Photoreceptor changes in Leber hereditary optic neuropathy with m.G11778A mutation
2023-06-17 06:52:20QingMeiMiaoYuFangChengHongMeiZhengJiaJiaYuanChangZhengChen
Qing-Mei Miao, Yu-Fang Cheng, Hong-Mei Zheng, Jia-Jia Yuan, Chang-Zheng Chen
Eye Center, Renmin Hospital of Wuhan University, Wuhan 430060, Hubei Province, China
Abstract● AIM: To evaluate the functional and structural changes of photoreceptors in patients and asymptomatic carriers with Leber hereditary optic neuropathy (LHON) using fullfield electroretinography (FERG) and optical coherence tomography (OCT).
● KEYWORDS: Leber hereditary optic neuropathy;asymptomatic carriers; photoreceptor; electroretinogram;mitochondrial dysfunction
INTRODUCTION
Leber hereditary optic neuropathy (LHON) is a primary inherited mitochondrial disease arising from mitochondrial DNA mutations[1].Over 95% of LHON cases are caused by three primary point mutations, m.11778G>A,m.3460G>A and m.14484T>C[2].Mutations result in the dysfunction of the mitochondrial respiratory chain complex subunit I[3].Retinal ganglion cells (RGCs) are rich in mitochondria and are most prone to mitochondrial dysfunction,eventually leading to RGC degeneration and necrosis and optic nerve atrophy[4].Most LHON patients are male, and LHON typically manifests as acute or subacute painless central visual loss in both eyes simultaneously or successively.Approximately 50% of male carriers and 90% of female carriers do not develop visual loss in their lifetime, referred to as asymptomatic carriers[5].
Photoreceptors are also densely packed with mitochondria.However, previous studies have shown that photoreceptors function and morphology are usually not affected in LHON patients[6-7].To date, most studies on LHON have focused on RGCs; little attention has been paid to the changes in photoreceptors.Some studies have revealed a decreased amplitude in the full-field electroretinography (FERG) or abnormal photoreceptors thickness on optical coherence tomography(OCT) in LHON patients, indicating abnormal photoreceptors function or structure[8-11].Notwithstanding, these studies did not deeply address the characteristics and mechanisms of photoreceptors dysfunction and abnormal morphology.
In this study, we analyzed the FERG and OCT manifestations of LHON-affected patients and asymptomatic carriers to explore the characteristics of photoreceptors impairment.
SUBJECTS AND METHODS
Ethical ApprovalThis study was approved by the Clinical Research Ethics Committee of the Renmin Hospital of Wuhan University (No.WDRY2021-K018) and followed the tenets of the Declaration of Helsinki.All participants provided written informed consent.

Table 1 Demographic data

Table 2 Comparison of FERG results of patients and asymptomatic carriers with normal reference values μV, mean±SD
ParticipantsLHON-affected patients with the m.G11778A mutation were invited to participate in this cross-sectional study at the Renmin Hospital of Wuhan University, which was conducted between March 2022 and August 2022.The inclusion criteria were as follows: 1) bilateral painless visual loss with central or paracentral scotoma; 2) an m.11778G>A mutation confirmed by genetic testing; 3) no other optic nerverelated or serious fundus diseases.Family members of these patients were included as asymptomatic carriers (i.e., those carrying the m.11778G>A mutation).Normal subjects were recruited from the First Clinical College of Wuhan University.The inclusion criteria were as follows: 1) best corrected visual acuity (BCVA) of 1.0 in both eyes (0.0 logMAR); 2) refractive error <±6 D; 3) intraocular pressure <21 mm Hg; 4) no ocular diseases.
