Clinical features and management of ureteric stump syndrome:Singlecentre experience and contemporary literature review
2022-07-20 05:46:32
Asian Journal of Urology 2022年2期
Dear editor,
“Ureteric stump syndrome(USS)”is a rare entity(incidence 0.8%—1.0%)with left-over in situ distal-ureter being the culprit[1—3].The presentation may be recurrent urinary tract infection(UTI),flank/abdominal pain,or hematuria[1,4].Although only few of the patients require intervention(approximately 1.1%—10%)[1—3],either with open excision of the stump[1—3]or via minimally invasive endoscopic approach[5,6],prompt diagnosis is often delayed.During simple nephrectomy,dilemma exists whether to consider concomitant total ureterectomy to eliminate the future risk of USS[4],or to consider subtotal-ureterectomy along with nephrectomy[1—3].In this letter,we present a retrospective analysis of clinical presentation,diagnostic approach,and management of three patients of USS(Table 1)treated at our centre and try to solve all these dilemmas.
Bilateral Cohen’s cross-trigonal ureteric reimplant was performed in a four-year-old boy with bilateral vesicoureteric reflux(VUR).Four years later,he again underwent left to right transureteroureterostomy with right ureteric rereimplant(Lich-Gregoir)due to left distal ureteric stricture with persistent right reflux.He ended up in chronic kidney disease and underwent renal transplantation after having pre-transplant bilateral laparoscopic simple nephrectomies.Six months after transplantation,he presented with persistent fever with UTI.Imaging showed abscess at the right renal fossa near the right native ureteric stump(Fig.1Aand 1B).He underwent open complete excision of the right native ureter.Post-operatively he had febrile episode for 3 days.
A twenty-seven-year-old lady underwent left open simple nephrectomy for non-functioning left kidney secondary to ureteric stone 4 months back elsewhere.She presented with non-healing discharging sinus from the drain site(started one-month after surgery).Tuberculosis was ruled out.Imaging showed retained left lower ureter with ureteric stones in situ with uretero-cutaneous fistula(Fig.1C—1E).Laparoscopic left completion ureterectomy was performed.The ureteric stump proximal to the stone was found dehiscent.She recovered satisfactorily.
A 71-year-old gentleman,diabetic and hypertensive,was diagnosed 3 years back with left lower ureteric stricture(inflammatory)with poorly functioning left kidney.He underwent left laparoscopic nephroureterectomy with removal of the stricture part of ureter(histopathology:Chronic pyelonephritis and chronic ureteritis,no evidence of malignancy).He presented with hematuria after 3 years.Imaging revealed mass in the left remnant of the ureter(Fig.1F and 1G)extending into the bladder.After multidisciplinary team opinion,he underwent robotic completion left ureterectomy with radical cystectomy with bilateral pelvic lymph node dissection with ileal conduit(histopathology:High grade transition cell carcinoma involving the left ureter and VUJ, pT3aN1). Postoperatively he had an episode of sepsis with acute kidney injury.
Completion ureterectomy during simple nephrectomy will require longer incision or separate incision(for laparoscopy,different port position)and may require transabdominal approach(for open extraperitoneal cases)which will increase the morbidity.Over that,problems related to residual distal ureters are rare and can be managed with intervention with successful results[1—3].de Caluwe et al.[2]in their studies on both open uppermoiety heminephrectomy and lower-moiety heminephrectomy recommended that complete excision of the ureter is not mandatory.Other authors in the literature have also commented that distal ureteric stump rarely caused a problem.In fact,Cain et al.[3]have favoured nephrectomy with partial ureterectomy for management of non-functioning kidney.Ade-Ajayi et al.[7]even added that distal ureterectomy may increase the risk of injury to the healthy ipsilateral lower-moiety ureter in duplex system.However,Androulakakis et al.[1]emphasized to keep ureter stump as short as possible,as longer ureteric stumps may predispose patients to develop USS.Casale et al.[8]discovered preoperative VUR as a contributing factor for USS and encouraged completion ureterectomy for patients with reflux.Persad et al.[4]also had similar opinion.Thus,the consensus is that complete ureterectomy along with nephrectomy is not up-front required for benign cases.However,in the presence of VUR on the ipsilateral side complete ureterectomy may be considered.Stone left in the ureter may be a source of infection.Hence,the ureterectomy specimen should include the stone-bearing segment.In our study,one patient had VUR and one had ureteric stone with non-functioning kidney.In such situations,surgeons should consider removal of the ureter completely or at least beyond the stone.
