Hematological indices as predictors of mortality in dengue shock syndrome: A retrospective study
2022-09-08 07:08:32GauriKetanBhatnagarParvezSamejaHardevaRamNeharaKuldeepSainiRaviDuttBhupenBhatnagarMohitSinghKhokharVikasKumarAnjaliGarg
Journal of Acute Disease 2022年4期
L.A. Gauri, Ketan Bhatnagar?, Parvez Sameja, Hardeva Ram Nehara, Kuldeep Saini, Ravi Dutt, Bhupen Bhatnagar, Mohit Singh Khokhar, Vikas Kumar, Anjali Garg
1S.P. Medical College, Bikaner, Rajasthan, India
2AIIMS Jodhpur, Rajasthan, India
ABSTRACT Objective: To explore predictive hematological parameters on admission which are associated with mortality in NS1 positive dengue shock syndrome patients.Methods: Demographic characteristics, hematological parameters, and the outcome of NS1 positive dengue shock syndrome patients without any comorbidity and coexisting infections were collected from the Intensive Care Unit and the results were compared between the survivor and non-survivor groups. Results: The mean age was (30.77±11.48) years and 56 (56.6%) patients were males. Out of the total 99 patients, 72 (72.27%) patients were successfully discharged and 27 (27.27%) patients eventually succumbed to death. The most common hematological finding was thrombocytopenia (95.95%), followed by anemia (52.52%) and decreased mean platelet volume (37.37%). After controlling other variables, logistic regression analysis showed that absolute neutrophil count and mean platelet volume were associated with mortality.Conclusions: Total leucocyte count, absolute neutrophil count, and total platelet count are significantly higher, and mean platelet volume is significantly lower in the non-survivor group as compared to the survivor group. Absolute neutrophil count and mean platelet volume are predictors associated with mortality.
KEYWORDS: Dengue shock syndrome; NS1; Complete blood count; Thrombocytopenia; Leucocytosis; White blood cell; Absolute neutrophil count; Mean platelet volume
1. Introduction
Dengue is an acute febrile illness caused by dengue RNA virus which belongs to the Flaviviridae family[1]. Dengue was first described by Benjamin Rush in the eighteenth century and the word “dengue” was taken from the Swahili word “Ka-dinga pepo” which means a seizure induced by an evil spirit[2]. It occurs due to bite of Aedes mosquito and is found in tropical and subtropical regions. According to World Health Organization, the incidence of dengue infection has risen tremendously with around half of the world population at risk and an estimated incidence of 390 million cases per year, and cases in Asian countries account for 70% of the burden in the world[3]. As per data provided by the Director General of Health Services, in the year 2021, India recorded about 193 245 cases with around 20 749 cases from Rajasthan accounting for 10.7% of the national burden. The rising trend of dengue in the past few years has become a global challenge and is primarily credited to population migration from rural to urban areas with sub-standard living patterns causing a higher density and providing breeding places for mosquitoes. The majority of the infected people are asymptomatic or have only mild symptoms such as fever, some may develop severe illness and in a few of them, it can become life-threatening[4]. The clinical course of the disease is divided into 3 phases viz. febrile, critical, and recovery phases. The incubation period is mostly about 4 to 7 days. It is also called “break-bone fever” because of the joint and muscle pain associated with this infection. The commonly observed hematologic changes in dengue fever include thrombocytopenia, leucopenia, and hemoconcentration[5].
Approximately 2%-5% of patients who had dengue infection develop severe complications, so it is very essential to stratify these patients and effectively look for those who require urgent intervention. This is important in resource-limited countries to reduce an overburden on the health care system[6]. Our study aims to describe the potential predictive hematological parameters which are associated with mortality in NS1 positive dengue shock syndrome (DSS) patients.
2. Patients and methods
2.1. Study setting and population
This was a retrospective study and included adult patients (≥18 yrs) with NS1 positive DSS without any comorbidity and coexisting infection who were admitted to the Intensive Care Unit at S.P. Medical College and P.B.M. Hospital, a tertiary care center in North Western Rajasthan during dengue outbreak between September 2021 to November 2021.
