Comparison of outcomes of idiopathic macular holes treated by vitrectomy with air or silicone oil tamponade based on the hole size
2022-08-10 01:39:38LanYinAnQiLiuXinJinLiangJiaFengXiangWang
關鍵詞:幼兒
INTRODUCTION
Macular hole is a full-thickness tissue defect in the retinal neuroepithelial layer of the macular region,which can cause visual loss, visual distortion and other clinical manifestations. Clinical treatment are mainly vitrectomy and internal limiting membrane peeling combined with different intraocular tamponade
. Expansile gas is the favorite tamponade, but due to some incidents of infection in China in recent years, it could not be obtained stably clinically. In fact, disinfected airusually has excellent effect on idiopathic macular hole (IMH) in some situations
, but in the meantime there are still a lot of failed reports
, whose main cause is due to the insufficient duration. So sometimes silicone oil is needed to be used. But because of the well-known side effects and limitation, it is often hard to make a choice between disinfected air and silicone oil. There are few articles comparing the effects of air and gas on IMH surgery, but articles about air
silicone oil has not been found. At present, there is no clear guidance for these two tamponades, and the choice relies mainly on the experience of the operators. In this study, we tried to explore the rule and compare the effects of them according to the closure rates, the closure shape, complications, and the improvement of vision.
SUBJECTS AND METHODS
All patients’ data and essential information were retrieved from medical records during the period from January 2017 to December 2019 in the Ophthalmology Department of Chinese PLA General Hospital. All the patients had been given explanation and signed informed consent before every operation under the supervision by the Medical Management Division of the hospital. And tenets of the Declaration of Helsinki were adhered to for this study.
Inclusion criteria: 1) macular full-thickness hole with stage II or above by optical coherence tomography (OCT)measurement; 2) course of disease ≤2y. Exclusion criteria:1) refractive stromal opacity affecting fundus examination or treatment; 2) history of ocular trauma, surgery or intraocular injection; 3) patients with refractive power <-6.00 D or axial length>26 mm; 4) patients with previous vitreoretinal surgery;5) patients with optic neuropathy; 6) patients with heart,lung, liver, kidney dysfunction or other intolerable surgical treatments; 7) patients with incomplete key follow-up records.All patients underwent best corrected visual acuity (BCVA),intraocular pressure (IOP), slit lamp microscope, fundus preset lens, fundus color photography and macular OCT examination.Zeiss Cirrus HD5000-OCT was used to scan IMH center with the scanning depth of 2 mm and the scanning range of 6×6 mm
. Four diameter lines of 0°, 45°, 90°, and 135°were selected. The minimum value of the four diameter lines measured by the built-in tool of OCT was selected as MMHD.BCVA was performed with international standard visual chart and converted to logarithm of the minimum angle of resolution(logMAR) visual acuity.
All eyes underwent conventional three channel pars plana vitrectomy. The posterior vitreous cortex was detached and cut. Internal limiting membrane was peeled from the upper vascular arch to the lower. Intraocular tamponade with air or silicone oil was employed at the end of the intervention.The 30 cases (30 eyes) were filled with air and 45 cases (45 eyes) with silicone oil. All operations were performed by three experienced doctors. After the operation, the patient kept a facedown position, air group for seven days and silicone oil group for two weeks. All cases were not combined with cataract surgery.
我們的出發點仍然是從語言表達著手來理解弗雷格的對象,關鍵在于理解什么是“不帶有空位”的表達,即理解弗雷格的專名。但正如達米特所言,“弗雷格從未費心對‘專名’這一范疇做過任何精確的規定”,而是“滿足于讓專名與其他類型的表達之間的整個區別依賴于直覺認識,僅以最為馬虎的考察為向導”。[注]Dummett, Frege, Philosophy of Language, Harper & Row, Publishers, 1973, p. 54. 斯魯格則大致總結出了識別弗雷格之專名的四個標準:
SPSS 21.0 was used for statistical analysis, and the measurement data was expressed as mean±standard deviation (mean±SD). The
-test was used to compare the common data between the two groups and between the groups in different MMHD intervals. Fisher exact probability test was used to test the closure rates and closure grade ratio of IMH after operation. BCVA before and after operation was compared with paired
-test.
