可視化角膜生物力學分析儀與非接觸眼壓計和動態輪廓眼壓計測量眼內壓的一致性研究
2015-03-21 09:18:36王麗強孟曉麗牛麗麗黃一飛
解放軍醫學院學報 2015年2期
葛 梅,田 磊,王麗強,孟曉麗,王 瑛,王 敏,牛麗麗,黃一飛
解放軍總醫院 眼科近視激光中心,北京 100853
臨床研究論著
可視化角膜生物力學分析儀與非接觸眼壓計和動態輪廓眼壓計測量眼內壓的一致性研究
葛 梅,田 磊,王麗強,孟曉麗,王 瑛,王 敏,牛麗麗,黃一飛
解放軍總醫院 眼科近視激光中心,北京 100853
目的探討可視化角膜生物力學分析儀(corneal visualization scheimpflug technology,Corvis ST)測量眼內壓(intraocular pressure,IOP)的重復性,及與非接觸眼壓計(non-contact tonometr,NCT)和動態輪廓眼壓計(dynamic contour tonometry,DCT)測量結果的一致性。方法選取正常角膜志愿者91例(91眼)。分別應用Corvis ST,NCT和DCT進行眼內壓測量,每種儀器測量3次。采用單因素方差分析比較3種不同眼壓計測量的IOP結果,組內相關系數(intraclass correlation coefficient,ICC)評估3種儀器各自測量眼內壓的可重復性;Bland-Altman分析比較3種儀器測量IOP的一致性;Pearson雙變量相關分析眼壓測量結果間的相關性。結果IOPCor、IOPNCT和IOPDCT的均值分別為(13.39±2.48) mmHg (1 mmHg= 0.133 kPa),(13.94±2.32) mmHg和(17.26±2.00) mmHg,差異有統計學意義(F=76.949,P<0.001)。相關性分析顯示,3種測量儀器所測眼壓結果存在明顯相關性(P均<0.001)。IOPCor、IOPNCT和IOPDCT科隆巴赫系數(Cronbach′s α)分別為0.94、0.91和0.94;組內相關系數ICC分別為0.83、0.76和0.83。Bland-Altman一致性分析顯示,組內偏差,IOPCor與IOPNCT為(-0.5± 1.8) mmHg;IOPCor與IOPDCT為(-3.9±2.1) mmHg;IOPDCT與IOPNCT為(-3.3±2.2) mmHg,其一致性界限區間分別為(-4.1 ~3.0) mmHg、(-7.9 ~ 0.2) mmHg和(-7.6 ~ 1.0) mmHg。結論Corvis ST能夠有效測量眼內壓且測量重復性好,與NCT測量結果具有較好的一致性,但與DCT測量結果存在差異。
眼內壓;可視化角膜生物力學測量儀;非接觸眼壓計;動態輪廓眼壓計
眼內壓(intraocular pressure,IOP)是決定青光眼發生和進展程度的最重要因素,也是目前青光眼治療中唯一可控制的指標,精確地測量眼壓對于青光眼的診斷、治療和隨訪具有重要的意義[1-2]。但眼內壓的測量易受環境因素、個體因素等多種內外在因素的影響,這些因素導致了同一個體的眼壓波動。雖然Goldmann壓平眼壓測量(Goldmann applanation tonometry,GAT)是目前臨床眼壓測量的金標準[3-4]。但其測量過程需要應用表麻藥物和熒光素染色,是一種侵襲性技術,而且其測量結果與中央角膜厚度(central corneal thickness,CCT)和角膜生物力學存在密切聯系[5-7]。Ehlers等[8]報道,當CCT處于520 μm左右時,GAT的測量的精確度最佳,當CCT每偏離70 μm,GAT眼壓值偏差增加約5 mmHg (1 mmHg=0.133 kPa)。另外,動態輪廓眼壓計(dynamic contour tonometry,DCT)運用輪廓匹配理論和電子感應技術測量眼內壓,由于其測量頭弧度與角膜表面弧度相仿,因此在接觸角膜表面時并不引起角膜形變,從而杜絕角膜彈性變形力對眼內壓測量值的影響。