卡培他濱治療腫瘤引起手足綜合征的Meta分析
2013-06-12 12:31:48蒲繪華王洪源
中國醫(yī)藥指南 2013年5期
關鍵詞:效應
蒲繪華 王洪源 *
(北京大學公共衛(wèi)生學院,北京 100191)
卡培他濱治療腫瘤引起手足綜合征的Meta分析
蒲繪華 王洪源 *
(北京大學公共衛(wèi)生學院,北京 100191)
目的 對卡培他濱治療腫瘤引起手足綜合征的系統(tǒng)綜述,評估卡培他濱引起手足綜合征的發(fā)生情況。方法 根據(jù)關鍵詞檢索出文獻共 689 篇,納入 21 篇文獻進行系統(tǒng)評價。結果 針對手足綜合征,以相對危險度 LnRR 為效應指標進行系統(tǒng)評價,與對照組相比,不同給藥方案的卡培他濱引起手足綜合征的風險不同,以 RD 為分析指標與 LnRR 得到的結果相同。結論 與對照組相比,Meta 分析結果顯示卡培他濱不同給藥方案發(fā)生手足綜合征的風險不同。
卡培他濱或希羅達;手足綜合征或掌跖紅斑樣變手足皮膚反應
臨床常用的氟尿嘧啶類抗腫瘤藥物有5-氟尿嘧啶(5-FU),其通過靜脈滴注或動脈灌注給藥,常見的不良反應為胃腸道毒性和骨髓抑制及注射部位的局部刺激性[1],卡培他濱是一種口服氟尿嘧啶類藥物,主要不良反應為惡心,嘔吐,腹瀉,手足綜合征(HFS),口腔炎等,HFS雖不會危及生命,但易導致停藥或減量[2],妨礙化療正常進行,影響患者的生活質量[3]。國內外已有卡培他濱引起HFS的相關報道和防治研究,但沒有對其發(fā)生風險進行正式評估,因此進行本研究,以確定卡培他濱相關的HFS的發(fā)生情況,為臨床和科研提供參考數(shù)據(jù)。
1 資料與方法
1.1 文獻檢索
根據(jù)關鍵詞檢索PubMed數(shù)據(jù)庫[(1995~2012),檢索式:(Capecitabin OR Xeloda OR Xelodar) AND (Hand Foot Syndrome OR Palmar Plantar Erythrodysesthesia Syndrome or Hand Foot Skin Reaction),Cochrane圖書館,CNKI,CBMDisc,萬方和維普數(shù)據(jù)庫。采用1995年至2012年6月的文獻。對已檢索文獻的參考目錄進行回顧,以獲取更多文獻。
1.2 文獻篩選
納入標準:①卡培他濱單藥或聯(lián)合其他化療/靶向治療為其中一個治療組的隨機對照試驗或非隨機對照試驗,5-FU單藥或5-FU聯(lián)合其他化療為對照組,并有足夠的安全性數(shù)據(jù);②適應證為腫瘤;③數(shù)據(jù)報告包括治療組及對照組例數(shù);④給藥方案包括治療藥物,劑量及治療周期;⑤有終點觀察結果:HFS的發(fā)生例數(shù)或百分比。