2.2. Ethical statement
The study is approved by the Institutional Ethics and Research Board of S.P. Medical College, Bikaner (Rajasthan) vide approval number F. 29 (Acad) SPMC/2022/2200, dated 30/04/2022.
2.3. Definitions
As per WHO classification, dengue hemorrhagic fever was labelled based on the presence of hemorrhage, fever, thrombocytopenia, and plasma leak suggesting increased vascular permeability like hemoconcentration, pleural effusion, ascites, and hypoalbuminemia[7]. DSS denotes dengue hemorrhagic fever with marked plasma leakage showing narrow pulse pressure or hypotension. Increased hematocrit (Hct) was considered as a value >45% while thrombocytopenia was defined as a total platelet count of <1.5 lac/mm3. Anemia was defined as hemoglobin less than 13 g/dL for males and less than 12 g/dL for females. Leucocytosis was considered with white blood cell count (WBC) count >11 000/mm3, neutrophilia was considered with absolute neutrophil count (ANC)>7 700/mm3, and decreased mean platelet volume (MPV) was labeled with a value <9.4 fl[8,9].
2.4. Data collection
Parameters like demographic, clinical, hematological, and the outcome of NS1 positive DSS patients were collected from the Intensive Care Unit. A total of 99 DSS patients were divided into two groups: one included the patients who survived (survivor; n=72) and the other included the patients who died (non-survivor; n=27) during treatment. Hematological parameters on admission were compared between the two groups and analyzed.
2.5. Primary outcome
The primary outcome was in-hospital death.
2.6. Laboratory investigations
Complete blood count of the NS1 positive DSS patients was studied for individual hematological indices like hemoglobin (Hb), mean corpuscular volume (MCV), Hct, WBC, ANC, absolute lymphocyte count (ALC), absolute monocyte count (AMC), platelet count, and MPV.
2.7. Statistical analysis
The statistical analysis was done using SPSS software version 16.0. The continuous variables were represented as median (Q1, Q3) or mean±SD while percentage and frequency were used to represent categorical variables. The Mann-Whitney test and Chi-square test were used to compare the two groups. The significance level of our study was α=0.05.
3. Results
3.1. Demographic characteristics
The demographic characteristics of the patients are shown in Table 1. The mean age was (30.77±11.48) years and 56 (56.6%) patients were male. Fifty-four (54.5%) patients belonged to the urban area and 45 (45.5%) belonged to the rural area. Out of the total 99 patients, 72 (72.27%) patients were successfully discharged and 27 (27.27%) patients eventually succumbed to death (Figure 1).

Table 1. Demographic characteristics.
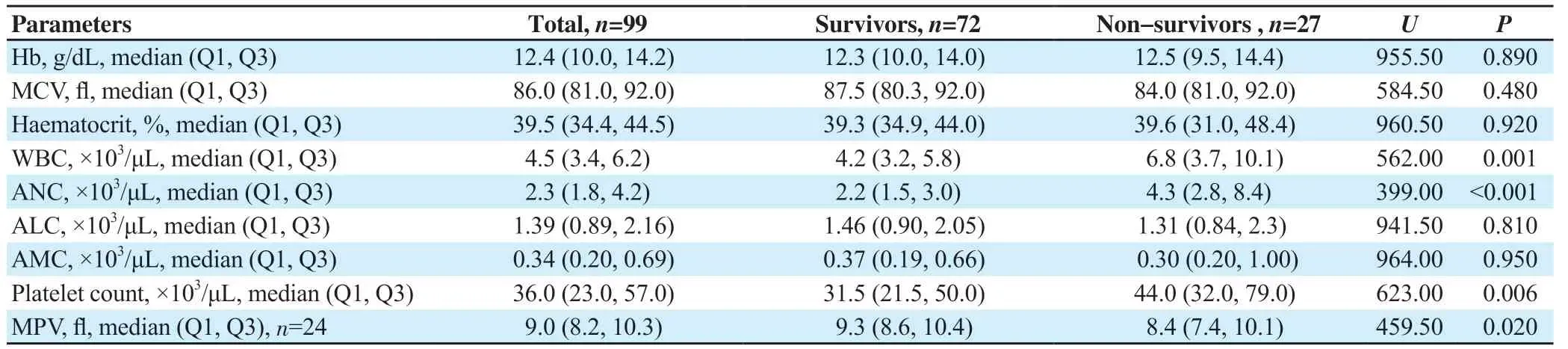
Table 2. Comparison of laboratory parameters in the survivor and non-survivor group.