一些研究表明,DCT的眼壓測量值不受CCT及角膜曲率的影響,能更準確地測量眼內壓[9-11]。但其患者配合要求較高,由于是接觸性測量,在角膜屈光手術后早期使用具有引起角膜瓣不穩定等缺點。基于Scheimpflug高速攝像技術研發的可視化角膜生物力學分析儀(corneal visualization scheimpflug technology,Corvis ST)已應用于臨床。該儀器能夠實時動態記錄角膜受壓形變及形態還原的整個過程,并分析角膜形變過程中的生物力學變化情況同時記錄中央水平截面角膜厚度,進一步根據角膜形變過程計算眼內壓[12]。本研究旨在探討新型眼壓測量儀Corvis ST與非接觸眼壓計(noncontact tonometry,NCT)和DCT測量正常人群眼內壓的組內重復性,以及3種設備眼壓測量結果組間的一致性,進而分析3種設備在臨床應用當中是否可以互相替代。
對象和方法
1 對象 2013年6月- 2014年3月就診于我院擬行近視激光手術的正常角膜志愿者共91例,均選取右眼為測量眼91眼。所有志愿者均經過系統的眼科檢查,包括裸眼及矯正視力檢查、主覺驗光、裂隙燈顯微鏡檢查、眼底檢查,Pentacam眼前節分析儀(Oculus,德國)測量眼前節形態參數。所有入選者均排除眼部其他疾病及外傷、手術史,
排除患有能夠影響眼部的全身系統性疾病患者,軟性角膜接觸鏡配戴者,需停戴2周以上。本實驗于2012年8月通過本院倫理委員會認證,所有志愿者均簽署了知情同意書。
2 方法 志愿者均分別應用Corvis ST (Oculus,德國),NCT (Topcon,日本)和DCT (Swiss,瑞士) 3種眼壓計測量眼內壓,測量結果分別記錄為IOPCor、IOPNCT和IOPDCT。測量順序按照志愿者就診順序,先分別應用Crovis ST和NCT測量IOP,再點表麻藥后應用DCT測量IOP,每種儀器分別測量3次,每次間隔1 ~ 2 min,不同儀器測量間隔>15 min。
3 DCT測量 志愿者取坐位,0.4%鹽酸奧布卡因滴眼液點眼行表面麻醉。DCT測量時,當測壓探頭與角膜接觸,通過裂隙燈看到“濕環”,調整“濕環”位置使之位于角膜中央,并將眼壓計測量頭端的芯片盡量置于“濕環”中央,當聽到連續而規則的蜂鳴聲5次以上后,撤離測壓頭,DCT的顯示屏上顯示此次測量的眼壓值、測量質量判定Q值和眼動脈振幅(ocular pulse amplitude,OPA)值。連續測量3次,測量數據可信度可用Q值表示,Q值≤3時結果可納入統計分析。測量結束后抗生素滴眼液點眼。
4 Corvis ST測量 無需表面麻醉,不接觸角膜。在計算機中輸入志愿者信息,志愿者取坐位,讓被檢者將下頜置于設備的下頜墊上,前額靠在前額托上,被檢者眨眼數次后睜大雙眼,注視中央固視紅點。設備正面監視攝像頭上安裝有角膜曲率計投影系統能夠聚焦和對準角膜頂點,檢查者使用自動模式控制操縱桿按屏幕提示進行瞄準和對焦,當達到第一個浦氏反射時,自動發射空氣脈沖印壓角膜形變,測量過程開始。一些表面欠規整或者透光度差的角膜,自動對焦困難,可選擇通過按操縱桿中央部測量按鈕手動測量,連續測量3次。
5 統計學方法 結果應用SPSS17.0軟件和MedCalc 13.0軟件進行統計學分析及繪圖。Kolmogorov-Smirnov檢驗測量結果是否為正態分布,正態分布數據采用-x±s表示,偏態分布數據計算中位數和變異范圍。3種不同眼壓計測量的眼內壓比較采用單因素方差分析(ANOVA),進一步兩兩比較采用最小顯著差法(LSD)。科隆巴赫系數(Cronbach′s α)和組內相關系數(intraclass correlation coefficient,ICC)評估Corvis S、NCT和DCT測量眼內壓的可重復性;Bland-Altman分析IOPCor、IOPNCT和IOPDCT之間的一致性;Pearson雙變量相關分析IOPCor、IOPNCT和IOPDCT的相關性。P<0.05為差異有統計學意義。
結 果
