee arthroplasty[J]. Knee Surg Sports Traumatol Arthrosc, 2014, 22(8):1812-1818.
6 韓旭東.脛骨內(nèi)側(cè)平臺后傾角放射學測量評價及其與膝骨關(guān)節(jié)炎的關(guān)系[D].廣州:廣州中醫(yī)藥大學,2011.
7 馬學東,金群華.寧夏地區(qū)回族中老年人脛骨平臺后傾角的測量評價[J].寧夏醫(yī)學雜志,2008,30(11):977-978.
8 Mohanty SS, Rao NN, Dash KK. Correlation of posterior tibial slope with metaphysio-diaphyseal angle in total knee arthroplasty: A radiological study[J]. Indian J Orthop, 2013, 47(1): 67-71.
9 Zhang Y, Wang J, Xiao J, et al. Measurement and comparison of tibial posterior slope angle in different methods based on threedimensional Reconstruction[J]. Knee, 2014, 21(3): 694-698.
10 Kuwano T, Urabe K, Miura H, et al. Importance of the lateral anatomic tibial slope as a guide to the tibial cut in total knee arthroplasty in Japanese patients[J]. J Orthop Sci, 2005, 10(1):42-47.
11 Yoo JH, Chang CB, Shin KS, et al. Anatomical references to assess the posterior tibial slope in total knee arthroplasty: a comparison of 5 anatomical axes[J]. J Arthroplasty, 2008, 23(4):586-592.
12 Khattak MJ, Umer M, Davis ET, et al. Lower-limb alignment and posterior tibial slope in Pakistanis: a radiographic study[J]. J Orthop Surg (Hong Kong), 2010, 18(1):22-25.
13 黃文華,姜楠,鐘世鎮(zhèn),等.脛骨平臺后傾角的測量及臨床意義[J].中國骨與關(guān)節(jié)損傷雜志,2007,22(10):825-828.
14 杜文延,魏福緣,衛(wèi)星,等.107例三江地區(qū)健康成人膝關(guān)節(jié)脛骨內(nèi)側(cè)平臺后傾角X線測量[J].黑龍江醫(yī)藥科學,2012,35(5):101-102.
15 張樹棟,曲廣運,張光輝,等.脛骨后傾角解剖與放射學測量評價[J].中華骨科雜志,2000(4):14-15.
16 王業(yè)華,呂厚山,寇伯龍,等.國人脛骨內(nèi)側(cè)平臺后傾角的測量及不同測量方法的比較[J].中國矯形外科雜志,2003,11(10):694-696.
17 Kansara D, Markel DC. The effect of posterior tibial slope on range of motion after total knee arthroplasty[J]. J Arthroplasty, 2006, 21(6):809-813.
18 李健,劉明廷,戚大春,等.股骨前髁偏距變化和脛骨平臺后傾角對全膝關(guān)節(jié)置換術(shù)后關(guān)節(jié)屈曲度的影響[J].濱州醫(yī)學院學報,2012,35(1):29-31.
Analysis of difference in posterior slope angle between intra-operation and post-operation of total knee arthroplasty
WU Sha, CAI Xu, LIU Pu, LUO yang
Department of Orthopedics, Chinese PLA General Hospital, Beijing 100853, China
CAI Xu. Email: caixu301@163.com
ObjectiveTo analyze the difference of posterior slope angle between intra-operation and post-operation of total knee arthroplasty (TKA) and provide a theoretical basis for adjusting the posterior slope angle.MethodsClinical data about 44 patients with TKA in Chinese PLA General Hospital from June 1 to September 2 in 2013 were collected. Patients were divided into two groups: cruciate-retaining group (n=22, 33 knees) and posterior-stabilized group (n=22, 31 knees) according to the difference of the prosthesis. The difference between posterior slope angle of intra-operation and post-operation were analyzed.ResultsIn the cruciate-retaining group, the posterior slope angle of post-operation was 5.73°±2.81° greater than that of intra-operation (P=0.00); In the posterior-stabilized group, the posterior slope angle of post-operation was 1.66°±1.43° greater than that of intra-operation (P=0.00).ConclusionIn the cruciate-retaining group, the posterior slope angle of post-operation is much smaller than that of intraoperation, which indicating that there is no need to adjust the posterior slope angle of intra-operation when it is too small. However, although there shows statistical difference of posterior slope angle between post-operation and intra-operation, the gap is not big, so we can predict the posterior slope angle of post-operation according to that of intra-operation.
arthroplasty, replacement, knee; tibia plateau; posterior slope angle
R 687.3
A
2095-5227(2015)03-0255-04
10.3969/j.issn.2095-5227.2015.03.015
時間:2014-12-19 16:29
http://www.cnki.net/kcms/detail/11.3275.R.20141219.1629.002.html
2014-09-29
吳廈,男,在讀碩士。專業(yè)方向:骨外科。Email: mike _wu0623@126.com
蔡谞,男,博士,主任醫(yī)師,碩士生導師。Email: caixu 301@163.com
猜你喜歡
音樂探索(2022年2期)2022-05-30 21:01:37
中學生數(shù)理化·八年級物理人教版(2019年9期)2019-11-25 07:33:02
小天使·一年級語數(shù)英綜合(2019年8期)2019-08-27 02:23:00
中學生數(shù)理化·八年級物理人教版(2019年3期)2019-04-25 06:20:54
中國特種設備安全(2018年11期)2019-01-08 02:08:32
小學科學(學生版)(2018年7期)2018-08-13 09:33:04
中學生數(shù)理化·八年級物理人教版(2018年3期)2018-05-31 08:52:45
數(shù)學小靈通(1-2年級)(2017年10期)2017-11-08 08:39:45
少兒科學周刊·兒童版(2016年1期)2016-03-14 03:52:21
鄭州大學學報(醫(yī)學版)(2015年2期)2015-02-27 14:50:46