Table 3. Laboratory findings in the survivor and non-survivor group (n, %).
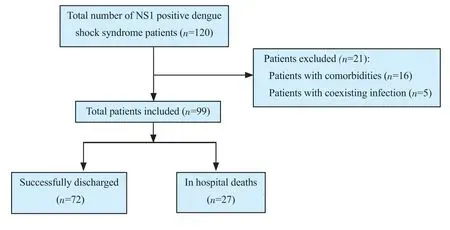
Figure 1. The study flowchart.
Among survivors, the mean age was (31.25±11.17) years, 41 (56.9%) patients were male and 40 (55.6%) patients lived in urban areas while in non-survivor group, the mean age was (29.52±12.41) years, 15 (55.6%) patients were male and 14 (51.9%) lived in urban areas.
3.2. Hematological parameters
The hematological parameters of the patients are shown in Tables 2 and 3. Thrombocytopenia was present in 95 (95.95%) patients and was the most common hematological finding, followed by anemia in 52 (52.52%) patients, decreased MPV in 37 (37.37%) patients, neutrophilia in 8 (8.08%) patients, and leucocytosis in 7 (7.07%) patients. Numbers of patients with leucocytosis (P=0.001) and neutrophilia (P<0.001) were significantly different between the two groups.
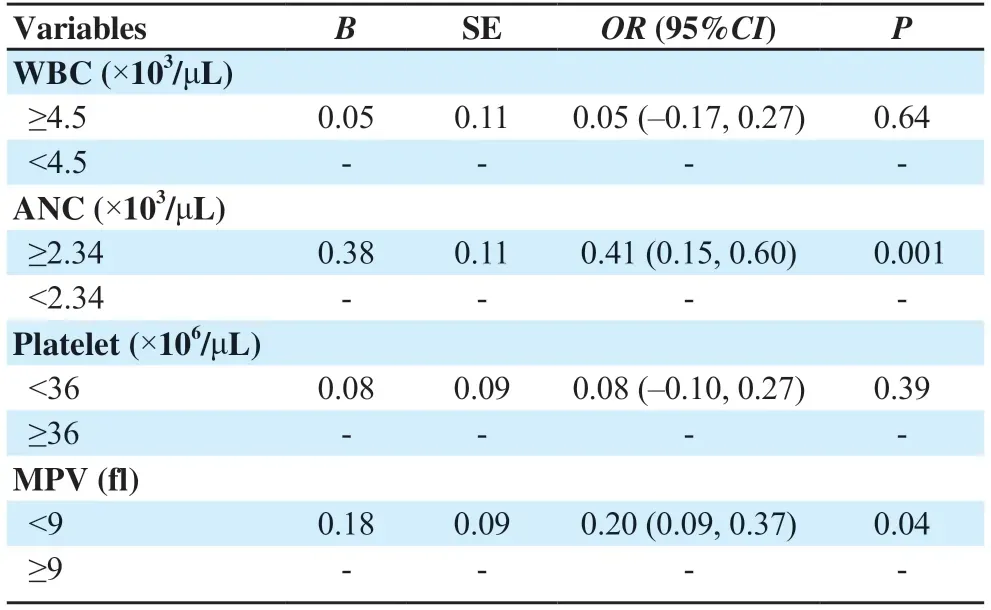
Table 4. Binary logistic regression analysis of variables associated with mortality.