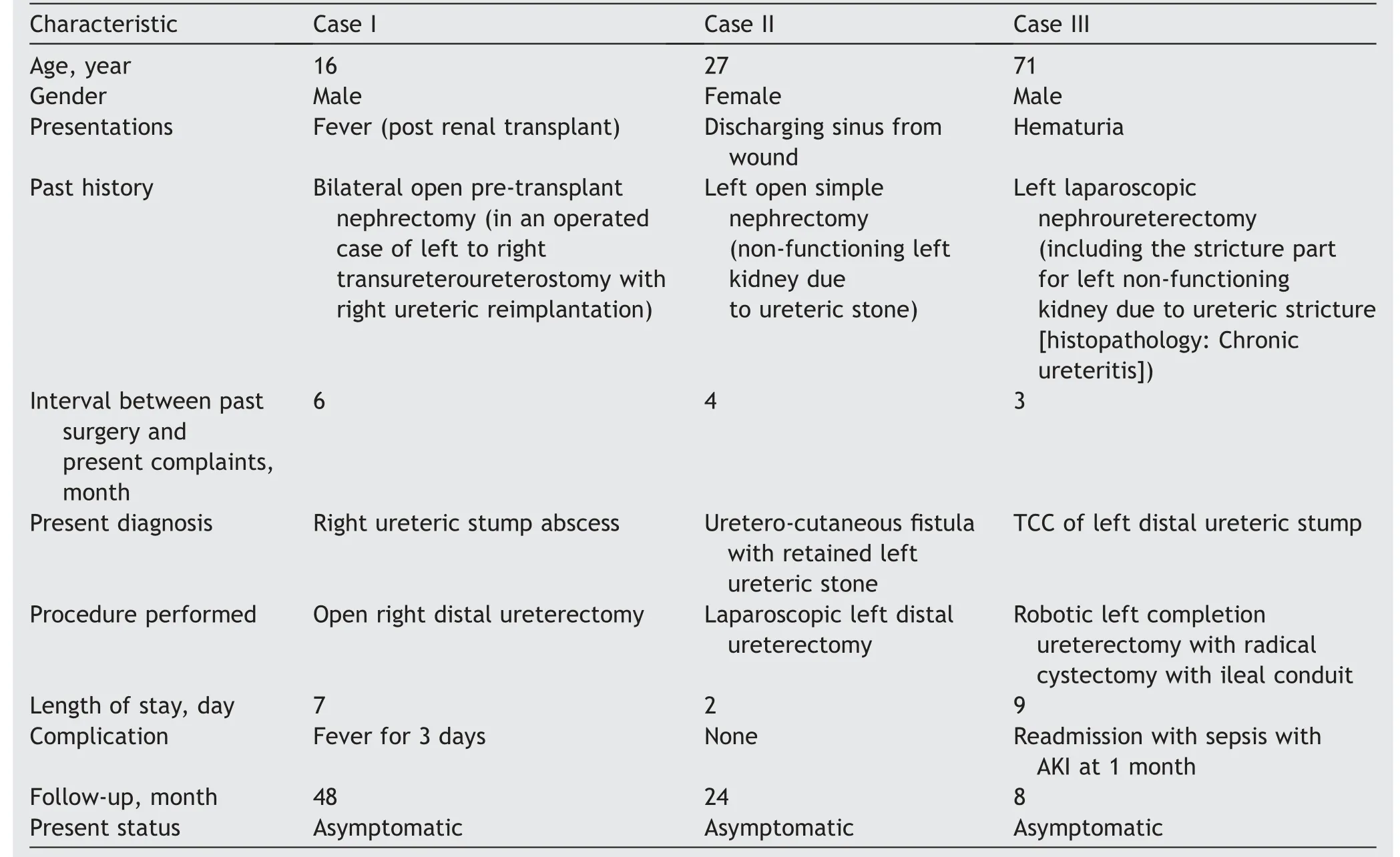
Table 1 Data of three patients with ureteric stump syndrome.