<0.05 was statistically significant.
上述的三類傳統算法主要基于圖像整體信息的變化來選定關鍵幀,容易造成關鍵幀選取錯誤、計算量大、實時性差等問題。因此,本文在此基礎上使用一種基于深度學習的目標檢測方法,通過建立卷積神經網絡(Convolutional Neural Network,CNN)模型,分類提取視頻中列車頭部、尾部及車身所在關鍵幀,使得基于深度學習的目標檢測在關鍵幀提取的應用中成為可能。
RESULTS
Totally 75 patients (75 eyes) with IMH who underwent vitrectomy combined with internal limiting membrane peeling were included in this study. There were 21 males and 54 females with the average age of 61.2±8.1y. The courses of disease ranged from two weeks to 24mo. The average course was 3.8±7.2mo.
In the air group, there were 8 males and 22 females with the average age of 63.1±9.6y and the average course of 3.6±8.5mo. In the silicone oil group, there were 13 males and 32 females with the average age of 58.7±7.0y and the average course of disease of 4.0±6.5mo. There was no significant difference in age and course of disease between the two groups(all
>0.05). In the range of MMHD ≤400 μm (MMHD1)there were 23 eyes in air group and 16 eyes in silicone oil group; the average of MMHD were (277.6±43.9) and(303.4±43.1) μm respectively; the average of BCVA were 1.23±0.46 and 1.27±0.50 respectively; there was no statistical difference (
>0.05). In the range of MMHD>400 μm (MMHD2)there were 7 eyes in air group and 29 eyes in silicone oil group;the average of MMHD were (491.6±70.8) and (525.4±103.6)μm respectively; the average of BCVA were 1.41±0.32 and 1.40±0.39 respectively; there was no statistical difference(
>0.05).
In this retrospective study, there was no difference in the overall closure rates of IMH between air group and silicone oil group. Venkatesh
studied various quantitative parameters of IMH by observing pre- and post-operative OCT images, and found a significant negative correlation of IMH closure with MMHD. Similarly, we found that the closure rate of MMHD1 in air group was higher than that of MMHD2;although there was no difference in silicone oil group between MMHD1 and MMHD2, MMHD1 was higher than MMHD2 in absolute value. Furthermore, we subdivided MMHD and compared air group with silicone oil group again. There was no significant difference in MMHD1 closure rates between the two groups; the closure rate of MMHD2 silicone oil group was higher than that of air group. The results showed that the two tamponades both have satisfactory closure effects for smaller IMH, and there was little difference between them; for larger IMH, the closure rate of silicone oil was obviously higher than that of air.
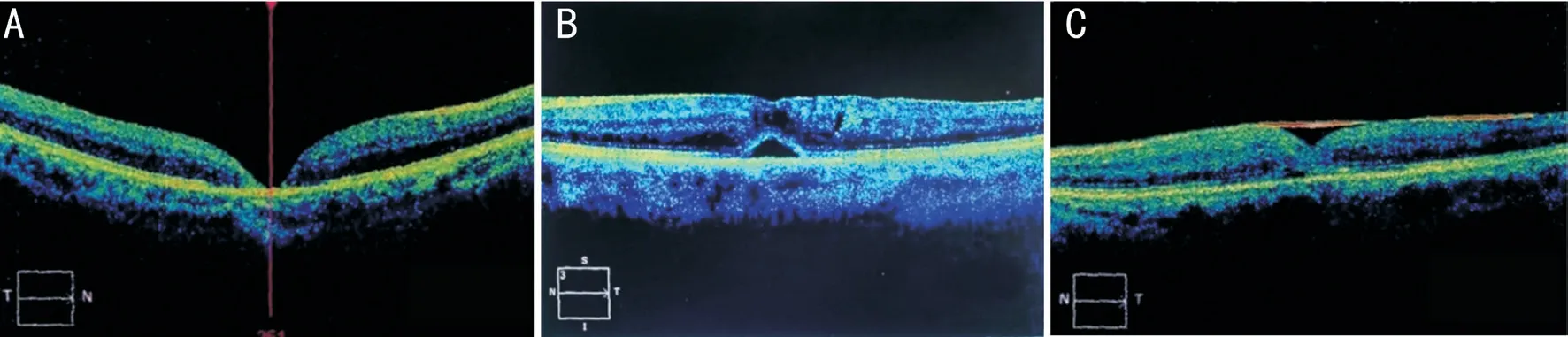
One month after the operation, BCVA, IOP, slit lamp microscope, fundus color photography and OCT were performed with the same equipment and method as before.The closure rates, complications and BCVA of air group and silicone oil group in different MMHD intervals before and after the treatment were compared and analyzed. The disappearance of neuroepithelial layer defect in macular area showed by OCT examination was regarded as IMH closure, while its existence was regarded as IMH unclosed (Figure 1A)
. According to the reference
, the closed IMHs were divided into two grades:A (bridge closure) and B (good closure). Grade A: Subretinal fluid was still present in the class a fovea (Figure 1B). Grade B:fovea was restored to a basically normal structure (Figure 1C).
