老年女性乳癌組織中Bcl-2蛋白表達及臨床意義
2024-10-17 00:00:00姜楠王欣馬萍張國芬李向利
青島大學學報(醫學版) 2024年4期
[摘要]目的探討B細胞淋巴瘤-2(Bcl-2)在老年女性乳癌組織中的表達及其與病人臨床病理特征和預后的關系。
方法采用免疫組織化學方法檢測92例老年女性乳癌組織中Bcl-2蛋白的表達,分析Bcl-2蛋白在老年女性乳癌組織中表達與病人臨床病理特征及預后的關系。
結果Bcl-2蛋白在老年女性乳癌組織中的陽性表達率為80.4%。Bcl-2的表達與腫瘤大小、淋巴結轉移、TNM分期、組織學分級和脈管瘤栓相關(χ2=4.459~11.607,P<0.05)。分子特征分析結果顯示,Bcl-2表達與病人的雌激素受體、人表皮生長因子受體-2表達和分子分型相關(χ2=14.572~19.390,P<0.05)。生存分析顯示,Bcl-2的表達與病人無進展生存率及總生存率無關(P>0.05)。
結論檢測Bcl-2蛋白的表達對于判斷老年女性乳癌預后和指導治療具有臨床參考價值。
[關鍵詞]乳腺腫瘤;老年人;基因,bcl-2;預后;免疫組織化學;病理學,臨床
[中圖分類號]R737.9;R365
[文獻標志碼]A
[文章編號]2096-5532(2024)04-0513-05doi:10.11712/jms.2096-5532.2024.60.136
[開放科學(資源服務)標識碼(OSID)]
[網絡出版]https://link.cnki.net/urlid/37.1517.R.20240927.1331.003;2024-09-2908:29:53
Expression and clinical significance of B-cell lymphoma-2 protein in breast cancer tissue of elderly female patients
JIANG Nan, WANG Xin, MA Ping, ZHANG Guofen, LI Xiangli
(Department of Thoracic Surgery, Beijing Chest Hospital, Capital Medical University, Beijing 101149, China); [Abstract]ObjectiveTo investigate the expression of B-cell lymphoma-2 (Bcl-2) in the breast cancer tissue of elderly female patients and its association with the clinicopathological features and prognosis of patients.
MethodsImmunohistochemistry was used to measure the expression of Bcl-2 protein in the breast cancer tissue samples of 92 elderly female patients, and its asso-
ciation with clinicopathological features and prognosis was analyzed.
ResultsThe positive expression rate of Bcl-2 was 80.4% in the breast cancer tissue samples of elderly female patients. The expression of Bcl-2 was associated with tumor size, lymph node metastasis, TNM stage, histological grading, and vascular tumor thrombus (χ2=4.459-11.607,P<0.05). The analysis of molecular characteristics showed that the expression of Bcl-2 was associated with estrogen receptor, Her-2, and molecular typing (χ2=14.572-19.390,P<0.05). The survival analysis showed that the expression of Bcl-2 was not associated with progression-free survival rate or overall survival rate (P>0.05).
ConclusionThe measurement of the expression of Bcl-2 protein in breast cancer tissue has a clinical reference value in predicting the prognosis of elderly female patients with breast cancer and guiding the treatment of such patients.