排除標準:①重復發(fā)表的文獻,保留總報告,排除分報告;連續(xù)發(fā)表的文獻,保留末次發(fā)表的文獻;②排除卡培他濱聯(lián)合其他氟尿嘧啶類藥物或聯(lián)合其他已證實易導致HFS的藥物(多柔比星,環(huán)磷酰胺,長春瑞濱和多西他賽)或聯(lián)合其他已證實易導致手足皮膚反應的藥物(索拉非尼和舒尼替尼)的文獻;③排除治療期間針對HFS進行干預的文獻,如涂抹尿素霜等;④排除聯(lián)合放療,免疫治療,中醫(yī)藥治療的文獻。
1.3 文獻的質量評價與資料提取
隨機對照試驗采用改良后的Jadad評價方法進行質量評估;非隨機對照試驗采用質量指數(shù)(Quality Index,又稱Downs & Black清單)進行質量評估。摘錄內容包括:給藥方案,給藥時間和腫瘤類型,受試者中位年齡,體能狀況評分,HFS發(fā)生例數(shù)或發(fā)生率。
1.4 統(tǒng)計分析
用STATA 12.0完成統(tǒng)計分析,以相對危險度(RR)為Meta分析的效應指標。①計算各研究的效應值,效應值的方差及權重;②采用DerSimonian and Laird法對效應值進行齊性檢驗;③根據(jù)齊性檢驗的結果,不存在異質性,用固定效應模型;如存在異質性,探討異質性來源:以腫瘤類型和給藥方案為指標進行亞組分析,以患者中位年齡,區(qū)域,腫瘤類型,給藥方案和治療時間為指標進行Meta回歸;如仍無法解決異質性,用隨機效應模型。④采用Begg’s test 和繪制漏斗圖的方法考察發(fā)表偏性;⑤當存在發(fā)表偏性時采用Trim and Fill法對合并效應值進行估計。
2 結 果
2.1 納入文獻概況
共檢索到689篇,初篩出41篇文獻進行全文精讀,按照入選和排除標準,排除不合格文獻14篇,最終納入meta分析的共21篇文獻,包括18項隨機對照試驗和3項非隨機對照試驗,見表1。
2.2 數(shù)據(jù)分析
2.2.1 效應值齊性檢驗
計算效應值LnRR,效應值的標準誤和權重,經(jīng)齊性檢驗,發(fā)現(xiàn)χ2=107.38,P<0.001,存在異質性。按腫瘤類型,分乳腺癌組,結直腸癌組和胃癌組,齊性檢驗結果分別為χ2=0.80,P=0.671; χ2=78.26,P<0.001;χ2=2.81,P=0.422;結直腸癌組P<0.05,仍存在異質性;按給藥方案,分為單藥和聯(lián)合方案組,結果分別為χ2=10.66,P=0.059和χ2=29.26,P=0.010;聯(lián)合方案組P<0.05,仍存在異質性。
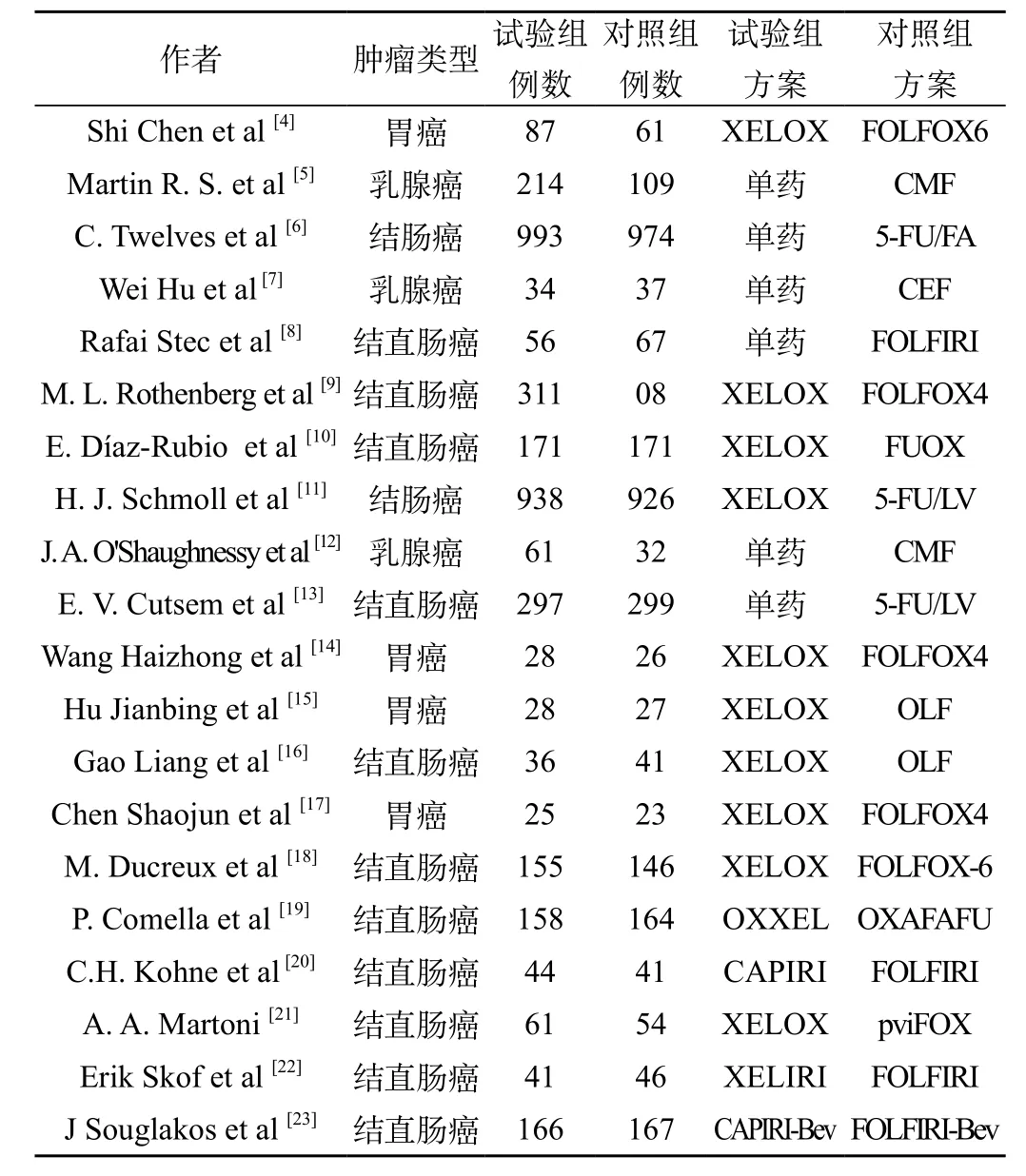
表1 納入Meta分析的文獻特征
2.2.2 合并效應值