1 3種眼壓計測得眼內壓值比較 入選志愿者總人數為91人,其中男性41人,女性50人,平均年齡為(27.4±6.2)歲,角膜平均曲率(43.10±1.72) D,中央角膜厚度(544±26.54)μm,角膜體積(60.91± 3.35) mm3,最大壓陷深度(1.07±0.12) mm。IOPCor、IOPNCT和IOPDCT的均值和變異范圍分別為(13.39± 2.48) mmHg和(8.83 ~ 21.50) mmHg;(13.94±2.32) mmHg和(8.33 ~ 19.00) mmHg;(17.26±2.00)mmHg和(12.9 ~22.1) mmHg。ANOVA分析顯示三者之間存在明顯統計學差異(F=76.949,P<0.001)。LSD組內兩兩比較,Corvis ST測量眼壓值小于NCT、DCT測量值(P均<0.001),但IOPCor和IOPNCT組間比較無統計學差異(P=0.105)。
2 3種眼壓計測量結果的重復性 3組眼內壓測量結果中,Corvis ST和DCT組內科隆巴赫系數和組內相關系數均為0.94和0.83,好于NCT的0.91和0.76,但Corvis ST的變異系數(coefficient of variation,CV)為4.18%而DCT組為2.89%。3種設備測量眼內壓的重復性結果分析見表1。
3 3種眼壓計測量結果的相關性 Pearson雙變量相關性分析顯示,IOPCor、IOPNCT和IOPDCT間存在明顯的相關性,IOPCor與IOPNCT(r=0.72,P<0.001); IOPCor與IOPDCT(r=0.59,P<0.001);IOPNCT與IOPDCT(r=0.49,P<0.001)。見圖1。
4 3種眼壓計測量結果的一致性 Bland-Altman圖(圖2)結果顯示,三者眼內壓測量結果之間差值的均值和標準差分別為(-0.5±1.8) mmHg、(-3.9± 2.1) mmHg和(-3.3±2.2) mmHg,眼內壓的95%一致性界限(-x±1.96 s)分別為(-4.1 ~ 3.0) mmHg、(-7.9 ~0.2) mmHg和(-7.6 ~ 1.0) mmHg,其中95.6%(87/91)、93.4%(85/91)和94.5%(86/91)的點均落在一致性界限內,結果顯示Corvis ST與NCT測量眼壓方面具有較高的一致性,好于Corvis ST與DCT。
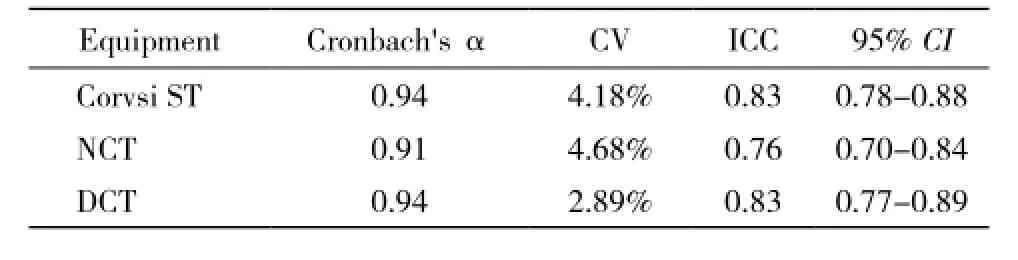
表1 Corvis ST、NCT和DCT測量眼壓組內重復性Tab. 1 Reproducibility of IOP measured by Corvis ST, NCT and DCT

圖 1 3種眼壓計測量眼壓值的相關性 A: Corvis ST和NCT; B: Corvis ST和DCT; C: DCT和NCTFig. 1 Scatter diagram of IOP measured by three tonometers A: Corvis ST and NCT; B: Corvis ST and DCT; C: DCT and NCT
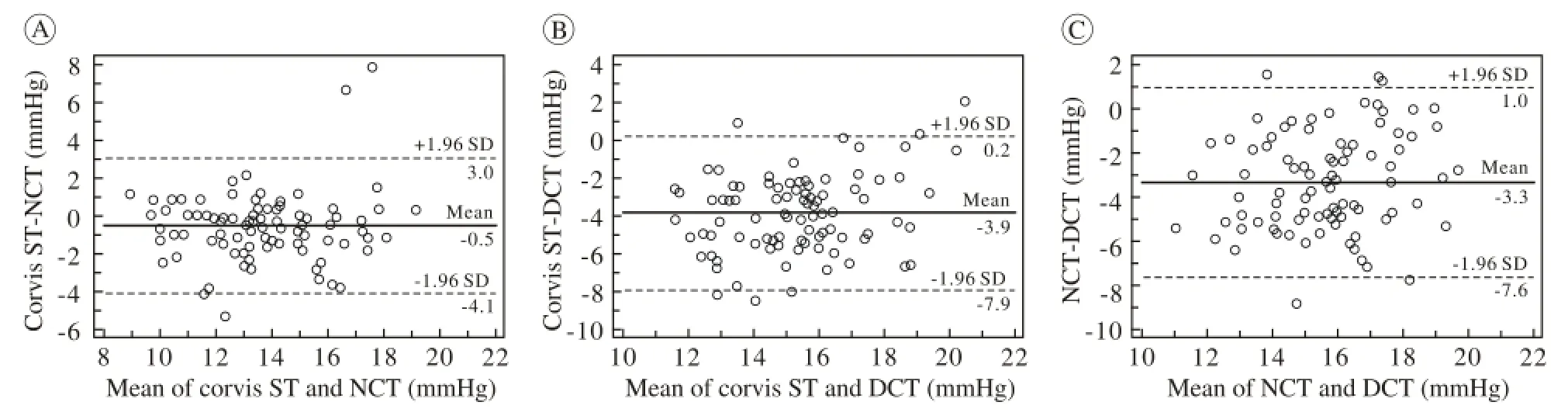
圖 2 3種眼壓計測量眼壓值Bland-Altman一致性分析 A: Corvis ST和NCT; B: Corvis ST和DCT; C: DCT和NCTFig. 2 Bland-Altman plots illustrating the reproducibility of IOP measurements A: Corvis ST and NCT; B: Corvis ST and DCT; C: DCT and NCT
討 論
