Temporary severe oculomotor nerve palsy after reconstruction of orbital medial wall fracture: a case report of nonfamiliar complication
2022-06-22 03:12:34YeonWoongChungTaeYoonLa
Commonly known complications following reconstruction of an orbital fracture include diplopia, hemorrhage, and displacement or infection of the orbital implant, and some studies have reported ptosis caused by temporary or permanent oculomotor nerve palsy after operation
. However, no study has reported a case of both medial and superior rectus palsy with ptosis. Ptosis and medial and superior rectus palsy are hypothesized to have a neurogenic origin of reversible or irreversible impairment of the oculomotor nerve branch that connects to the muscle, rather than by direct damage of the levator muscle or extraocular muscle
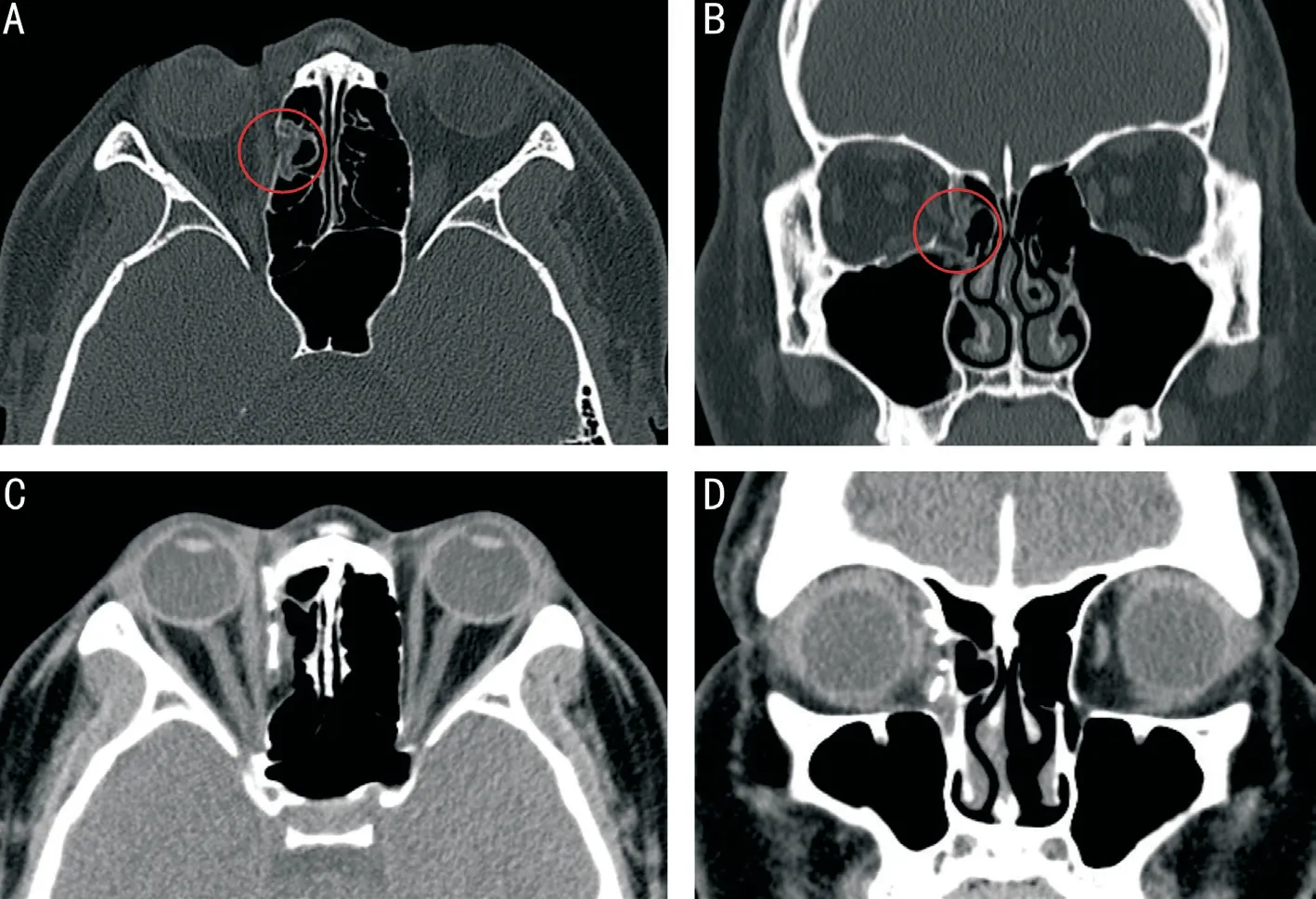
. However, it is difficult to identify which part of the nerve branch was damaged and which manipulation during or after surgery caused the damage.We experienced a case of temporary severe oculomotor nerve palsy which showed both complete ptosis and medial and superior rectus palsy that developed immediately after a successful reconstruction of an orbital medial wall fracture.We present this nonfamiliar complication of orbital medial wall fracture repair with a literature review. The study was conducted in accordance with the Declaration of Helsinki.Proper consent for publication of photographs of patient was taken.A 21-year-old female patient presented to the clinic under suspicion of an orbital wall fracture after hitting her right eye on the ground following a fall four days prior. An ophthalmic examination revealed slight edema and ecchymosis in the eyelids. During the extraocular movement examination, the patient experienced pain during medial gaze and -1 degree of extraocular movement limitation and diplopia during upward gaze. Exophthalmometry showed 14 mm in the right eye and 15 mm in the left eye. On orbital computerized tomography(CT), a moderate fracture in the orbital medial wall of the right eye was observed, with slight incarceration of the orbital tissue and the medial rectus at the fracture site (Figure 1A-1B). Based on the imaging results and clinical findings, reconstruction of the orbital wall fracture was performed. Under general anesthesia, the orbital medial wall fracture site was exposed by a transcaruncular-conjunctival approach to release the incarcerated orbital tissue, and fractured bone fragments were removed. The fracture site was reconstructed with a 1-mmthick titanium mesh MEDPOR
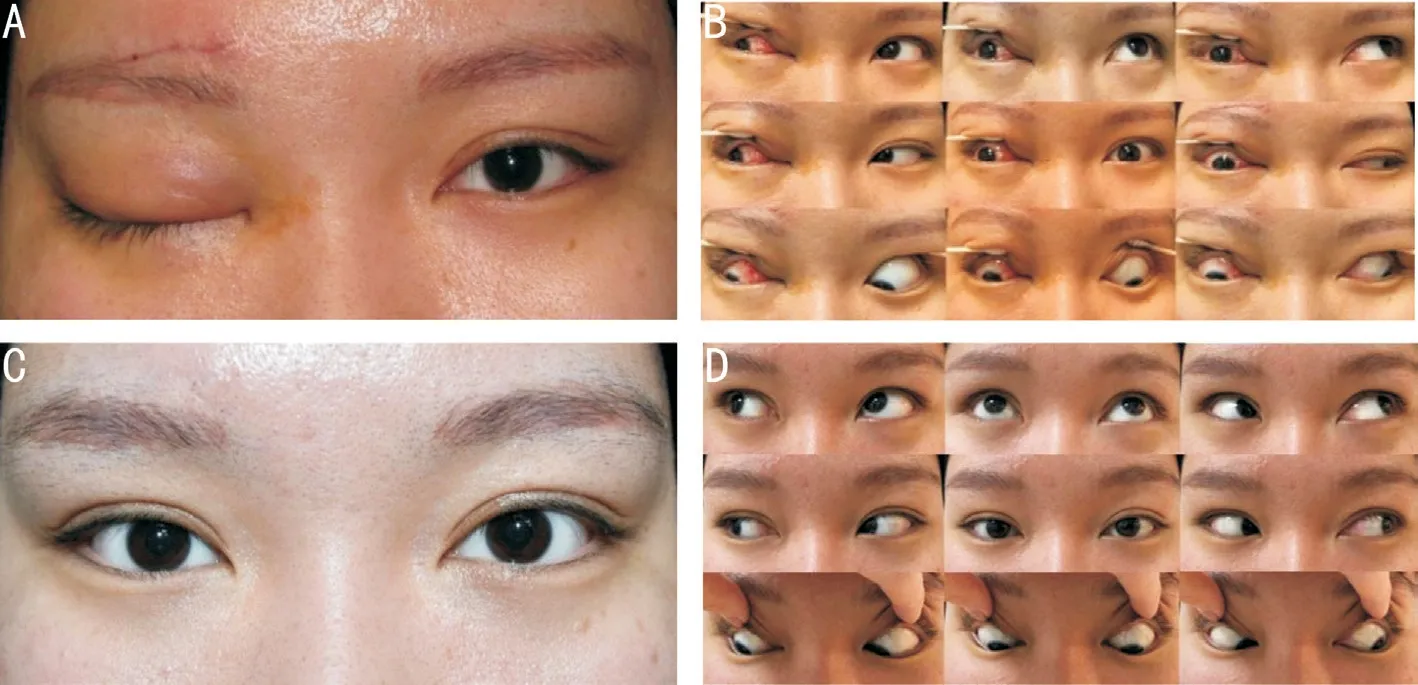
implant. The operation was successfully completed within the normal time range without any problems. However, after recovery from anesthesia,the patient was unable to open her right eye despite mild lid swelling, and the right eye showed severe exotropia of about 45 prism diopters (PD) with complete limitation of ocular movement in the medial and upward directions. Visual acuity and pupillary reactions were normal, but the patient was immediately administered oral steroid of 60 mg (Solondo