Clinical presentation of USS may range from UTI,abscess,hematuria,flank pain to even uretero-cutaneous fistula.There have been individually reported case of empyema of the retained ureter in literature.One article has reported stone in a retained ureteric stump after ileocystoplasty.Even a case of fistulae developing between ectopic ureteric stump and uterus following simple nephrectomy,has been noted in literature.Development of malignancy in retained stump had also been noted by Kim et al.[9].Clinical suspicion is the key for successful diagnosis of USS.Infective causes need to be ruled out.Ultrasound is an office-based non-invasive tool to detect collection or distended stump.Micturating cystourethrogram will be helpful to detect reflux.Computed tomography can easily detect the presence of any stone,abscess,empyema,mass,or fistulous communication.Cystoscopy is an integral part of haematuria evaluation and should be a part of investigation if haematuria is present or imaging is suspicious of malignancy.
Simple excision of the retained ureter either by open or laparoscopic technique is the best treatment option of USS[1—3].Casale et al.[8]reported successful laparoscopic distal ureterectomy.Escolino et al.[10]advised to always perform transperitoneal laparoscopy to excise maximum ureter.We performed in our study laparoscopic ureterectomy in one case and robotic assisted ureteric stump excision with radical cystectomy in another.Endoscopic methods include sub-ureteric injection or endoscopic fulguration.Bullock et al.[5]reported endoscopic sub-ureteric injection of dextranomer/hyaluronic acid as treatment for refluxing ureteric stumps.Ehrlich et al.