[Key words]breast neoplasms; aged; genes, bcl-2; prognosis; immunohistochemistry; pathology, clinical
乳癌是女性最常見的惡性腫瘤之一,已經取代肺癌成為全球第一大癌癥類型,2020年全球新增病例226萬[1]。乳癌也是我國女性最常見的癌癥類型[2-4]。隨著社會人口老齡化的加劇,老年女性乳癌病人總數日益增多[5],總體死亡率較高,老年女性乳癌已逐漸成為乳癌診療領域關注的重點。腫瘤的發生是多基因參與和協同作用的結果,多種癌基因和抑癌基因與乳癌的預后密切相關[6]。參與細胞凋亡的B細胞淋巴瘤-2(Bcl-2)基因與乳癌的發生、發展及預后密切相關[7-8]。然而,Bcl-2蛋白在老年女性乳癌組織中的研究相對較少。本研究采用免疫組織化學方法檢測Bcl-2蛋白在老年女性乳癌組織中的表達,分析其表達與病人臨床病理特征的關系及對生存預后的影響,旨在探討Bcl-2在老年女性乳癌診斷、治療及預后評估中的作用。
1材料和方法
1.1標本及其來源
選取2011年8月—2019年7月清華大學第一附屬醫院普外科收治的92例老年女性乳癌病人作為研究對象,病人年齡65~91歲,平均(72.9±6.3)
歲。研究對象一般特征見表1。所有病人均經手術切除乳房,獲取92例蠟塊組織標本,其中原位癌7例,浸潤性癌85例。納入標準:①女性,年齡≥65歲;②病理結果為乳癌;③術前未行化療、放療、內分泌治療等新輔助治療;④臨床病理資料完整;⑤隨訪資料完整;⑥未合并其他惡性腫瘤。對所有92例老年女性乳癌病人定期進行生存隨訪,生存數據主要是通過查閱住院系統電子病歷、門診系統電子病歷以及與病人和(或)其親屬的電話訪談收集的。隨訪時間24~135個月,中位隨訪時間71.5個月,隨訪時間截至2022年11月。本研究經清華大學第一附屬醫院倫理委員會審核批準且所有病人及家屬均知情同意。