In this study, the median WBC count was significantly higher in non-survivors as compared to survivors [6.8 (3.7, 10.1) cells×103/μL vs. 4.2 (3.2, 5.8) cells×103/μL, P=0.001]. The median ANC was also significantly higher in the non-survivors group [4.3 (2.8, 8.4) cells×103/μL vs. 2.2 (1.5, 3.0) cells×103/μL, P<0.001]. The median platelet count was significantly higher in the non-survivors group [44.0 (3.02, 79.0) cells×103/μL vs. 31.5 (21.5, 50.0) cells×103/μL; P=0.006]. The median MPV was significantly lower in non-survivors [8.4 (7.4, 10.1) vs. 9.3 (8.6, 10.4); P=0.02]. After controlling other variables, logistic regression analysis showed that the predictors associated with mortality were ANC and MPV (Table 4).
4. Discussion
The complete blood count analysis is an effective and noncumbersome way to predicate the outcome of dengue patients. In this study, the in-hospital deaths were significantly associated with higher WBC count, higher ANC, higher platelet count, and lower MPV value. Patients with leucocytosis and neutrophilia were significantly higher in the non-survivors group. The mortality in the study group was 27.27%. Logistic regression analysis after controlling other variables showed that the predictors associated with mortality were ANC and MPV.
In this study, the mean age of the study group was (30.77±11.48) years, 56 (56.6%) patients were male and 54 (54.5%) patients lived in urban areas, which is similar to other studies done in the Indian subcontinent[10-12]. Jain et al[10] reported a mean age of (30.9±13.9) years with males as the majority. Baitha et al[11] also has similar conclusion. The higher male and urban predominance may be due to more outdoor exposure of males and the higher population density in urban areas with a substandard living pattern.
The median WBC count of this study was significantly higher in the non-survivors group. Among the non-survivors, 20 deaths were attributable directly to dengue, 3 deaths were due to ventilatorassociated pneumonia, 3 deaths were due to gastrointestinal bleeding with septic shock and 1 died due to intracranial hemorrhage. Leucopenia is a well-known manifestation in the case of dengue infection and this study demonstrated higher WBC in the nonsurvivors group. The results were in line with other studies[11,13-15]. Singhal et al[13] reported a high WBC count in all fatalities and it has been reported earlier also as a poor prognostic marker. Another study by Amancio et al reported that the factors correlated with mortality were subsequent comorbidities, difficulty of breathing, lassitude, higher WBC, elevated serum creatinine, and decreased serum albumin levels[14]. Baitha et al[11] concluded that a higher leucocyte count, acute kidney injury, and tachypnea at time of admission were significantly associated with higher in-hospital mortality. Another study conducted by Eu-Ahsunthornwattana et al[15] reflected the absence of leucopenia as a marker of severe dengue infection. The associated leucocytosis might be due to gastrointestinal bleed with simultaneous bacteremia, meningitis, or ventilator-associated pneumonia. Therefore, empirical antibiotics should be administered to dengue patients with leucocytosis, altered sensorium, and gastrointestinal bleed[16,17].
ANC was statistically higher in the non-survivor group as compared to the survivor group suggesting bacterial infection. Ralapanawa et al[18] also showed higher leucocyte and neutrophil values in patients with dengue hemorrhagic fever.