目前,根據不同的設計原理,臨床上測量眼內壓的方法很多,但是沒有一種方法能夠完全排除角膜因素的影響。Corvis ST是一種新型的非接觸性的眼壓測量儀,它利用氣體脈沖印壓角膜,使角膜形變達到壓平狀態及最大壓陷狀態,Scheimpflug高速相機記錄下角膜受壓形變的全過程,通過計算機軟件分析計算眼內壓。Corvis ST是第一個能夠實現實時動態觀察眼內壓測量過程并記錄眼內壓的設備。由于該儀器尚未廣泛應用,所以相關的臨床數據有限。本文中,我們對比了新型眼壓測量儀器Corvis ST與NCT和DCT測量正常志愿者眼內壓的結果,發現Corvis ST能夠有效測量眼內壓,并且測量重復性好,其ICC=0.83,且與NCT測量結果具有較好的一致性。但其與DCT測量結果仍存在差異,Bland-Altman分析顯示IOPCor與IOPDCT的均值相差3.9 mmHg,Corvis ST眼內壓測量值小于NCT和DCT的測量值。
Ito等[13]對比分析了DCT和NCT測量眼壓結果發現,IOPDCT比IOPNCT平均高3.2 mmHg,這與我們的研究結果相符。一些研究發現,DCT測量眼壓值比GAT測量值高1 ~ 2.3 mmHg[14-15]。Kniestedt等[16]研究人尸體眼發現,GAT測量的眼壓值總比真實眼壓值小平均約4 mmHg,而DCT的測量值卻更接近真實眼內壓。本研究發現,IOPDCT的均值比IOPCor和IOPNCT分別高3.9 mmHg和3.3 mmHg。造成這種結果的原因,可能是由于IOPCor和IOPNCT與GAT一樣都是應用角膜壓平的測量原理,所以測量的眼壓值小于DCT測量值。
Hon與Lam[12]應用Corvis ST測量37名正常角膜志愿者發現,IOP組內重復性測量結果ICC=0.80。Nemeth等[17]也有相似的結論,Corvis測量參數中重復性最好的是CCT,其次是IOP,其ICC=0.865,CV=6.9%。祖培培等[18]也發現Corvis ST測量IOP的重復性Cronbach′s Alpha系數和ICC均>0.8,這與我們的結論相似。Corvis ST測量眼內壓組內的重復性較好。
Pearson雙變量相關分析顯示,IOPCor、IOPNCT與IOPDCT均有明顯的相關性(P均<0.001),IOPCor與IOPNCT及IOPDCT,IOPNCT與IOPDCT的相關系數r分別為0.72、0.59和0.49,可見IOPCor和IOPNCT的相關性最好。
本研究中IOPCor與IOPNCT的一致性好,但與IOPDCT的一致性欠佳,IOPCor的均值分別較IOPNCT與IOPDCT小0.5 mmHg和3.9 mmHg。Hong等應用Corvis ST、NCT和GAT測量23例正常志愿者和36例青光眼患者的眼內壓,發現Corvis ST測量的眼壓值比NCT小2.4 mmHg,比GAT小1.3 mmHg。分析兩研究中Corvsi ST與NCT測量差值的區別,可能為入選志愿者不同導致,Hong的研究包括青光眼患者,其IOPCor均值為21.7 mmHg,遠高于本研究正常志愿者IOPCor均值13.39 mmHg;另外非接觸眼壓計的品牌和機器使用時間不同,也可能造成系統誤差。祖培培等[18]同樣研究正常志愿者的報道中IOPCor與IOPNCT的差值為1.08 mmHg,與本研究結果相似。分析IOPCor與IOPNCT的一致性好,但與IOPDCT的一致性欠佳的原因,主要是是由于3種設備測量原理不同造成,Corvis ST與NCT均為氣沖壓平原理測量IOP,而DCT應用內置壓力感受器測量IOP,測量過程無需壓平角膜。
綜上所述,Corvis ST能夠有效測量眼內壓且測量重復性好,與NCT測量結果相關性明顯且具有較好的一致性,但與DCT測量結果仍存在差異。Corvis ST眼壓測量值較NCT和DCT測量值偏低,有可能會延誤青光眼的診斷和治療。
1 Gr?dum K, Heijl A, Bengtsson B. A comparison of glaucoma patients identified through mass screening and in routine clinical practice[J]. Acta Ophthalmol Scand, 2002, 80(6): 627-631.
