“Capsule drape wrap”—a new technology for iridoschisis management during phacoemulsification
2023-06-17 06:51:36HuiChenWanChenYongBinLinWeiRongChen
Hui Chen, Wan Chen, Yong-Bin Lin, Wei-Rong Chen
State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangdong Provincial Key Laboratory of Ophthalmology and Visual Science, Guangzhou 510060, Guangdong Province, China
Abstract● AlM: To introduce a new technique for iridoschisis management during phacoemulsification: “capsule drape wrap”.
● KEYWORDS: “capsule drape wrap”technique;iridoschisis management; iris hook; phacoemulsification
INTRODUCTION
Iridoschisis is an uncommon condition of which a only few cases have been reported[1-11].This condition is characterized by separation of the anterior iris stroma from the posterior stroma and usually associated with cataract and lens subluxation[12-13].It is suggested that iridoschisis a consequence of either senile changes or blunt trauma or develops secondarily to glaucoma[14-15].
Management of iridoschisis during cataract surgery is challenging because phacoemulsification can be impeded by the degenerated iris fibrils freely floating in the anterior chamber (AC), as the tip and the irrigation-aspiration port of the phaco instrumentation are subject to the contact with the free ends[16].As a solution to facilitate the operation of phacoemulsification, the applications of iris hooks were previously described to ensure the clearance of iris fibrils from the pupillary aperture, preventing the engagement with the phaco instruments[17].However, with atrophy of the pupillary margin or glaucoma[18], iris hooks could slide from the iris during phaco.
Inspired by the ophthalmic drape for wrapping long and prominent eyelashes in anterior segment surgery, for which the drape is tightly sealing the lid margins, the eyelid speculum then allows the drape to completely wrap along the lid margin,thereby holding the eyelashes firmly under the drape (Figure 1).Accordingly, we developed a “capsule drape wrap”technique,based on the insertion of flexible nylon iris hooks to hold anterior capsule in place, consequently enabling the residual capsule to function as the drape.With the modified technique,the stability of the prolonged iris can be maintained depending on the capsular margin, and the iris fibers resulting from iridoschisis can be restricted at the periphery of the iris(Supplementary online Video 1).
SUBJECTS AND METHODS
Ethical ApprovalWe report a case of sever iridoschisis who underwent cataract surgery successfully with the modified“capsule drape wrap”technique.Written informed surgical consent was obtained from the patient.The study was approved by the Institutional Review Board of Zhongshan Ophthalmic Center (2021KYPJ082) and conducted in accordance with the tenets of the Declaration of Helsinki.

Figure 1 Diagram of ophthalmic drape for wrapping long and prominent eyelashes in anterior segment surgery.
Case ReportAn 80 year-old man presented with 6-month history of visual loss from both eyes.His clinical history excluded previous ocular trauma or inherited ocular diseases.The patient was on diabetes mellitus treatment.At the time of admission, the intraocular pressure was 11.6 (OD)/11(OS) mm Hg.His best-corrected visual acuity (BCVA) was 0.4 (logMAR) in the right eye and 0.6 (logMAR) in the left.Both ACs were remarkably shallow.In the right eye, localized splitting of the iris stroma was observed, and the free ends of the atrophic iris fibers were detected in the AC.The pupil was round, showing normal responses.Apparent nuclear sclerotic changes presented in both lenses (Figure 2).
Gonioscopy showed Shaffer grade 4 angle (270°) in both eyes.The optic disc and macula appeared to be healthy in the posterior segment examination.Visual fields were normal.Ultrabiomicroscopy showed narrow angle and marked iris convexity.A diagnosis of right idiopathic iridoschisis, bilateral narrow angles and cataract was decided.
The left eye was first treated with surgical procedures; and 1wk later, the right eye was treated.For the right eye, the surgery was operated described as follows.Six months after the surgery, the BCVA of both eyes increased by 0.1 (logMAR).
Surgical TechniqueWithin 1h before the surgery, 4 times of the pupil-dilating eyedrops were applied, and the recipe included tropicamide 1%, phenylephrine 10%, and diclofenac 0.1%.
A cohesive ophthalmic viscosurgical device (OVD) of sodium hyaluronate was applied to fill the AC, thereby holding the iris fibrils in place, enlarging the pupil and stabilizing the AC(Figure 3B).
For placing the iris hooks, the stab incisions through the peripheral cornea, which were adjacent to the site of iridoschisis, were made with 15 degree blade (Figure 3C).Epinephrine hydrochloride 1:4000 was injected intracamerally.Subsequent to the OVD injection, the continuous capsulorhexis was applied.The capsulorhexis size was controlled to be small,while the position was eccentric from the atrophic iris stroma(Figure 3D), leaving relatively wide residual capsule along the degenerated iris.