Full-Field Electroretinography RecordingFERG was recorded using the GOTEC visual electrophysiology instrument (GT-2008V-IV, Chungking, China) according to the standard protocol of the International Society for Clinical Electrophysiology of Vision[12].The amplitudes of the a-wave induced in response to dark-adapted 0.01 electroretinography,dark-adapted 3.0 electroretinography, light-adapted 3.0 electroretinography and light-adapted 30 Hz flicker electroretinography were recorded, followed by the photopic negative response (PhNR), defined as the first negative wave after the b-wave[13].The a-wave and PhNR amplitudes were recorded from the trough to the baseline.The reference value was determined according to the normal value obtained by the laboratory.
Optical Coherence Tomography RecordingThe macula and optic disc were imaged by Spectralis HRA-OCT (Heidelberg Engineering, Heidelberg, Germany).The macula was imaged by a horizontal B-scan through the fovea, and the optic disc was imaged by a 3.4 mm diameter circular scan.A real-time automatic tracking function was adopted, the images were superimposed 100 times, and images with a signal strength>20 were retained.Automated segmentation and thickness analyses of the peripapillary retinal nerve fiber layer (pRNFL)were performed using built-in software.The thicknesses of the pRNFL in the nasal, superior, temporal, inferior and average quadrants were recorded.The macular images were exported to Image J software (version 1.53 k, National Institutes of Health,USA).The outer nuclear layer (ONL) and photoreceptor inner and outer segment (IS/OS) were manually segmented.The ONL and IS/OS thicknesses of the fovea, nasal parafovea and temporal parafovea (1500 μm away from the fovea) were measured.The total photoreceptors thickness was calculated as the sum of the ONL and IS/OS thicknesses.
Statistical AnalysisStatistical analyses were performed using SPSS software (version 25.0, SPSS Inc., Chicago,Illinois, USA).Measurement data are expressed as the mean±standard deviation (SD).One-way analysis of variance(ANOVA) ort-test was used for group comparisons, and pairwise comparisons were performed with the least significant difference test.P<0.05 was considered statistically significant.
RESULTS
Demographic DataDemographic data are shown in Table 1.A total of 14 LHON-affected patients (11 males; mean age:20.00±9.37y; mean BCVA: 1.81±0.56 logMAR; mean disease duration: 26.71±21.34mo), 12 asymptomatic carriers (12 females; mean age: 39.83±6.48y), and 15 normal subjects (12 males; mean age: 24.20±1.52y) were included in the study.There was no statistically significant difference in age and gender between patients and normal subjects (P>0.05).Due to the fact that most of the family members accompanying LHON patients to our hospital are their mothers, the majority of carriers included in this study are middle-aged women.
Full-Field ElectroretinographyThe FERG results of the affected patients and asymptomatic carriers are shown in Table 2.Except for PhNR amplitude reduction, the amplitudes the dark-adapted 3.0 a-wave and light-adapted 3.0 a-wave of patients were both significantly decreased(P<0.001).In addition, the amplitudes of the dark-adapted 3.0 a-wave and light-adapted 3.0 a-wave of carriers were also slightly decreased (P<0.001).However, the amplitudes of the dark-adapted 0.01 a-wave and light-adapted 30 Hz flicker electroretinography of patients and carriers were not significantly decreased (P>0.05).

Figure 1 Macular ONL, IS/OS and photoreceptors thicknesses of affected patients, asymptomatic carriers and normal subjects The boxes represent the 25% to 75% interquartile ranges, and the middle lines represent the median.ONL: Outer nuclear layer; IS/OS: Photoreceptor inner and outer segment; PR: Photoreceptor.
Macular Optical Coherence TomographyThe ONL, IS/OS and total photoreceptors thicknesses of the macular fovea,nasal parafovea and temporal parafovea in patients, carriers and controls are shown in Table 3 and Figure 1.Compared with controls, the ONL and photoreceptors thicknesses of the macular fovea in patients was increased slightly (P<0.05).There were no differences between affected patients and normal subjects regarding the thickness of the IS/OS in the fovea or the photoreceptors in the parafovea (P>0.05).The thicknesses of the ONL, IS/OS and photoreceptors of the fovea in asymptomatic carriers were not significantly altered(P>0.05).The ONL and photoreceptors layers of the parafovea in asymptomatic carriers were slightly thinner than those in the controls (P<0.05), whereas no significant differences were detected in IS/OS thicknesses (P>0.05).