2 Kass MA, Gordon MO. Intraocular pressure and visual field progression in open-angle glaucoma[J]. Am J Ophthalmol, 2000,130(4): 490-491.
3 Dielemans I, Vingerling JR, Hofman A, et al. Reliability of intraocular pressure measurement with the Goldmann applanation tonometer in epidemiological studies[J]. Graefes Arch Clin Exp Ophthalmol, 1994, 232(3):141-144.
4 Wessels IF, Oh Y. Tonometer utilization, accuracy, and calibration under field conditions[J]. Arch Ophthalmol, 1990, 108(12):1709-1712.
5 Shimmyo M, Ross AJ, Moy A, et al. Intraocular pressure, Goldmann applanation tension, corneal thickness, and corneal curvature in Caucasians, Asians, Hispanics, and African Americans[J]. Am J Ophthalmol, 2003, 136(4): 603-613.
6 Marjanovi? I, Konti? D, Hentova-Sen?ani? P, et al. Correlation between central corneal thickness and intraocular pressure in various age groups[J]. Srp Arh Celok Lek, 2010, 138(5/6): 279-286.
7 Whitacre MM, Stein R. Sources of error with use of Goldmann-type tonometers[J]. Surv Ophthalmol, 1993, 38(1): 1-30.
8 Ehlers N, Bramsen T, Sperling S. Applanation tonometry and central corneal thickness[J]. Acta Ophthalmol (Copenh), 1975, 53(1):34-43.
9 Carbonaro F, Andrew T, Mackey DA, et al. Comparison of three methods of intraocular pressure measurement and their relation to central corneal thickness[J]. Eye (Lond), 2010, 24(7): 1165-1170.
10 Sullivan-Mee M, Lewis SE, Pensyl D, et al. Factors influencing intermethod agreement between goldmann applanation, pascal dynamic contour, and ocular response analyzer tonometry[J]. J Glaucoma, 2013, 22(6): 487-495.
11 Ouyang PB, Li CY, Zhu XH, et al. Assessment of intraocular pressure measured by Reichert Ocular Response Analyzer, Goldmann Applanation Tonometry, and Dynamic Contour Tonometry in healthy individuals[J]. Int J Ophthalmol, 2012, 5(1): 102-107.
12 Hon Y, Lam AK. Corneal deformation measurement using Scheimpflug noncontact tonometry[J]. Optom Vis Sci, 2013, 90(1):e1-e8.
13 Ito K, Tawara A, Kubota T, et al. IOP measured by dynamic contour tonometry correlates with IOP measured by Goldmann applanation tonometry and non-contact tonometry in Japanese individuals[J]. J Glaucoma, 2012, 21(1): 35-40.
14 Schneider E, Grehn F. Intraocular pressure measurement-comparison of dynamic contour tonometry and goldmann applanation tonometry[J]. J Glaucoma, 2006, 15(1): 2-6.
15 Realini T, Weinreb RN, Hobbs G. Correlation of intraocular pressure measured with goldmann and dynamic contour tonometry in normal and glaucomatous eyes[J]. J Glaucoma, 2009, 18(2): 119-123.
16 Kniestedt C, Nee M, Stamper RL. Dynamic contour tonometry: a comparative study on human cadaver eyes[J]. Arch Ophthalmol,2004, 122(9): 1287-1293.