1.2免疫組織化學方法檢測Bcl-2表達
采用SP法對組織切片進行染色,Bcl-2抗體購于北京中杉金橋生物技術有限公司。蠟塊切片、脫蠟、水化后,滅活內源性過氧化物酶,高壓熱抗原修復(EDTA,pH=8.0),滴加Bcl-2抗體(ZM-0010,1∶100),4 ℃孵育過夜,37 ℃孵育2 h,滴加二抗,室溫避光孵育30 min,37 ℃孵育30 min,二氨基聯苯胺(DAB)避光顯色,蘇木精復染,透明,封片。以Bcl-2陽性的扁桃體組織作為陽性對照,以磷酸鹽緩沖溶液(PBS)代替一抗作為陰性對照。
1.3免疫組織化學結果判定
Bcl-2免疫組織化學染色結果判定參照文獻標準[9]:細胞核或細胞質出現棕黃色或棕褐色顆粒為陽性。在陽性區域隨機選擇5個高倍鏡視野,對Bcl-2的陽性強度及陽性細胞比例進行評分。①染色強度評分標準:無著色0分,淺黃色1分,棕黃色2分,棕褐色3分;②陽性細胞比例評分標準:無陽性細胞為0分,陽性細胞<10%為1分,陽性細胞10%~50%為2分,陽性細胞51%~75%為3分,陽性細胞>75%為4分。染色總評分=陽性細胞比例評分×染色強度評分。染色總評分≥4分為陽性,<4分為陰性。
1.4統計學處理
采用SPSS 26.0統計軟件對數據進行統計學分析。計數資料比較采用Pearson χ2檢驗;采用Kaplan-Meier生存分析法(Log-rank檢驗)進行生存分析。以 P<0.05為差異有統計學意義。
2結果
2.1Bcl-2在老年女性乳癌組織中的表達
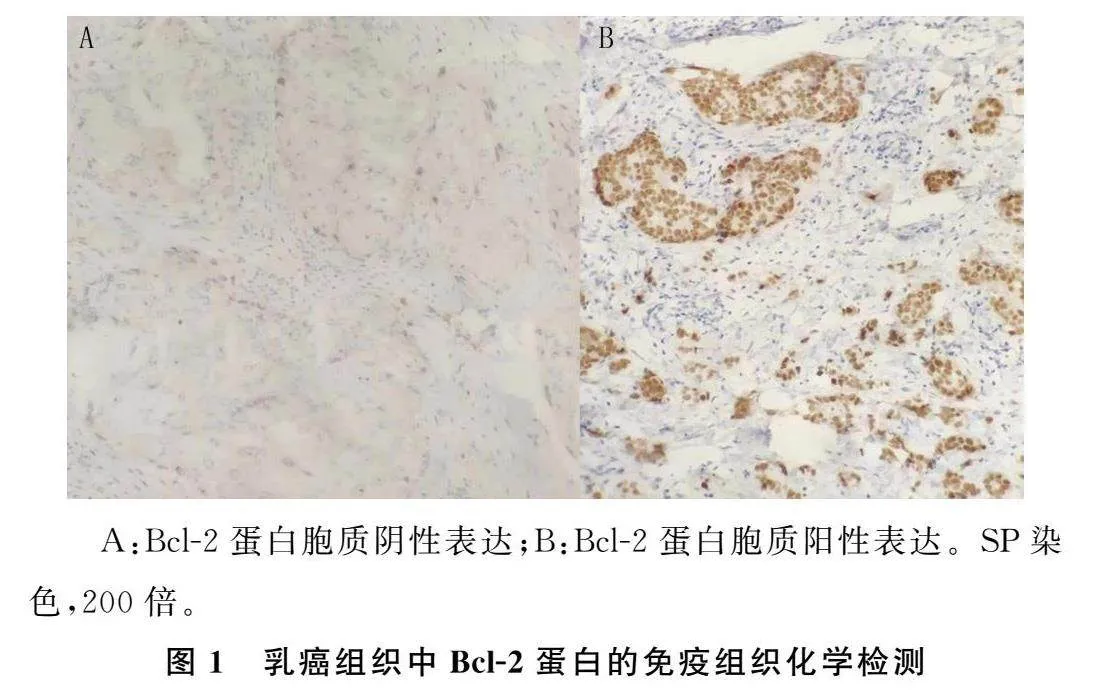
老年女性乳癌組織中Bcl-2主要表達于細胞質。 92例老年女性乳癌病人中,Bcl-2的陽性表達率為80.4%(74/92)。見圖1。
2.2Bcl-2與臨床病理特征的關系
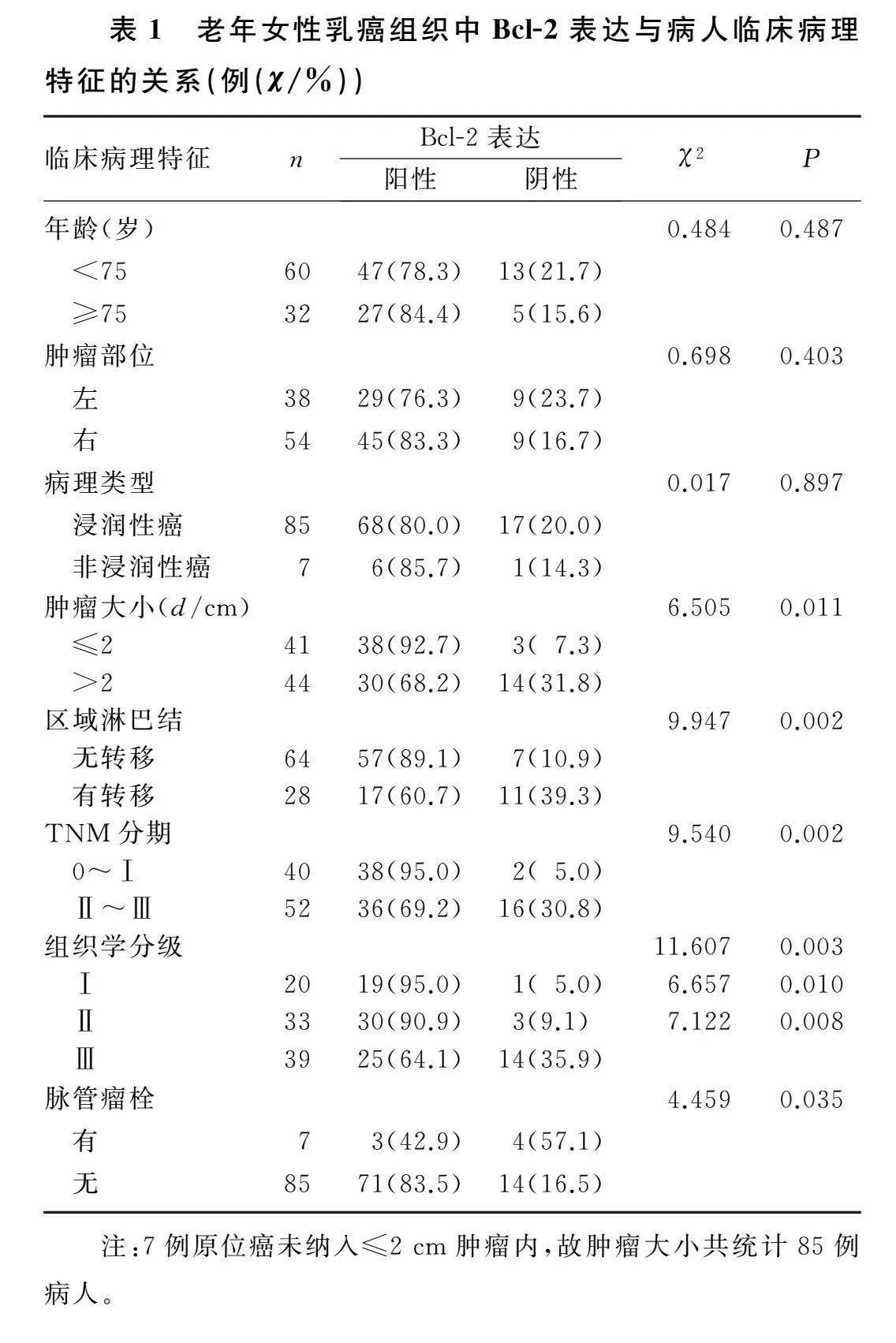