Optic Disc Optical Coherence TomographyThe pRNFL thicknesses of affected patients, asymptomatic carriers and controls are shown in Table 4 and Figure 2.The nasal, superior,temporal, inferior and average quadrant pRNFL thicknesses were significantly decreased in the patients compared with those of asymptomatic carriers and controls (P<0.001).None of the quadrant pRNFL thicknesses were significantly different in carriers compared to controls (P>0.05).
DISCUSSION
In this study, FERG and OCT were used to evaluate thefunction and structure of photoreceptors in LHON-affected patients and asymptomatic carriers with the m.11778G>A mutation.Previous studies have shown that LHON usually causes RGC dysfunction, leading to amplitude reduction or prolonged latency of pattern electroretinography, visual evoked potential and PhNR.However, FERG results are usually normal[4,6,14-16].Some studies have revealed sporadic cases with decreased FERG amplitude or delayed latency,indicating partial photoreceptors dysfunction.An animal experiment revealed that the amplitude of the dark-adapted and light-adapted a-wave and b-wave of mitochondrial DNA mutant mice decreased by 17.7%–33.1%[17].Riordan-Evaet al[10]found that among 34 LHON patients, 3 demonstrated a decreased b-wave amplitude.Salom?oet al[9]reported that one patient and one carrier had decreased light-adapted 3.0 electroretinography and 30 Hz flicker electroretinography amplitudes.Changet al[8]reported that 5 of 7 patients showed decreased dark-adapted b-wave or light-adapted 30 Hz flicker response amplitudes.
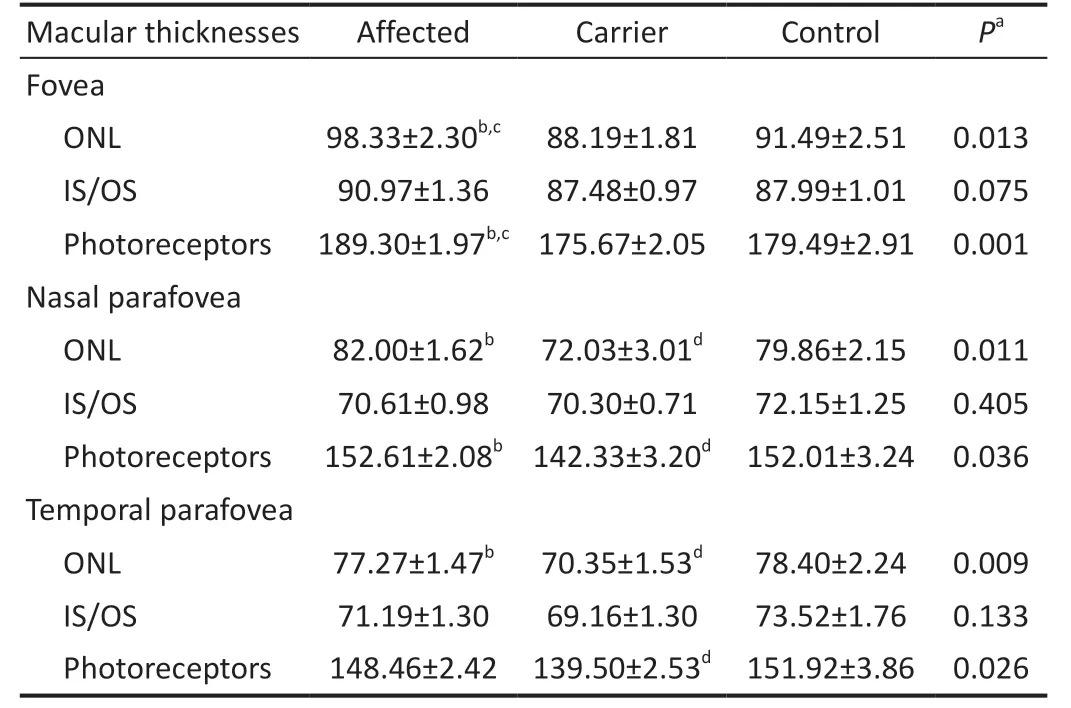
Table 3 Comparison of photoreceptor thicknesses on OCT between affected individuals, carriers, and control μm, mean±SD
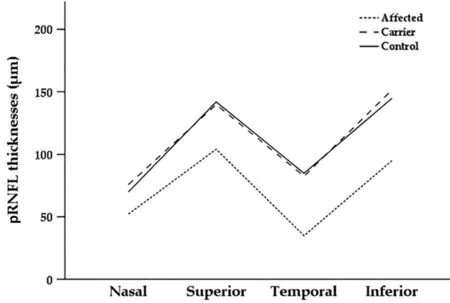
Figure 2 Comparison of the nasal, superior, temporal and inferior pRNFL thicknesses between the affected, carrier, and control groups pRNFL: Peripapillary retinal nerve fiber layer.
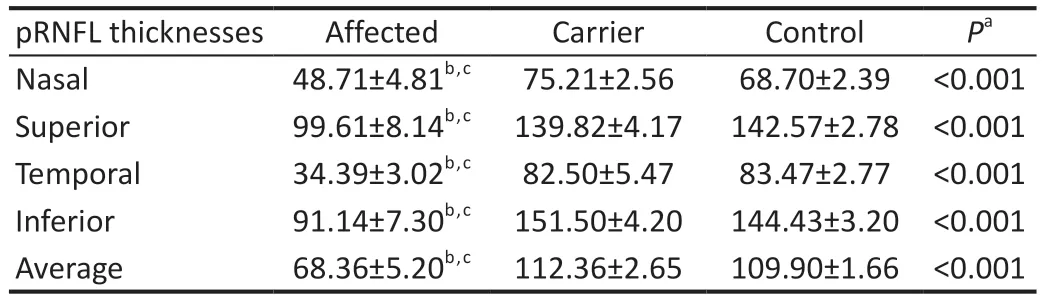
Table 4 Comparison of pRNFL thicknesses on OCT between affected,carrier, and control μm, mean±SD