17 Nemeth G, Hassan Z, Csutak A, et al. Repeatability of ocular biomechanical data measurements with a Scheimpflug-based noncontact device on normal corneas[J]. J Refract Surg, 2013, 29(8): 558-563.
18 祖培培,王雁,左彤,等.角膜生物力學眼壓分析儀Corvis ST測量值的重復性與一致性研究[J].中華眼視光學與視覺科學雜志,2013,15(5):261-265.
Evaluation of intraocular pressure measured with Corvis ST tonometry, noncontact tonometry and dynamic contour tonometry
GE Mei, TIAN Lei, WANG Liqiang, MENG Xiaoli, WANG Ying, WANG Min, NIU Lili, HUANG Yifei
Department of Ophthalmology, Chinese PLA General Hospital, Beijing 100853, China
HUANG Yifei. Email: huangyf301@gmail.com
Objective To explore the repeatability of the Corneal Visualization Scheimpf l ug Technology (Corvis ST) for measuring intraocular pressure (IOP), and compare the results of Corvis ST with the results of noncontact tonometer (NCT) and dynamic contour tonometer (DCT). Methods Ninety-one eyes from 91 healthy subjects were included in this study. All the right eyes were chosen for IOP measurement using Corvis ST, NCT and DCT, respectively, and each measurement repeated three times. The IOP results of three different tonometers were analyzed with ANOVA, and the intraclass correlation coefficient (ICC) was used to evaluate the repeatability of these three methods; Bland-Altman was used to evaluate the consistency of IOP results, and the correlation relationship between the IOP results were analyzed by Pearson correlation analysis. Results The mean values of IOPCor, IOPNCTand IOPDCTwere (13.39±2.48) mmHg (1 mmHg=0.133 kPa), (13.94±2.32) mmHg and (17.26±2.00) mmHg, respectively. The difference were statistically signif i cant (F=76.949, P<0.001, ANOVA). Correlation analysis showed that three tonometers measured IOP results had signif i cant correlation between each other (P<0.001). The Cologne Bach coeff i cient (Cronbach's α) of IOPCor, IOPNCTand IOPDCTwere 0.94, 0.91 and 0.94, respectively; and ICC were 0.83, 0.76 and 0.83, respectively. Bland-Altman consistency analysis showed that in group IOPCorand IOPNCT, the deviation was (-0.5±1.8) mmHg, IOPCorand IOPDCTwas (-3.9±2.1) mmHg, IOPDCTand IOPNCTwas (-3.3±2.2) mmHg, the consistency limit intervals were (-4.1- 3.0) mmHg, (-7.9- 0.2) mmHg and (-7.6- 1.0) mmHg, respectively. Conclusion Corvis ST can effectively measure the IOP with good measurement repeatability. The relationship with NCT measurement results shows good consistency, but there still exist differences with DCT measurement results.
intraocular pressure; corneal visualization scheimpf l ug technology; non-contact tonometer; dynamic contour tonometer
R 770.4
A
2095-5227(2015)02-0101-05
10.3969/j.issn.2095-5227.2015.02.001
時間:2014-10-11 17:25
http://www.cnki.net/kcms/detail/11.3275.R.20141011.1725.007.html
2014-08-07
國家自然科學基金項目(81271052;31271059);國家重點基礎研究發展計劃(973計劃) (2013CB967001);香港理工大學博士監督計劃(G-UB58)
Supported by the National Natural Science Foundation of China (81271052; 31271059); National “973” Program for Basic Research of China (2013CB967001)
葛梅,女,本科,護師。研究方向:角膜屈光手術。Email: gemei_oph@163.com
黃一飛,男,博士,主任醫師,教授。Email: huangyf301@gmail.com
猜你喜歡
公民與法治(2022年5期)2022-07-29 00:47:28
教學考試(高考物理)(2021年5期)2021-11-08 10:31:22
中醫眼耳鼻喉雜志(2021年1期)2021-07-22 07:38:14
民用飛機設計與研究(2020年4期)2021-01-21 09:15:02
中學生數理化·八年級物理人教版(2019年9期)2019-11-25 07:33:02
中學生數理化·八年級物理人教版(2019年3期)2019-04-25 06:20:54
電子制作(2018年18期)2018-11-14 01:48:24
中學生數理化·八年級物理人教版(2018年3期)2018-05-31 08:52:45
山東工業技術(2016年15期)2016-12-01 05:31:22
少兒科學周刊·兒童版(2016年1期)2016-03-14 03:52:21