實驗目的 《新疆維吾爾自治區農村雙語幼兒園課程設置方案(試行)》(新教雙〔2017〕15號)要求:“激發各族幼兒學習國家通用語言的興趣,讓他們能夠在生動活潑的教育活動中獲得國家通用語言的聽、說能力。”通過實驗驗證信息技術能夠提升南疆農村幼兒國家通用語言聽說能力的發展。
One month after the operation, there was no significant change in the lens of all eyes in the air group, but the lens opacity of three eyes deteriorated in the silicone oil group. No serious complications such as endophthalmitis occurred in all cases.
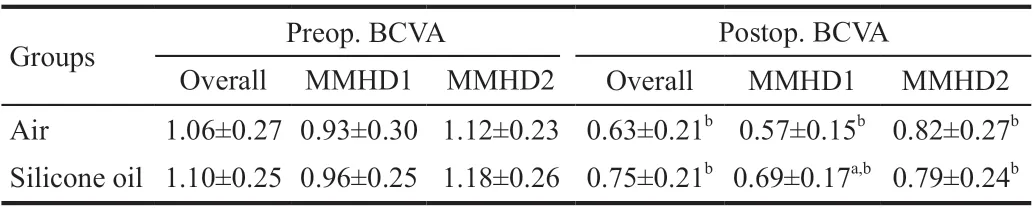
The postoperative BCVA of the air group, the silicone oil group and the subgroup according to the MMHD were improved compared with the preoperative (all
<0.05). There was no significant difference in the postoperative BCVA between the overall air group and the overall silicone oil group, while the MMHD1 air group was better than the silicone oil group(
<0.05), and there was no significant difference between the MMHD2 air group and the silicone oil group (
>0.05; Table 3).According to the literature, ocular hypertension (OHT) has been defined as a postsurgical IOP>21 mm Hg or an increase of >10 mm Hg over the IOP baseline
, and ocular hypotony has been defined as a postsurgical IOP≤7 mm Hg
. There were seven eyes (15.56%) with ocular hypertension in silicone oil group and none in air group. Under the treatment with captopril hydrochloride and brinzolamide eye drops, all the IOP returned to normal within one week. There were two eyes(6.7%) with ocular hypotony in the air group, but without retinal nor choroidal detachment.
One month after operation, there was no significant difference in closure grade between MMHD1 air group and silicone oil group (
>0.05), but the proportion of Grade B in MMHD2 silicone oil group was higher than that in air group (
<0.05;Table 2).

DISCUSSION
The closure of macular hole is mainly due to the release of traction in the vertical and tangential directions
, and the top pressure of tamponade on the neuroepithelium at the edge of the hole
. It is generally considered that inert gas is a relatively ideal tamponadematerial because of its long duration effect and few side effects
. However, in recent years, most of Chinese medical institutions lack of inert gas because of infection and related problems. So, the surgeons could only choose between disinfected air and silicone oil.