) as compressive oculomotor nerve palsy was suspected. The dose of the drug was reduced by half every week, and administration was discontinued about 4wk after surgery. The patient was unable to open her eyes upon examination one day after operation, and the levator function test showed 0 mm, with no improvement in extraocular movement (Figure 2A-2B).The patient was able to slightly open her eyes from one week after the operation and perform limited ocular movements in the medial and upward directions, showing 0 mm of marginal reflex distance (MRD), 1.5 mm of interpalpebral fissure (IPF),5 mm of levator function (LFT), and 30 PD of exotropia. In addition, the ocular movement test showed an improvement from -4 to -3 in both medial and upward directions. Ptosis improved over time; when the patient visited the clinic one month after the operation, MRD 1 was measured at 2 mm,IPF at 7 mm, and LFT at 10 mm, with the angle of exotropia reduced to 15 PD. The ocular movement test showed further improvement to -1 in both medial and upward directions.Three months after the operation, the patient’s lid returned to the preoperative position, and ocular movements were normal, showing orthophoria in all gaze directions (Figure 2C-2D). Diplopia was not observed, and the patient recovered completely. Orbital CT performed three months after the operation showed a well reconstructed orbital medial wall and no damage or abnormality in all extraocular muscles (Figure 1C-1D).Many studies have reported temporary ptosis caused by compression or damage of the oculomotor nerve
lid trauma,sphenoid sinus inflammation, pituitary tumor, intracranial vasculopathy, and neurosurgery
. However, reports on ptosis caused by oculomotor nerve palsy after reconstruction of orbital wall fracture are rare
, and there is no prior report of ptosis combined with severe medial and superior rectus palsy.Anatomically, the terminal portion of the oculomotor nerve is divided into the superior branch that passes through the bottom of the superior rectus, where it divides again into the branch that controls the superior rectus and another that controls the levator muscle. In particular, the branch that connects to the levator muscle is longer than that connecting to the extraocular muscle and is more susceptible to manipulations carried out in the narrow orbital space because of its extraconal path