腫瘤類型分組時方差不齊,仍存在異質性,用隨機效應模型分析。胃癌組LnRR為10.586,95% CI(4.553,24.615);結直腸癌組LnRR為3.364,95%CI(2.458,4.605);乳腺癌組LnRR為20.603,95%CI(8.660,49.015)。經(jīng)u檢驗,三組P值均<0.05,說明卡培他濱治療胃癌,結直腸癌或乳腺癌時引起HFS的發(fā)生率與對照組的差異有顯著性。
給藥方案分組時方差不齊,仍存在異質性,用隨機效應模型分析,卡培他濱聯(lián)合方案LnRR為2.949,95% CI(2.309,3.765);單藥方案LnRR為8.919,95%CI(5.542,14.353)。經(jīng)u檢驗,兩組P均<0.05,說明卡培他濱采用聯(lián)合或單藥方案引起HFS的發(fā)生率與對照組的差異有顯著性。
發(fā)表偏性檢驗,繪制漏斗圖發(fā)現(xiàn)對稱性較好,并采用Begg’s檢驗對納入的研究進行出版偏性的檢驗,Z=1.54(continuity corrected),Pr>|z|=0.124 (continuity corrected),說明收集的文獻不存在發(fā)表偏性,見圖1。
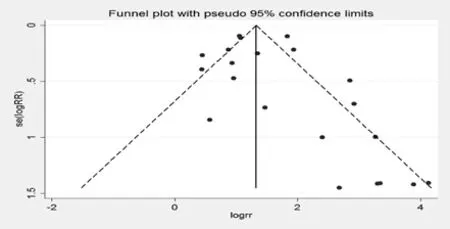
圖1 卡培他濱治療腫瘤引起手足綜合征的漏斗圖
2.2.3 Meta回歸的分析結果
以效應值LnRR為因變量,將患者中位年齡,區(qū)域,腫瘤類型,給藥方案和給藥時間拆分為啞變量進行Meta回歸,在不同患者中位年齡,不同腫瘤類型和不同給藥時間,卡培他濱治療腫瘤引起HFS的LnRR在各組之間,差異無顯著性,P值分別為:0.597,0.708和0.383,均>0.05;在不同給藥方案之間,與對照組相比較,卡培他濱引起HFS的發(fā)生風險不同(P=0.002)。
3 討 論
因卡培他濱最早于1998年上市,故檢索采用上市前3年至今的相關文獻,檢索較全面;分析評價的指標是不良反應,但不是最被關注的致命不良反應,被隱蔽的機會少。本研究僅針對中文及英文文獻,非英語及非中文文獻未收錄可能造成因收錄不全引起的結果偏倚;本研究針對腫瘤的治療涉及一線,二線,新輔助和輔助治療多種情況,腫瘤的類型也較多,各組合缺乏一定數(shù)量的原始文獻,無法進行細分;本研究從試驗所在區(qū)域進行分析,但納入的亞洲區(qū)域的文獻均來自中國,且僅有3篇,數(shù)量有限,因此不同區(qū)域對卡培他濱引起HFS的風險是否有顯著差異,有待于進一步的研究。
4 結 論
不同給藥方案發(fā)生HFS的風險不同。
[1]Chabner BA,Lynch TJ Jr,Longo DJ.HARRISON’S Manual of Oncology[M].The McGraw-Hill Companies,Inc,2008.