One month after operation, IMHs were closed in 26 eyes out of 30 eyes in air group, and the closure rate was 86.67%. IMHs were closed in 43 eyes out of 45 eyes in silicone oil group,and the closure rate was 95.56%. There was no significant difference in IMH closure rate between the two groups(
>0.05). In MMHD1, IMHs were closed in 22 eyes out of 23 eyes in air group, and the closure rate was 95.65%; IMHs were
all closed in 16 eyes in silicone oil group, and the closure rate was 100.0%, there was no significant difference between the two groups (
>0.05). In MMHD2, IMHs were closed in four eyes out of seven eyes in air group (57.14%), and in 27 eyes out of 29 eyes in silicone oil group (93.1%), so the silicone oil group showed a better result than the air group (
<0.05).The closure rate of MMHD1 in air group was higher than that of MMHD2 (
<0.05), while the closure rate of different MMHD didn’t exist significant difference in silicone oil group(
>0.05), but the rate of absolute value in MMHD1 was higher than that in MMHD2 (Table 1).
For smaller IMH (≤400 μm), the efficacy of vitrectomy combined with air should be considered better than silicone oil; for larger IMH (>400 μm), the efficacy of silicone oil may be better than air.

There was no significant difference in BCVA between the overall air group and the overall silicone oil group. Because some studies had shown that the improvement of visual function was closely related to both the MMHD and the closure rate of IMH
, each group was subdivided according to MMHD in our study. It was found that BCVA of MMHD1 air group was better than silicone oil group, but significant difference was not found in MMHD2 between the two tamponades. There are many determinants of visual acuity after IMH surgery. For the comparison of air and silicone oil, the main factors are the closure rate, closure shape and complications
. There was no significant difference in the closure rate and shape between the two MMHD2 groups. The difference of BCVA was mainly due to the complications of silicone oil, such as complicated cataract and secondary glaucoma. In addition, the side effects of silicone oil on visual acuity include promoting preretinal proliferation and even causing macular fold
. Besides, there are many reports about the damage of optic nerve and optic chiasm caused by silicone oil drops
. In our study, the silicone oil group was better than the air group in terms of the closure rate and closure shape in MMHD2 because of the better efficacy of continuous top pressure. But at the same time,the complications of silicone oil offset those advantages.As a result, there was no significant difference in BCVA between the two MMHD2 groups.
Through this study, it can be concluded that for smaller IMH,choosing air can obtain better vision with similar closure rate,and relieve patients from pain and complications; for larger IMH, choosing silicone oil can achieve better closure efficacy with similar postoperative vision.
(1)完善顧客導向型偏離量表的文化普適性。雖然Leo等學者嚴格按照量表開發程序,最終形成顧客導向型偏離的測量量表,但該量表是以澳大利亞接待業一線員工基于自身工作經歷而形成的問項池,直接用于測量我國酒店業一線員工的顧客導向型偏離時,是否存在文化差異還不得而知。因此,顧客導向型偏離量表……
登錄APP查看全文
猜你喜歡
天津教育(2023年2期)2023-03-14 07:34:52
早期教育(美術教育)(2021年9期)2021-10-13 06:04:46
早期教育(美術教育)(2021年5期)2021-09-22 01:39:06
早期教育(美術教育)(2021年3期)2021-09-18 02:55:17
早期教育(美術教育)(2021年4期)2021-09-18 02:12:23
早期教育(美術教育)(2021年2期)2021-09-15 02:07:27
早期教育(美術教育)(2021年11期)2021-06-30 14:55:22
中國生殖健康(2020年7期)2021-01-18 03:02:24
甘肅教育(2020年6期)2020-09-11 07:45:12
動漫界·幼教365(小班)(2019年6期)2019-06-10 02:14:04
 International Journal of Ophthalmology
2022年8期
International Journal of Ophthalmology
2022年8期
- International Journal of Ophthalmology的其它文章
- Advances in the research of plant-derived natural products against retinoblastoma
- Acute bilateral anterior uveitis in paediatric inflammatory multisystem syndrome temporally associated with COVlD-19
- Metamorphopsia as the first clinical sign of renal cell carcinoma
- Sutureless contact lens-type amniotic membrane for persistent epithelial defects after infectious keratitis
- A case of conjunctival intraepithelial neoplasia with spheroidal degeneration: a clinicopathological study
- Risk of anxiety and depression in patients with uveitis: a Meta-analysis