.Reconstruction of orbital medial wall fracture requires special attention because of structures like the inferior oblique muscle,medial canthal tendon, and ethmoidal artery and nerve. If the fracture site is largely located at superiorly and posteriorly, it is difficult to perform repair procedures. In this case, excessive pressure may have been exerted on the retractor to secure the operation field, which may have damaged the surrounding tissues, causing edema. A prolonged operating time may affect the nerve structures in the orbital space. The exact cause and mechanism of temporary ptosis and medial and superior rectus palsy after orbital wall fracture repair have not been identified.However, these symptoms are hypothesized to be caused by two pathophysiologic mechanisms. One is neurapraxia caused by pressure-induced ischemia due to traction or compression of the surrounding orbital tissue, including the terminal portion of the oculomotor nerve. The resulting traction or compression of orbital content can induce local high pressure on the terminal branch of oculomotor nerve. The second is stretching injury of oculomotor nerve branch, resulting from excessive pulling or traction of the orbital content
. Such temporary palsy symptoms caused by trauma or compression naturally recover over time in most cases, requiring no special treatment. However, initial administration of high-dose steroids protects nerve cells from free radicals generated by ischemic nerve injury through an antioxidant action, thereby promoting recovery
. Jung and Chi
and Jung
reported cases of symptom improvement upon high-dose steroid administration in patients with temporary neurogenic ptosis after reconstruction of orbital medial wall fracture. On the other hand, Ryu and Ahn
reported a case of postoperative ptosis that did not improve despite steroid treatment and required corrective operation. In our case, the patient was immediately treated with high-dose oral steroid for postoperative symptoms of ptosis and medial and superior rectus palsy. Although it is difficult to clarify whether recovery was spontaneous or due to the medication, patient recovery accelerated from one week of steroid administration. Despite the successful operation,such unexpected ptosis and extraocular muscle palsy can cause great physical and mental distress in patients, as well as being disconcerting for the surgeon. However, as most of these complications improve naturally over time, it is important to inform patients of the possibility before surgery and reassure patients during recovery. Administration of oral steroids can foster spontaneous recovery.
為了讓這個(gè)故事生動(dòng)有趣,我在細(xì)節(jié)處花了較多筆墨,人物對(duì)話(huà)也偏向幽默搞笑,孩子們讀得興致盎然,讀完后他們對(duì)“減少是為了增加”的人生哲學(xué)更加認(rèn)同了。
In conclusion, as seen in this case, ptosis and medial and superior rectus palsy after successful reconstruction of orbital medial wall fracture can be caused by ischemic injury of the oculomotor nerve branch by compression or traction during surgery, indicating the need for extra caution during operation.Although rare and temporary, such complications may occur unpredictably following a successful operation. Therefore,they should be considered important complications by both surgeons and patients.