[2]Aru WS.The Use of Capecitabine in Cancer:Management of the Hand Foot Syndrome[J].Acta Med Indones,2005,37(3):174-176.
[3]Lassere Y,Hoff P.Management of hand-foot syndrome in patients treated with capecitabine (Xeloda)[J].Eur J Oncol Nurs,2004,8(Suppl 1):S31-S40.
[4]Chen S,Feng X,Li Y,et al.Efficacy and safety of XELOX and FOLFOX6 adjuvant chemotherapy following radical total gastrectomy[J].Oncol Lett,2012,3(4):781-786.
[5]Stockler MR,Harvey VJ,Francis PA,et al.Capecitabine versus classical cyclophosphamide, methotrexate,and fluorouracil as first-line chemotherapy for advanced breast cancer[J].J Clin Oncol,2011,29(34):4498-4504.
[6]Twelves C,Scheithauer W,McKendrick J,et al.Capecitabine versus 5-fluorouracil/folinic acid as adjuvant therapy for stage III colon cancer:final results from the X-ACT trial with analysis by age and preliminary evidence of a pharmacodynamic marker of efficacy[J].Ann Oncol,2012,23(5):1190-1197.
[7]Hu W,Shi J,Sheng Y,et al.Clinical study of adjuvant capecitabine monotherapy in Chinese elderly patients (aged 55-70) with stage IIa breast cancer[J].Onkologie,2010,33(8/9):433-436.
[8]Stec R,Bodnar L,Szczylik C.Feasibility and efficacy of capecitabine and FOLFIRI in patients aged 65 years and older with advanced colorectal cancer:a retrospective analysis[J].J Cancer Res Clin Oncol,2010,136(2):283-392.
[9]Rothenberg ML,Cox JV,Butts C,et al.Capecitabine plus oxaliplatin(XELOX) versus 5-fluorouracil/folinic acid plus oxaliplatin (FOLFOX-4) as second-line therapy in metastatic colorectal cancer:a randomized phase III noninferiority study[J]. Ann Oncol,2008,19(10):1720-1726.
[10]D íaz-Rubio E,Tabernero J,G ó mez-Espa ? a A,et al.Phase III study of capecitabine plus oxaliplatin compared with continuous-infusion fluorouracil plus oxaliplatin as firstline therapy in metastatic colorectal cancer:final report of the Spanish Cooperative Group for the Treatment of Digestive Tumors Trial[J].J Clin Oncol,2007,25(27):4224-4230.
[11]Schmoll HJ,Cartwright T,Tabernero J,et al.Phase III trial of capecitabine plus oxaliplatin as adjuvant therapy for stage III colon cancer:a planned safety analysis in 1,864 patients[J].J Clin Oncol,2007,25(1):102-109.
[12]Oshaughnessy JA,Blum J,Moiseyenko V,et al.Randomized,openlabel,phase II trial of oral capecitabine (Xeloda) vs.a reference arm of intravenous CMF(cyclophosphamide,methotrexate and 5-fluorouracil) as first-line therapy for advanced/metastatic breast cancer[J].Ann Oncol,2001,12(9):1247-1254.
[13]Van Cutsem E,Twelves C,Cassidy J,et al.Oral capecitabine compared with intravenous fluorouracil plus leucovorin in patients with metastatic colorectal cancer:results of a large phase III study[J].J Clin Oncol,2001,19(21):4097-4106.
[14]王海忠,王湘輝,呂志誠.XELOX與FOLFOX4方案治療進展期胃癌的隨機對照臨床研究[J].現(xiàn)代腫瘤醫(yī)學,2010,18(5):947-950.
[15]胡建兵,文芳,翁 潔.XELOX和OLF方 案 治療晚期胃癌的隨 機 對照臨床研究[J].中國實用醫(yī)藥,2009,4(15):25-26.
[16]高亮,王永向,盧麗琴,等.卡培他濱 聯(lián)合方案治療老年晚期結直腸癌的臨床研究[J].中國醫(yī)師進修雜志(綜合版),2008,31(8):20-23.