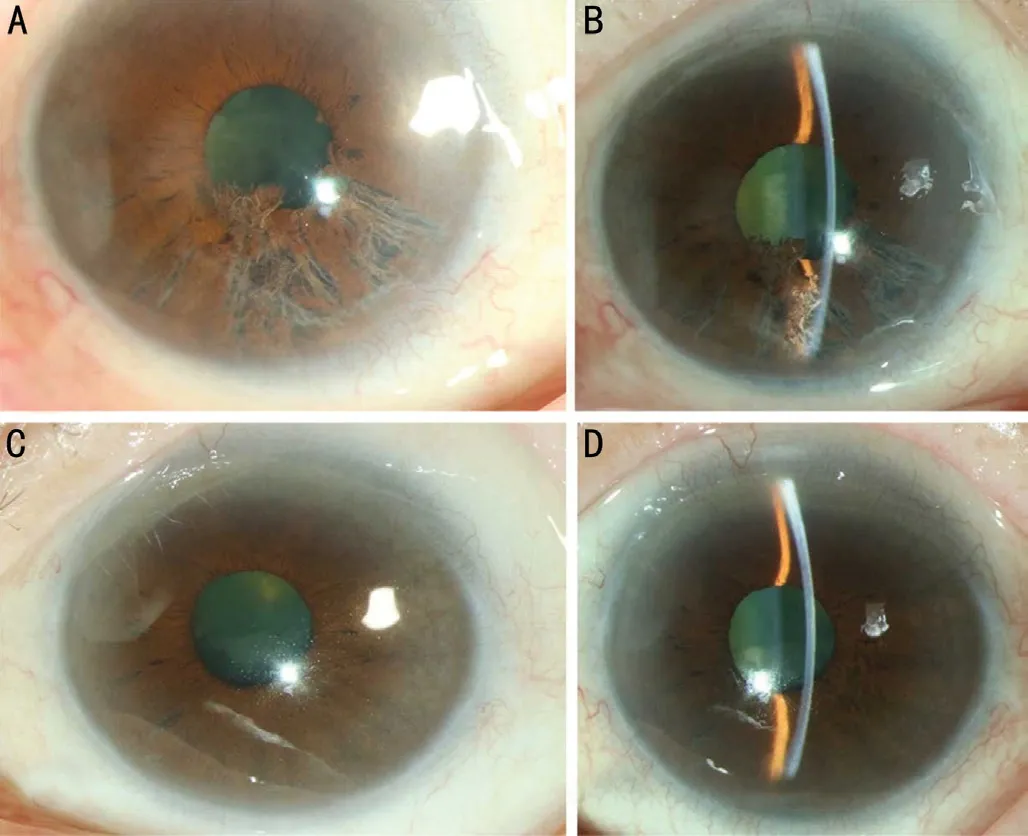
Figure 2 Slitlamp photograph A, B: The anterior segments of right eye with iridoschis; C, D: The anterior segments of left eye.
By embedding the iris hooks into the posterior chamber,the restriction on the anterior capsule was stabilized.Gentle traction was applied through the hooks to achieve pupil enlargement.Therefore, the margin of the anterior capsule could act like a drape wrap, firmly trapping the degenerate fibrillary iris strands from floating in the AC and stabilizing the capsular bags simultaneously.In another word, the iridoschisis was additionally covered by the anterior capsule.Then the stable placement of a single iris hook was secured with a silastic sleeve (Figure 3E).
The nucleus was removed using modified chopping technique.After the removal of residual cortical material, the continuous capsulorhexis was expanded to 5.3 mm if necessary, thereby allowing the implantation of an intraocular lens (IOL) into the capsular bag.Subsequently, the remnant of OVD was aspirated, followed by the removal of iris hooks and balanced salt solution was injected to hydrate and seal the corneal incision.
Before completing the surgery, careful examination was required to exclude any iris fibers trapped in the stab incisions.After the withdrawal of the iris hooks, the trapped fibers may become the entrance for the foreign materials, which was a predisposing condition for sympathetic ophthalmia.
At the end of surgery, acetylcholine was applied for pupil constriction.Finally, the eye was patched and subsequently shielded.
DISCUSSION
The pre-existing iridoschisis can increase the difficulty and risk of cataract surgery because of impaired pupil dilation and the iris fibrils which may interfere with the aspiration by phaco instruments.Therefore, additional post-operative complications may be induced by iridoschisis, for example,the sphincter muscle can be damaged, and the pigmented iris epithelium can be exposed, thereby inducing symptomatic photic phenomena[19-22].