腫瘤直徑≤2 cm、無淋巴結轉移、TNM分期為0~Ⅰ期、組織學Ⅰ或Ⅱ級、無脈管瘤栓的老年女性乳癌病人癌組織中Bcl-2的表達率分別顯著高于腫瘤直徑>2 cm、有淋巴結轉移、TNM分期為Ⅱ~Ⅲ期、組織學Ⅲ級、有脈管瘤栓的病人(χ2=4.459~11.607,P<0.05),而Bcl-2表達與病人的年齡、腫瘤部位和病理類型無關(P>0.05)。見表1。
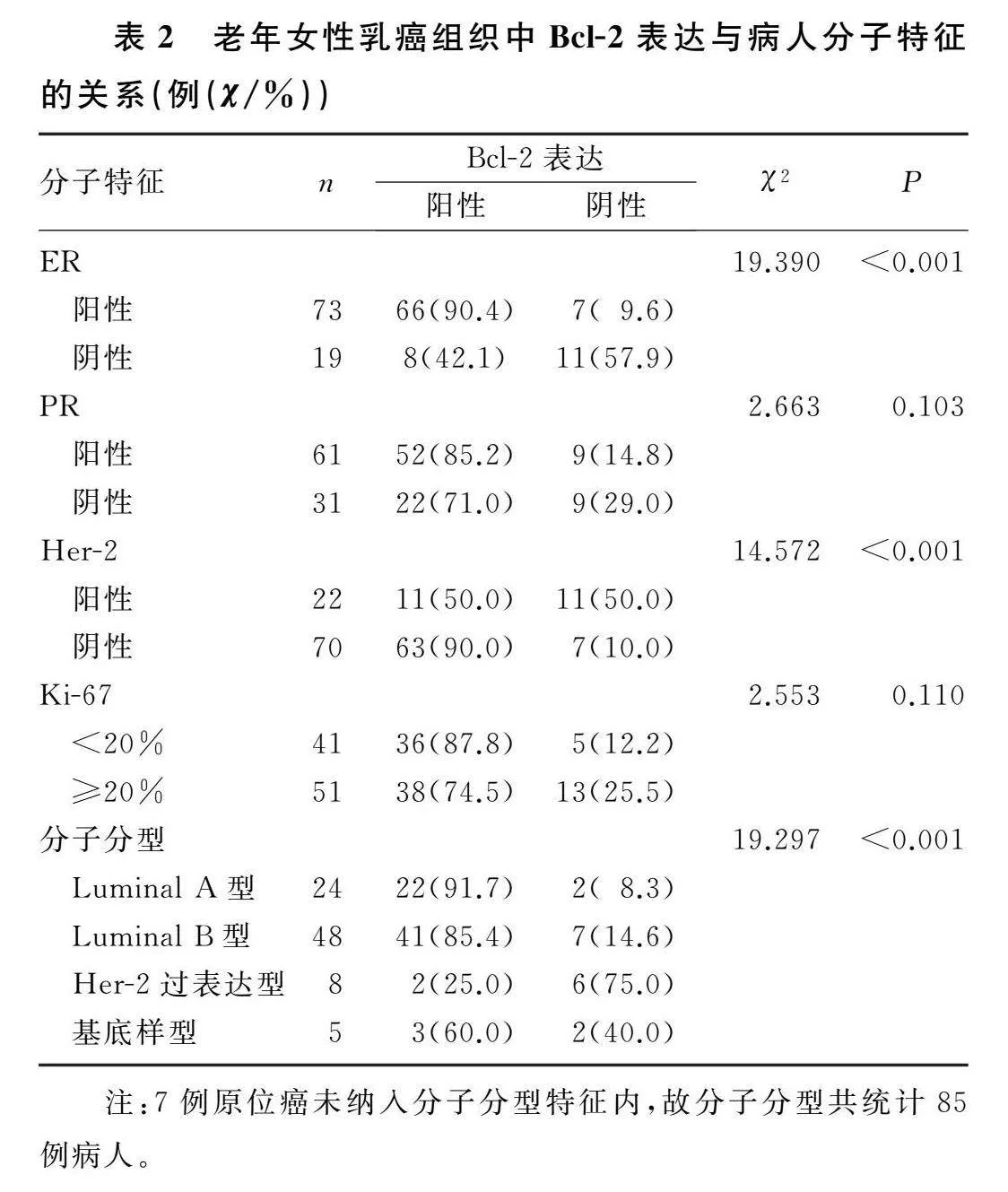
2.3Bcl-2與分子特征的關系
雌激素受體(ER)陽性、人表皮生長因子受體-2(Her-2)陰性、Luminal A型或Luminal B型的老年女性乳癌病人癌組織中Bcl-2的陽性表達率分別顯著高于ER陰性、Her-2陽性、Her-2過表達型的病人(χ2=14.572~19.390,P<0.05),而Bcl-2的表達與孕激素受體(PR)和Ki-67表達無關(P>0.05)。見表2。
2.4Bcl-2表達與老年女性乳癌病人術后生存時間的關系
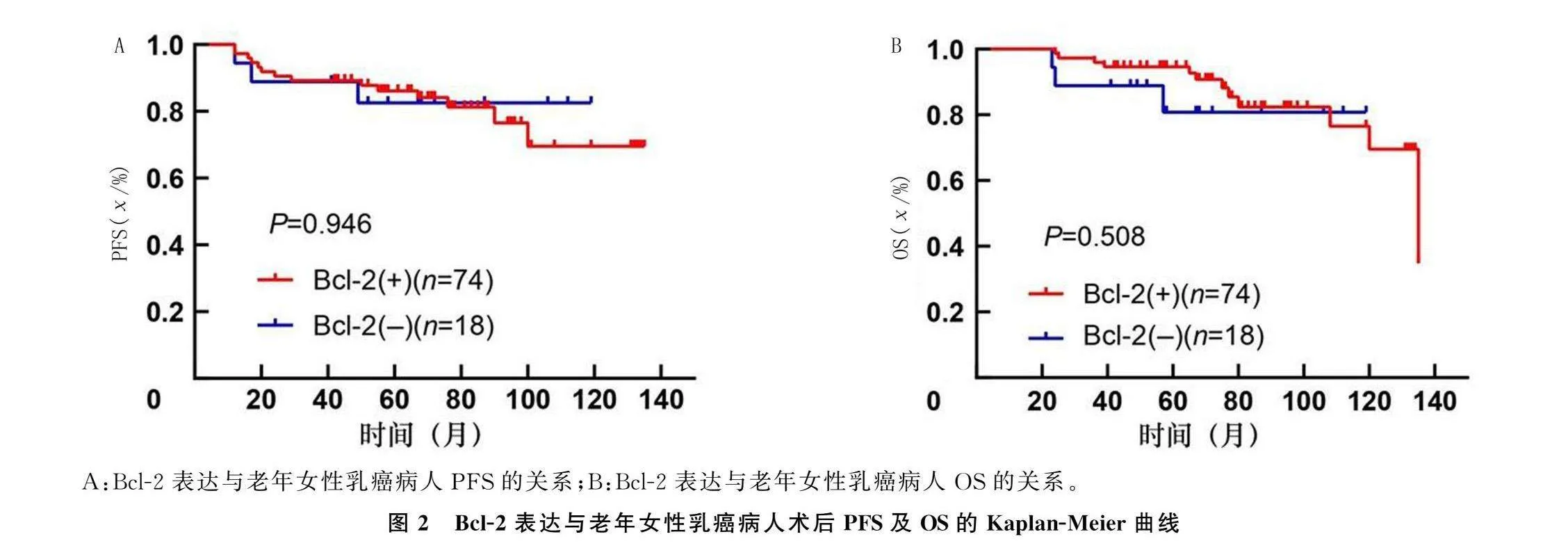
對92例老年女性乳癌病人進行生存分析,結果顯示,Bcl-2陽性組的3年無進展生存率 (PFS)為89.2%,5年PFS為86.5%,總PFS為81.1%;Bcl-2陰性組的3年PFS為88.9%,5年PFS為83.3%,總PFS為83.3%,兩組比較差異均無統計學意義(χ2=0.005,P=0.946)。見圖2A。Bcl-2陽性組的3年總生存率(OS)為95.9%,5年OS為94.6%,總OS為82.4%;Bcl-2陰性組病人的3年PFS為88.9%,5年PFS為83.3%,總PFS為83.3%,兩組比較差異無統計學意義(χ2=0.438,P=0.508)。見圖2B。
3討論