[6]described transurethral fulguration as well as open fulguration of the stump successfully.Some authors also treated patients with endoscopic electrofulguration followed by ureteric filler material injection.Bullock et al.[5]also successfully did semirigid ureteroscopy and lithotripsy.Although we did not use any endoscopic procedures,literature suggested endoscopic techniques for treatment of selected USS are valid treatment options.
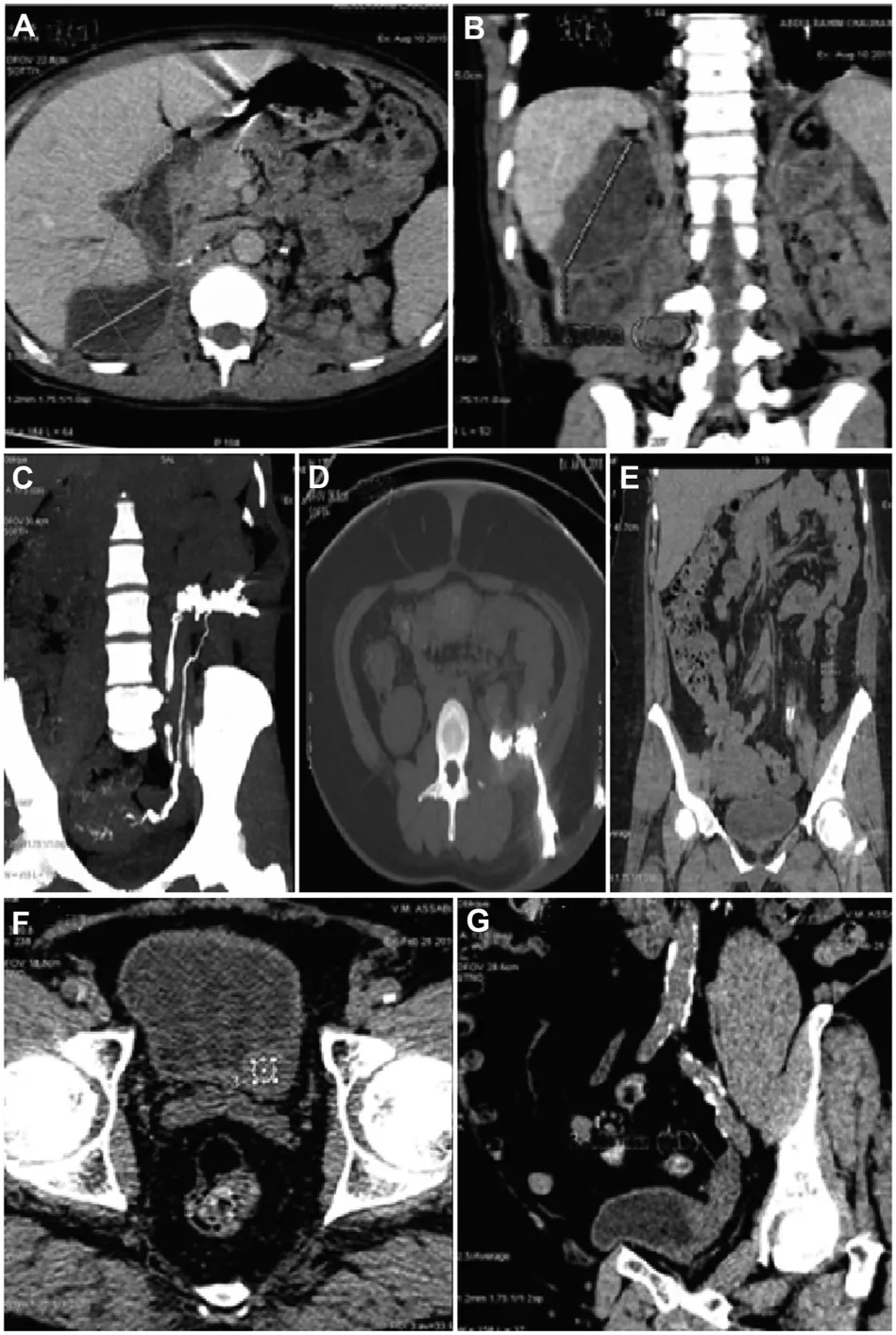
Figure 1 Computed tomography images of patients with ureteric stump syndrome.(A)Right renal fossa collection(transverse view);(B)Right renal fossa collection(coronal view);(C)Uretero-cutaneous fistula (coronal view);(D)Uretero-cutaneous fistula(transverse view);(E)Ureterocutaneous fistula with retained stone in the left ureter;(F)Left vesico-ureteric junction region and distal left ureter mass(transverse view);(G)Left vesico-ureteric junction region and distal left ureter mass(sagittal view).
Incidences of USS are low;hence,it is difficult to carry out a large-sample prospective study.With these three index cases,we tried to summarise the approach and management of USS by proposing an algorithm(Fig.2).To conclude,USS diagnosis is challenging as clinical presentations are varied.Radiological investigations are essential for detection.Completion ureterectomy is the permanent remedy either in open and laparoscopic surgical approach.Endourological approaches are also up-coming for management of USS.Contemporary literature does not support complete ureterectomy in all cases of simple nephrectomies.
Author contributions
Study design:Krishnendu Biswas,Abhishek G.Singh.
Data acquisition:Krishnendu Biswas.
Data analysis:Krishnendu Biswas.
Drafting of manuscript:Krishnendu Biswas.Critical revision of the manuscript:Arvind P.Ganpule,Ravindra B.Sabnis,Mahesh R.Desai.