To protect the iris, several pupil expanding devices are conducive to the surgery, including iris retractors, flexible iris hooks, and pupil expanders[16,23-26].Among of which, iris hooks is commonly available in most operating room, while many surgeons habitually use the device for inadequate pupil dilation[27-28].On the other hand, the applications of other devices are considered relatively complicated, which require extra learning processes.Nonetheless, additional precautionary measures are still advisable to optimize the safe utilization of iris hook.Even with the appropriate placement of iris hooks,some iris fiber may not be constricted.First, the disintegrated fibrils may escape the capture of the hooks, still extending into the surgical field.Second, it should be highlighted that iridoschisis has evident association with atrophic pupillary margin or glaucoma, thereby inducing the loose of iris hooks from the impaired iris[20].The engagement of the untrapped fibrils and the phaco instruments can increase the risks of hemorrhage in the arterioles and other post-operative complications.
Since the use of iris hooks can retard the movement of free fibers but may fail to provide completely fixation, inspired by ophthalmic drape for wrapping long and prominent eyelashes in anterior segment surgery, we developed a modified “capsule drape wrap”technique, which utilize flexible nylon iris hooks to capture the relatively wide residual anterior capsule instead of the iris.As a supplementary preventive procedure, a small capsulorhexis is deliberately decentered away from the site of iridoschisis.Consequently, the involvement of anterior capsule can prevent the contact between the degenerated iris stroma and the phaco instrumentation to a greater extent.Depending on the modified technique, the iris rim can be stabilized by the residual capsule, and the iris strands can be restricted at the periphery of the iris to achieve successful phacoemulsification.Ⅰn our case, consequent to the application of the modified technique, no aspiration of iris fibrils occurred.Moreover, the benefit of the novel technique also includes the extra enlargement of the pupillary aperture.Inadequate pupil dilation results in the increased difficulty of cataract surgery.The margins of anterior capsule also contribute to additional pupil dilation.Subsequently, the capsulorhexis can be enlarged and made circular before IOL implantation.
Reported less frequently, the co-existence of iridoschisis and lens subluxation have been noticed[9,13,23,29].It has been presumed that lens displacement may be a predisposing factor for iridoschisis by pushing the iris forward.There were specified phacoemulsification techniques to deal with the interference resulting from zonular weakness.The application of iris hooks was originally developed for patients with lens instability induced by pseudoexfoliation syndrome[30].Also,phacoemulsification with iris hooks to stabilize the capsular bag provides improved efficacy and safety for the removal of subluxated cataractous lenses.Depending on the proper placement and firm fixation of the iris hooks, the capsular bag is stabilized.The mutually perpendicular distribution of the paired fixation points, as well as the firmness of the hooks holding the margin of the capsulorhexis in place, constricts the free floating of the disintegrated iris fibrils.Stretching the opening of the anterior capsule also increases the resistance against any rotational movement of the bag.We suggest that the modification is a safe and relatively easy technique to trap the iris and stabilize the capsular bag simultaneous during phacoemulsification for patients with iridoschisis.
In conclusion, “capsule drape wrap”technique with flexible iris hooks can enlarge the pupil and trap the loose iris fibers,as well as stabilize the capsular bag in cases of iridoschisis.This technique is supposed to be highly applicable in clinical practice, due to the easy acquirements and handling of the required equipment, while the insertion procedures have been familiar to the experienced phaco-surgeon.It prevents further disruption to the loose iris fibers and ensures the stability of capsule–iris complex, consequently minimizing the risk of surgical complications in phacoemulsification.On the other hand, further studies with a larger group of patients and longer follow-up are required to assess the long-term safety and stability of this technique.
ACKNOWLEDGEMENTS
Foundations:Supported by the National Key R&D Program of China (No.2020YFC2008202); the National Natural Science Foundation of China (No.81970813); the Natural Science Foundation of Guangdong Province (No.2023A1515011198);Guangzhou Municipal Science and Technology Project (No.SL2022A03J00553)
Conflicts of Interest:Chen H, None; Chen W, None; Lin YB, None; Chen WR, None.
登錄APP查看全文
 International Journal of Ophthalmology
2023年6期
International Journal of Ophthalmology
2023年6期
- International Journal of Ophthalmology的其它文章
- Role of 7-methylxanthine in myopia prevention and control: a mini-review
- How internal limiting membrane peeling revolutionized macular surgery in the last three decades
- Photoreceptor changes in Leber hereditary optic neuropathy with m.G11778A mutation
- Efficacy and safety of subthreshold micropulse laser in the treatment of acute central serous chorioretinopathy
- Efficacy of ripasudil in reducing intraocular pressure and medication score for ocular hypertension with inflammation and corticosteroid
- Different serum levels of lgG and complements and recurrence rates in IgG4-positive and negative lacrimal gland benign lymphoepithelial lesion