研究表明,我國老年女性乳癌的發病率呈上升趨勢,70~74歲已經成為乳癌發病年齡的第二高峰[10-11],且年齡越大,預后越差[12-13]。作為乳癌病人中的特殊群體,老年女性乳癌病人的臨床病理特征具有特殊性。乳癌是一種高度異質性腫瘤,其疾病發展是一個多基因參與、多階段演變的復雜生物學過程[14]。乳癌的發生不僅與某些原癌基因和腫瘤抑制基因的突變、缺失或激活有關,也與細胞凋亡的抑制有關[15]。Bcl-2基因是一種抗凋亡基因,其表達通過變更或移位而增強[16-18],其表達產物對多種因素誘導的細胞凋亡具有抑制作用。研究發現,參與細胞凋亡的Bcl-2基因產物在淋巴造血組織、腎癌、胃癌、乳癌及神經膠質瘤中均有表達[19],Bcl-2基因與腫瘤細胞的增殖密切相關。此外,Bcl-2也是調節細胞自噬的重要因子,其在腫瘤中過表達可減少細胞的自噬活性,并結合其抗凋亡作用維持癌細胞的生存[20-23]。理論上,Bcl-2蛋白可以抑制凋亡,減少自噬并使腫瘤細胞永生化。Bcl-2表達越強,細胞生長越快,惡性程度越高,越容易發生浸潤和轉移,預后越差。但當Bcl-2基因在乳癌中高表達時,總體結果確實與更好的病理生物學行為相關[24-28]。ZINKEL等[29]研究表明,Bcl-2基因不僅
能抑制細胞凋亡,還可以延長細胞周期,從而延緩腫瘤細胞的增殖。KE等[30]研究發現,Bcl-2高表達可以減弱乳癌細胞的擴散和遷移能力。上述研究結果可能部分解釋了為什么乳癌組織中Bcl-2的高表達與更好的病理生物學行為相關。
國內外研究發現,無區域淋巴結轉移、臨床分期較早、組織學分級較低以及腫瘤較小的腫瘤中Bcl-2高表達的比例較高[9,24,31-32]。本文研究結果顯示,Bcl-2的表達與腫瘤較大、有區域淋巴結轉移、臨床分期晚、組織學分級高、有脈管瘤栓等預后較差因素呈負相關。與國內外研究結果一致,Bcl-2在老年女性乳癌組織中的高表達與較好的臨床病理特征及預后密切相關。對Bcl-2與生存預后相關性研究顯示,Bcl-2陽性病人的PFS和OS均明顯優于Bcl-2陰性病人[9,24]。另有研究結果表明,三陰性乳癌中的Bcl-2高表達預示著病人預后不良[33]。本研究中Bcl-2陽性和陰性老年女性乳癌病人的PFS及OS均無明顯差異。這可能與樣本量較小以及老年人的治療依從性較差有關。