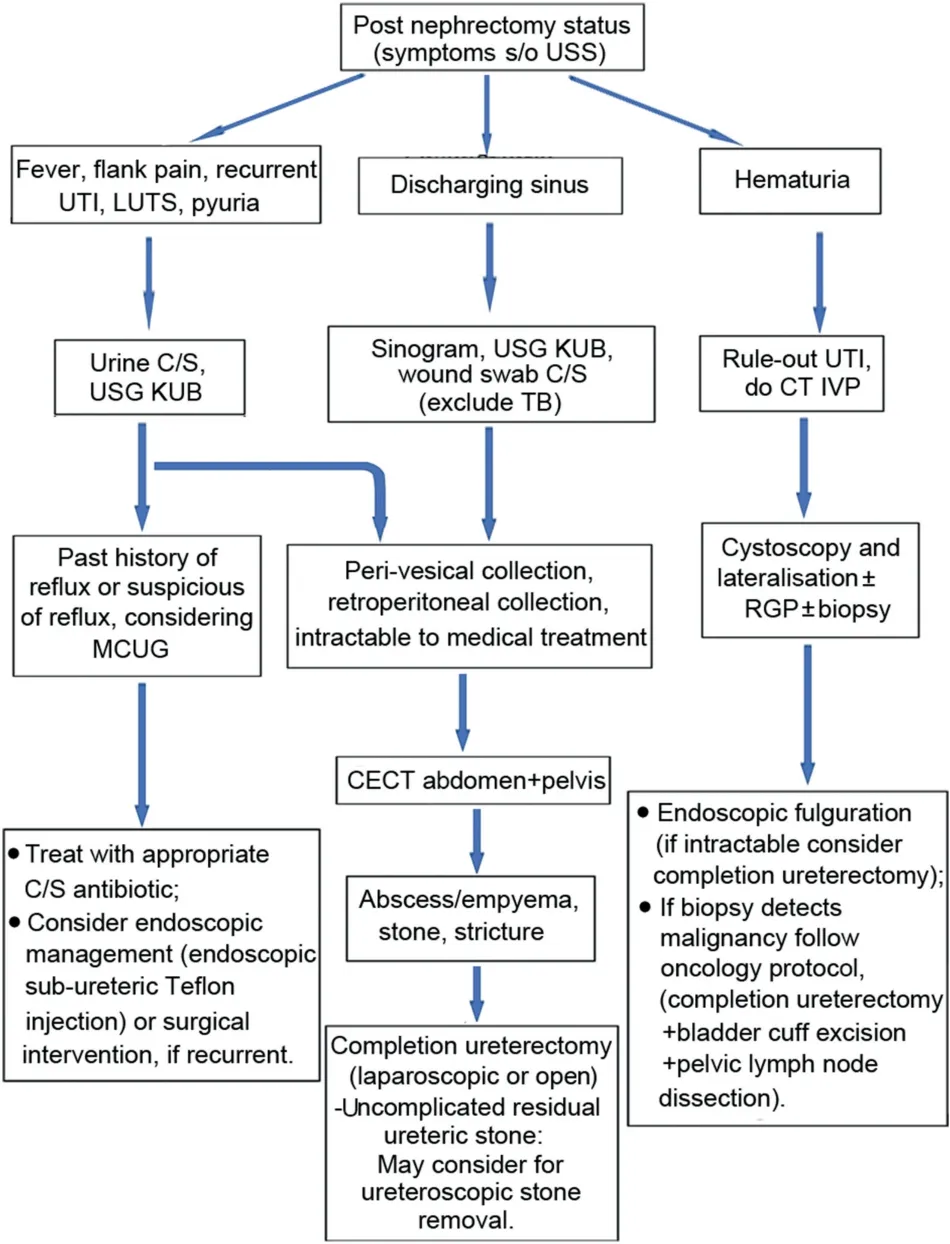
Figure 2 Algorithm of approach to ureteric stump syndrome.USS,ureteric stump syndrome;UTI,urinary tract infection;LUTS,lower urinary tract infection;s/o,suggestive of;C/S,culture&antibiotic sensitivity;TB,tuberculosis;USGKUB,ultrasonography kidney-ureter-bladder;CT IVP,computed tomography with intravenous pyelography;MCUG,micturating cystourethrogram;CECT,contract enhanced computed tomography;RGP,retrograde pyelography.
Conflicts of interest
The authors declare no conflict of interest.
 Asian Journal of Urology2022年2期
Asian Journal of Urology2022年2期
- Asian Journal of Urology的其它文章
- Manuscript Guide for Authors
- Encrusted cystitis and ascites due to urethral calculus
- Impact of coronavirus disease 2019 on semen parameters
- Clinical lesson learned from genetic analysis in patients prior to surgical repair of hypospadias
- Factors influencing the degree of participation in surgical decision-making among Chinese patients with prostate cancer:A qualitative research
- Impact of delay from transperineal biopsy to radical prostatectomy upon objective measures of cancer control