This study showed that in addition to the decrease in PhNR amplitude, the dark-adapted 3.0 electroretinography and light-adapted 3.0 electroretinography a-wave amplitudes in patients also decreased significantly.The dark-adapted 3.0 electroretinography and light-adapted 3.0 electroretinography a-wave amplitudes in asymptomatic carriers were also slightly decreased.This finding is consistent with previous studies.However, unlike in previous studies, over 90% of the patients and carriers in this study showed abnormal FERG results.One reason for this difference may be that the sample size included in each study was different; additionally, the severity of the patients’disease was inconsistent across studies.In addition,dark-adapted 0.01 electroretinography a-wave amplitudes in affected patients and asymptomatic carriers in this study were not significantly decreased.This result suggests that photoreceptors dysfunction mainly affects cones, and rods are not significantly affected.However, we observed a slight increase in 30 Hz flicker electroretinography a-wave amplitude in asymptomatic carriers, and the specific reasons need further investigation.
The OCT results showed that the pRNFL thickness of patients was significantly decreased compared with that of controls,while there was no statistically significant difference between carriers and controls.In addition, this study found that the ONL thickness of the fovea in patients was significantly increased compared with that in controls.However, there were no differences between patients and controls regarding IS/OS thickness in the fovea or photoreceptors thickness in the parafovea.Our findings are consistent with Liuet al[7], who reported that the thicknesses of the outer layers of the retina,such as the IS, OS and retinal pigment epithelium, was not significantly altered in 16 LHON patients.Nevertheless, Lamet al[11]found that the thickness of the OS in such patients increased significantly, while the thickness of the ONL+IS did not significantly change.They speculated that the cause of OS thickening in LHON patients might be a compensatory morphological reaction caused by optic atrophy rather than photoreceptors dysfunction.