MELELLA等[34]研究結果表明,雌激素可以刺激乳癌細胞系MCF-7中Bcl-2的表達,提示Bcl-2蛋白在ER陽性乳癌中的表達受雌激素的調節。VAN等[31]研究發現Bcl-2在ER陽性乳癌組織中表達更高。ER在乳癌組織中的高表達提示腫瘤分化高,惡性程度低,對內分泌治療敏感等[32]。李娟等[9]和HWANG等[24]等研究發現,Bcl-2在Her-2陰性的乳癌組織中表達明顯增高。Her-2參與調控細胞生長,促進腫瘤增殖分化,其過度表達提示惡性程度高,預后不良[28]。TAWFIK等[33]和KOLA-
CINSKA等[35]研究發現,Bcl-2在Luminal A型乳癌組織中明顯高表達。本文研究結果顯示,Bcl-2蛋白在ER陽性、Her-2陰性和Luminal A型乳癌組織中均高表達,與國內外研究結果基本一致。因此,Bcl-2在老年女性乳癌組織中的高表達提示對內分泌治療敏感且預后良好。
本研究存在下列不足和缺陷:①樣本量小,研究結果可能存在一定偏差;②單中心研究有一定局限性;③入組病例時間跨度較大,治療方案存在一定差異。未來將進一步開展多中心研究,在短時間內獲得足夠的樣本,以減少上述原因造成的局限性。
綜上所述,Bcl-2蛋白與乳癌的發生發展密切相關。在老年女性乳癌中,Bcl-2高表達與更好的臨床病理特征呈正相關,預示預后更好。檢測乳癌組織中Bcl-2蛋白的表達對于判斷老年女性乳癌預后和指導治療具有臨床參考價值。
[參考文獻]
[1]SUNG H, FERLAY J, SIEGEL R L, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA: a Cancer Journal for Clinicians, 2021,71(3):209-249.