Thrombocytopenia was the most common hematological finding in this study but no association was found with the primary outcome. Possible mechanisms of thrombocytopenia include (I) inhibition of bone marrow progenitor cells due to dengue virus, (Ⅱ) increased apoptosis leading to platelet destruction, (Ⅲ) complement-mediated lysis, (Ⅳ) production of anti-platelet antibodies, (V) disseminated intravascular coagulation leading to platelet consumption. The median total platelet count was significantly higher in the nonsurvivor group. This suggests that the platelet count could not predict mortality, which has also been mentioned in some studies[10,11,19]. A study done by Jain et al[10] concluded that platelet counts neither correlate with bleeding manifestations nor determine the disease outcome of dengue infection. Baitha et al[11] also showed that neither bleeding manifestation nor thrombocytopenia determined the mortality. In the study of Chaloemwong et al[19], prolonged duration of thrombocytopenia was seen more commonly in severe dengue patients and was considered to be a predictor of severity rather than total platelet count. The bleeding manifestation in case of dengue infection is more due to coinciding platelet dysfunction and therefore efforts should not be made to just increase the platelet count by transfusion and possessing the patients to undue risk of transfusion reaction. This result was not consistent with some other studies. A study by Pinto et al[20] from Brazil showed that age >55 years, hematuria, gastrointestinal bleeding, and low platelet count were associated with high mortality. Nandwani et al[21] in their study concluded that initial thrombocytopenia, initial leucocytosis, and low MPV are probable predictors of fatal outcomes in disease progression.
The median MPV value in our study was significantly lower in the non-survivor group as compared to the survivor (P=0.02). MPV is an indicator of bone marrow activity, a high MPV denotes increased megakaryocytic activity whereas a low MPV denotes bone marrow suppression and is associated with high chances of bleeding[22]. Studies have shown that dengue fever is associated with a lower value of MPV[21-23]. Nandwani et al[21] in their retrospective analysis observed that low MPV was associated with worse outcome in course of disease. Nehara et al[23] in their study regarding platelet indices in dengue patients showed that low MPV and low PCT (plateletcrit) has appreciable specificity and sensitivity for dengue fever and a low PCT and low platelet count can be used as a predictor of severity in dengue infection. A study by Khatri et al[24] among dengue patients found no significant abnormality regarding MPV, platelet distribution width or PCT compared to controls. Other studies have shown that MPV is not a considerable prognostic marker in dengue infection[22]. Since only a few studies explored the association between platelet indices and disease outcomes, further research is required to confirm the same.
In this study, the mortality rate was 27.27%. This could be due to more sick patients being admitted to the hospital as it is a tertiary care center and therefore represents the Berksonian bias. Case fatality in dengue has varied from 0.5%-5% but in cases of DSS it has ranged up to 44%[15].
This study had a few limitations. It was a single-center study with a small sample size which included only those patients who were admitted to the Intensive Care Unit. The results may differ depending on the geography of the areas, genetic makeup of the patients, and the prevalent serotype. The strength is that a complete blood count can easily be used to stratify the severity of dengue easily and costeffectively in developing countries where well-equipped health infrastructure is lacking.
In conclusion, total leucocyte count, ANC, and total platelet count are significantly higher, and MPV was significantly lower in the nonsurvivor group as compared to the survivor group. After controlling other variables, predictors associated with mortality are ANC and MPV. Hematological indices are objective measures as compared to the subjective findings like generalized weakness, pain abdomen, and headache and therefore are more important in determining the severity and predicting the outcome.
Conflict of interest statement
The authors report no conflict of interest.
Funding
This study received no extramural funding.
Authors’ contributions
L.A.G., H.R.N., and K.B. contributed to the project design, data interpretation, drafting, and revising; P.S., K.S., and R.D. contributed to statistical analysis, data interpretation, and submission; B.B., M.S.K, V.K., and A.G. contributed to collection of data, statistical analysis, and data interpretation. All authors contributed equally to the manuscript.
 Journal of Acute Disease2022年4期
Journal of Acute Disease2022年4期
- Journal of Acute Disease的其它文章
- Challenges of COVID-19 prevention and control: A narrative review
- Delayed post-hypoxic leukoencephalopathy following barbiturate overdose: A case report
- Severe progression of autoimmune hepatitis in a young COVID-19 adult patient: A case report
- Associated risk factors for post-COVID-19 mucormycosis at a tertiary care centre: A cross-sectional study
- Different routine laboratory tests in assessment of COVID-19: A casecontrol study
- Effect of oral premedication of midazolam, ketamine, and dexmedetomidine on pediatric sedation and ease of parental separation in anesthesia induction for elective surgery: A randomized clinical trial