Although there are few studies on photoreceptors in LHON patients, similar results have been found in other glaucomarelated studies.Many studies have demonstrated that the ONL at the fovea in glaucoma patients is significantly thickened, while the IS/OS thickness at the fovea and the photoreceptors thickness at the parafovea are not significantly changed.Histopathology confirmed swelling of the cones.It was speculated that the change in cones resulted from the degeneration of RGCs[18-20].Since LHON and glaucoma are diseases of progressive optic atrophy caused by degeneration and necrosis of RGCs, we speculate that the causes of ONL thickening in the fovea of LHON patients are similar to those in glaucoma.Further prospective studies are needed to explore the causes of photoreceptors morphological abnormalities.Studies have shown that most RGCs are only connected to cones, and cone density is highest in the fovea[21].Therefore,this study mainly observed the abnormal function and structure of cones in LHON patients.In addition, this study found that the thickness of the ONL in the parafovea of asymptomatic carriers was decreased, but the specific mechanism is unclear.Larger sample size studies are required in the future to further investigate the mechanisms underlying ONL thinning.
This study has some limitations.First, the sample size of this study is small, which limits the universality of the conclusions.Second, we manually measured the thickness of the ONL and IS/OS in the macular region, which may have resulted in errors.
In conclusion, this study evaluated photoreceptors function and structure in LHON-affected patients and asymptomatic carriers using FERG and OCT.The dark-adapted 3.0 electroretinography and light-adapted 3.0 electroretinography a-wave amplitudes were decreased, and thickening of the ONL was observed in the fovea of LHON patients.This result suggests abnormalities in the function and structure of photoreceptors, especially cones.Meanwhile, asymptomatic carriers also showed a slight decrease in the amplitude of the a-wave, indicating subclinical dysfunction.The results of this study show that photoreceptors are affected in LHON to some extent in addition to RGCs.Future prospective studies are required to further explore the mechanisms underlying photoreceptors impairment in LHON-affected patients and asymptomatic carriers.
ACKNOWLEDGEMENTS
Authors’contributions:conceptualization, Miao QM, Chen CZ,and Yuan JJ; methodology, Miao QM, Zheng HM, and Chen CZ; examination, Miao QM and Cheng YF; data collection,Miao QM, Cheng YF, Zheng HM, Yuan JJ and Chen CZ; data analysis, Miao QM, Cheng YF, and Zheng HM; manuscript,Miao QM; editing, Miao QM, Zheng HM and Chen CZ.All authors agreed to the final version of the manuscript.
Foundations:Supported by the National Natural Science Foundation of China (No.82101115); Wuhan University Independent Innovation Fund Youth Project(No.2042021kf0094).
Conflicts of Interest:Miao QM, None; Cheng YF, None;Zheng HM, None; Yuan JJ, None; Chen CZ, None.
登錄APP查看全文
 International Journal of Ophthalmology
2023年6期
International Journal of Ophthalmology
2023年6期
- International Journal of Ophthalmology的其它文章
- Role of 7-methylxanthine in myopia prevention and control: a mini-review
- How internal limiting membrane peeling revolutionized macular surgery in the last three decades
- Efficacy and safety of subthreshold micropulse laser in the treatment of acute central serous chorioretinopathy
- Efficacy of ripasudil in reducing intraocular pressure and medication score for ocular hypertension with inflammation and corticosteroid
- Different serum levels of lgG and complements and recurrence rates in IgG4-positive and negative lacrimal gland benign lymphoepithelial lesion
- Subconjunctival conbercept for the treatment of corneal neovascularization