[2]CAO W, CHEN H D, YU Y W, et al. Changing profiles of cancer burden worldwide and in China: a secondary analysis of the global cancer statistics 2020[J]. Chinese Medical Journal, 2021,134(7):783-791.
[3]ZHENG R S, ZHANG S W, ZENG H M, et al. Cancer incidence and mortality in China, 2016[J]. Journal of the National Cancer Center, 2022,2(1):1-9.
[4]RAHMAT S A, HE Y T. Cancer burden and attributable risk factors of cancers in China: epidemiological insights and comparisons with India[J]. Cancer Control, 2024,31:10732748241276674.
[5]鄭榮壽,孫可欣,張思維,等. 2015年中國惡性腫瘤流行情況分析[J]. 中華腫瘤雜志, 2019,41(1):19-28.
[6]姜楠,顏承平,劉晉紅,等. 乳腺癌組織中雌孕激素受體、c-erbB-2、p53、bcl-2 及pS2 的表達及意義[J]. 中華臨床醫師雜志(電子版), 2010,4(11):2127-2130.
[7]AL-ZUBAIDY H F S, MAJEED S R, AL-KOOFEE D A F. Evaluation of Bax and BCL 2 genes polymorphisms in Iraqi women with breast cancer[J]. Archives of Razi Institute, 2022,77(2):799-808.
[8]王洋,劉偉,韓曉東,等. 乳腺癌患者病理特征與Bcl-2、CXCL13、PAX8表達情況的關系分析[J]. 檢驗醫學與臨床, 2024,21(10):1431-1435.
[9]李娟,王建成,陳小紅. 人乳頭瘤病毒感染對乳腺癌患者p53、bcl-2和c-erbB-2表達及預后的影響[J]. 中國腫瘤外科雜志, 2023,9(1):76-79.
[10]FAN L, ZHENG Y, YU K D, et al. Breast cancer in a transitional society over 18 years: trends and present status in Shanghai, China[J]. Breast Cancer Research and Treatment, 2009,117(2):409-416.
[11]WU L, CHEN G Z, ZENG Z R, et al. Analysis of breast cancer screening results and influencing factors of breast cancer in Guangdong Province from 2017 to 2021[J]. Journal of Epidemiology and Global Health, 2024,14(1):131-141.
[12]SOTO-PEREZ-DE-CELIS E, LI D N, YUAN Y, et al. Functional versus chronological age: geriatric assessments to guide decision making in older patients with cancer[J]. The Lancet Oncology, 2018,19(6):e305-e316.
[13]RUCKHBERLE E, SCHMIDT M, WELT A, et al. Palbociclib: randomized studies and real-world evidence as the basis for therapeutic planning in metastatic breast cancer[J]. Geburtshilfe und Frauenheilkunde, 2024,84(9):813-836.
[14]NARZIEYVA D F, JONIBEKOV J J, ERKINOVA S N.
Morphological features of tumor in different treatment options for patients with locally advanced breast cancer[J]. Middle European Scientific Bulletin, 2020,1(7):105-107.
[15]SUN B Q, ZHAO H W. The bioinformatics analysis of RIOX2 gene in lung adenocarcinoma and squamous cell carcinoma[J]. PLoS One, 2021,16(12):e0259447.
[16]MOLTO L, RAYMAN P, PASZKIEWICZ-KOZIK E, et al. The Bcl-2 transgene protects T cells from renal cell carcinoma-mediated apoptosis[J]. Clinical Cancer Research: an Official Journal of the American Association for Cancer Research, 2003,9(11):4060-4068.
[17]CZYSTOWSKA M, SZCZEPANSKI M J, SZAJNIK M, et al. Mechanisms of T-cell protection from death by IRX-2: a new immunotherapeutic[J]. Cancer Immunology, Immunotherapy, 2011,60(4):495-506.
[18]YU B, SUN X, SHEN H Y, et al. Expression of the apoptosis-related genes BCL-2 and BAD in human breast carcinoma and their associated relationship with chemosensitivity[J]. Journal of Experimental & Clinical Cancer Research, 2010,29(1):107.