四是建立了養(yǎng)護(hù)資金獎(jiǎng)補(bǔ)制度。市財(cái)政局會(huì)同市水務(wù)局印發(fā)了《天津市實(shí)行河道水生態(tài)環(huán)境管理地方行政領(lǐng)導(dǎo)負(fù)責(zé)制以獎(jiǎng)代補(bǔ)專(zhuān)項(xiàng)資金使用管理辦法》,制定了《河道水生態(tài)環(huán)境養(yǎng)護(hù)資金測(cè)算標(biāo)準(zhǔn)》。市級(jí)財(cái)政共安排河長(zhǎng)制管理專(zhuān)項(xiàng)資金6 043萬(wàn)元,其中以“以獎(jiǎng)代補(bǔ)”的方式補(bǔ)助各區(qū)縣堤岸水面保潔、水質(zhì)保護(hù)工作3 397萬(wàn)元,以獎(jiǎng)代補(bǔ)資金補(bǔ)助比例與考核成績(jī)掛鉤。各區(qū)縣的養(yǎng)護(hù)資金基本由市級(jí)財(cái)政、區(qū)縣級(jí)財(cái)政、街道辦事處、鎮(zhèn)政府以及區(qū)縣水務(wù)部門(mén)自籌組成。
None;
None.
1 Jung JW, Chi MJ. Temporary unilateral neurogenic blepharoptosis after orbital medial wall reconstruction: 3 cases.
2008;222(5):360-362.
2 Jung SK, Choi JA, La TY. Temporary severe neurogenic blepharoptosis after reconstruction of orbital medial wall fracture.
2011;52(9):1099.
3 Ryu SK, Ahn M. Postoperative neurogenic blepharoptosis after repair of a medial orbital wall fracture using the transcaruncular approach.
2011;52(5):624.
4 Kim TG, Shin JH. Spontaneous resolution of isolated neurogenic blepharoptosis after blunt trauma.
2018;97(44):e12988.
5 K?cker C, Wagner F, Caversaccio M, Anschuetz L. Horner syndrome as complication of acute sphenoid sinusitis.
2019;11(1):112-116.
6 Shen GX, Wu KJ, Chen Z, Gao YF, Nan GX. Sudden-onset unilateral ptosis induced by pituitary Macroadenoma, with false-positive jolly and neostigmine tests.
2018;32(2):295-298.
7 Bhatti MT, Eisenschenk S, Roper SN, Guy JR. Superior divisional third cranial nerve paresis: clinical and anatomical observations of 2 unique cases.
2006;63(5):771-776.
8 Derakhshan I. Superior branch palsy of the oculomotor nerve with spontaneous recovery.
1978;4(5):478-479.
9 Foroozan R. Transsphenoidal diplopia.
2004;49(3):349-358.
10 Song H, Lim SY, Park MC, Lee IJ, Park DH. Transient and isolated neurogenic blepharoptosis after medial orbital wall reconstruction.
2014;25(3):1106-1108.
11 Peter NM, Pearson AR. Orbital apex syndrome from blunt ocular trauma.
2010;29(1):42-44.
登錄APP查看全文
猜你喜歡
今日農(nóng)業(yè)(2022年15期)2022-09-20 06:56:20
股市動(dòng)態(tài)分析(2020年15期)2020-08-12 09:09:31
股市動(dòng)態(tài)分析(2020年14期)2020-08-12 09:09:12
股市動(dòng)態(tài)分析(2020年13期)2020-08-12 05:25:53
股市動(dòng)態(tài)分析(2020年12期)2020-08-12 05:25:33
股市動(dòng)態(tài)分析(2020年11期)2020-08-10 08:54:37
股市動(dòng)態(tài)分析(2020年10期)2020-08-10 08:53:55
建材發(fā)展導(dǎo)向(2019年10期)2019-08-24 06:26:30
建材發(fā)展導(dǎo)向(2019年10期)2019-08-24 06:26:20
雜文月刊(2016年1期)2016-02-11 10:35:51
 International Journal of Ophthalmology
2022年6期
International Journal of Ophthalmology
2022年6期
- International Journal of Ophthalmology的其它文章
- Intraocular lens removal or not during vitrectomy for acute infectious endophthalmitis after cataract surgery
- Vitreous function and intervention of it with vitrectomy and other modalities
- Short-term outcomes of mitomycin C-augmented excisional bleb revision with capsulectomy for failed Ahmed glaucoma valve
- Evaluation of nintedanib as a new postoperative antiscarring agent in experimental extraocular muscle surgery
- Multimodal imaging of experimental choroidal neovascularization
- A novel Nance-Horan syndrome mutation identified by next-generation sequencing in a Chinese family