[17]陳 紹 俊 ,黃 海 欣 ,李 桂 生.卡 培 他 濱 與 氟 尿 嘧 啶/亞葉 酸 鈣 聯(lián) 合奧沙利鉑治療晚期胃癌的隨機對照臨床研究[J].中國癌癥雜志,2007,17(6):483-486.
[18]Ducreux1 M,Bennouna J,Hebbar M,et al.Capecitabine plus oxaliplatin (XELOX) versus 5-fluorouracil/ leucovorin plus oxaliplatin (FOLFOX-6) as first-line treatment for metastatic colorectal cancer[J].Int J Cancer,2011,128(3):682-690.
[19]Comella P,Massidda B,Filippelli G,et al.Randomised trial comparing biweekly oxaliplatin plus oral capecitabine versus oxaliplatin plus i.v. bolus Xuorouracil/ leucovorin in metastatic colorectal cancer patients:results of the Southern Italy Cooperative Oncology study 0401[J].J Cancer Res Clin Oncol,2009,135(2):217-226.
[20]Kohne CH,De Greve J,Hartmann JH,et al.Irinotecan combined with infusional 5-fluorouracil/ folinic acid or capecitabine plus celecoxib or placebo in the first-line treatment of patients with metastatic colorectal cancer.EORTC study 40015[J].Ann Oncol,2008,19(5):920-926.
[21]Martonia AA,Pinto C,Di Fabio F,et al.Capecitabine plus oxaliplatin(xelox) versus protracted 5-fluorouracil venous infusion plus oxaliplatin (pvifox) as first-line treatment in advanced colorectal cancer:A GOAM phase II randomised study (FOCA trial)[J].Eur J Cancer,2006,42(18):3161-3168.
[22]Skof E,Rebersek M,Hlebanja Z,et al.Capecitabine plus Irinotecan (XELIRI regimen) compared to 5-FU/LV plus Irinotecan (FOLFIRI regimen) as neoadjuvant treatment for patients with unresectable liver-only metastases of metastatic colorectal cancer:a randomised prospective phase II trial[J].BMC Cancer,2009,9:120.
[23]Souglakos J,Ziras N,Kakolyris S,et al.Randomised phase-II trial of CAPIRI (capecitabine, irinotecan) plus bevacizumab vs FOLFIRI (folinic acid,5-fluorouracil,irinotecan) plus bevacizumab as firstline treatment of patients with unresectable/metastatic colorectal cancer (mCRC)[J].Br J Cancer,2012,106(4):453-459.
Capecitabine-Induced Hand Foot Syndrome: A Meta-analysis
PU Hui-hua, WANG Hong-yuan (Peking University School of Public Health, Beijing 100191, China)
ObjectiveThe purpose of the study was to conduct a Meta-analysis to focus on hand-foot syndrome (HFS) for Capecitabine in treatments of cancers.MethodsA comprehensive literature search identified 689 articles published from 1995 to 2012 with key words. Total 21 eligible articles entered the meta-analysis.ResultThe risks of HFS induced by capecitabine in different treatment regimens were different.The result by RD was the’ same. Among different tumors,median ages and treatment duration,HFS induced by capecitabine was not significantly different.ConclusionCompared with controlled arm,different capecitabine containing regimens had different potential to induce HFS.
Capecitabine OR Xeloda OR Xelodar; Hand Foot Syndrome OR Palmar Plantar Erythrodysesthesia Syndrome or Hand Foot Skin Reaction
R73
:B
:1671-8194(2013)05-0031-03
*通訊作者:
猜你喜歡
核科學與工程(2021年4期)2022-01-12 06:30:26
今日農(nóng)業(yè)(2020年19期)2020-12-14 14:16:52
小學生必讀(中年級版)(2020年9期)2020-12-04 02:07:22
科學大眾(2020年17期)2020-10-27 02:49:10
紅土地(2018年11期)2018-12-19 05:10:56
意林·全彩Color(2018年9期)2018-11-13 22:49:38
中學物理·高中(2016年12期)2017-04-22 11:53:03
中國衛(wèi)生(2016年4期)2016-11-12 13:24:14
中國衛(wèi)生(2014年4期)2014-12-06 05:57:14
小櫻桃·童年閱讀(2014年11期)2014-12-01 22:21:30