[19]KIM R, EMI M, MATSUURA K, et al. Therapeutic potential of antisense (AS) Bcl-2 as a chemosensitizer for patients with gastric and breast carcinoma[J]. Gan to Kagaku Ryoho Cancer & Chemotherapy, 2005,32(11):1540-1545.
[20]WANG H, XU B, SHI J. N6-methyladenosine METTL3 promotes the breast cancer progression via targeting Bcl-2[J]. Gene, 2020,722: 144076.
[21]ZHANG J, ZHANG S Q, SHI Q, et al. The anti-apoptotic proteins Bcl-2 and Bcl-xL suppress Beclin 1/Atg6-mediated lethal autophagy in polyploid cells[J]. Experimental Cell Research, 2020,394(1):112112.
[22]ZHANG Y X, LIU S Y, ZHAO T S, et al. METTL3-mediated m6A modification of Bcl-2 mRNA promotes non-small cell lung cancer progression[J]. Oncology Reports, 2021,46(2):163.
[23]RAMKUMAR K, TANIMOTO A, DELLA CORTE C M, et al. Targeting BCL2 overcomes resistance and augments response to aurora kinase B inhibition by AZD2811 in small cell lung cancer[J]. Clinical Cancer Research: an Official Journal of the American Association for Cancer Research, 2023,29(16):3237-3249.
[24]HWANG K T, KIM Y A, KIM J, et al. Prognostic influences of BCL1 and BCL2 expression on disease-free survival in breast cancer[J]. Scientific Reports, 2021,11(1):11942.
[25]FABI A, MOTTOLESE M, BENEDETTO A D, et al. p53 and BLC2 immunohistochemical expression across molecular subtypes in 1099 early breast cancer patients with long-term follow-up: an observational study[J]. Clinical Breast Cancer, 2020, 20(6):e761-e770.
[26]呂德明,俎彩霞,呂凌霄. 乳腺癌PTEN、Ki-67、Bcl-2和BRCA-1蛋白表達情況及其與臨床預后的關系[J]. 中國婦幼保健, 2020,35(10):1921-1924.
[27]焦丹,劉越. p53和Bcl-2陽性表達與乳腺癌患者臨床特征的關系[J]. 癌癥進展, 2019,17(12):1445-1448.
[28]李清苗,谷國梅,師晨陽. p53及bcl-2蛋白在乳腺癌中的表達及與c-erbB-2表達的相關性[J]. 實用癌癥雜志, 2021,36(4):567-570.
[29]ZINKEL S, GROSS A, YANG E. BCL2 family in DNA da-
mage and cell cycle control[J]. Cell Death and Differentiation, 2006,13(8):1351-1359.
[30]KE H N, PARRON V I, REECE J, et al. BCL2 inhibits cell adhesion, spreading, and motility by enhancing actin polyme-
rization[J]. Cell Research, 2010,20(4):458-469.
[31]VAN NGUYEN C, NGUYEN Q T, VU H T N, et al. Combined p53 and Bcl2 immunophenotypes in prognosis of Vietnamese invasive breast carcinoma: a single institutional retrospective analysis[J]. Technol253094e09458b18b8334655e2ddda498e66be5cd9ce755a3360212511025f8dcogy in Cancer Research & Treatment, 2020,19:1533033820983081.
[32]黃信,張清,呂榮釗,等. 乳腺癌組織中蛋白 Bcl-2的表達及意義[J]. 暨南大學學報(自然科學與醫學版), 2015,36(5):421-424.
[33]TAWFIK K, KIMLER B F, DAVIS M K, et al. Prognostic significance of Bcl-2 in invasive mammary carcinomas: a comparative clinicopathologic study between “triple-negative” and non-“triple-negative” tumors[J]. Human Pathology, 2012,43(1):23-30.
[34]MILELLA M, TRISCIUOGLIO D, BRUNO T, et al. Trastuzumab down-regulates Bcl-2 expression and potentiates apoptosis induction by Bcl-2/Bcl-XL bispecific antisense oligonu-
cleotides in HER-2 gene: amplified breast cancer cells[J]. Clinical Cancer Research: an Official Journal of the American Association for Cancer Research, 2004,10(22):7747-7756.
[35]KOLACINSKA A, CHALUBINSKA J, ZAWLIK I, et al. Apoptosis-, proliferation, immune function-, and drug resis-
tance-related genes in ER positive, HER2 positive and triple negative breast cancer[J]. Neoplasma, 2012,59(4):424-432.
(本文編輯牛兆山)