Short-term outcomes of mitomycin C-augmented excisional bleb revision with capsulectomy for failed Ahmed glaucoma valve
2022-06-22 03:14:30BarDavidovShimonKurtzIlonaMohilevtsevaMichaelWaisbourdRonyRachmiel
INTRODUCTION
Glaucoma is the leading cause of global irreversible blindness worldwide, and poses a considerable public health threat
. The only method thus far proven effective in preventing the development of glaucomatous optic neuropathy or reducing its progression is lowering of intraocular pressure(IOP)
. The use of glaucoma drainage devices (GDDs) for refractory glaucoma has greatly increased worldwide during the last 20y
. Moreover, GDD surgery had lower failure rates and a decreased need for additional glaucoma surgery compared to trabeculectomy in the tube versus trabeculectomy(TVT) study, as well as failure rates similar to those of trabeculectomy in the Primary TVT study
. Failure rates of GDD implantation, however, were reportedly as high as 29.8%-53% in several large clinical trials, and bleb fibrosis with encapsulation leading to a hypertensive phase (HTP) was reportedly the main reason for uncontrolled high IOP after Ahmed glaucoma valve implantation (AGVI). Higher rates of HTP were reported in valved tubes, such as the Ahmed glaucoma valve (AGV), than in non-valved tubes, such as the Baerveld tube. Significantly higher levels of cytokines [
,transforming growth factor-β (TGF-β), chemokines CCL-2,CXCL1,
] and different types of interleukins were found in the aqueous from encysted blebs following tube shunt implants
. Their high concentration in cases of higher IOP levels suggests that their levels increase along with an increase in the IOP, and raises the possibility that encysted blebs form cytokines
. It is speculated that this higher rate is related to the stimulation of fibrosis by pro-inflammatory cytokines in the first aqueous humor, which is instantly filtered in valved shunts, such as the AGV, as opposed to a delayed filtration of ligated non-valved implants.
小區前面是一條八車道的寬闊馬路,出小區左拐數十米,便是一個交叉路口。或乘車,或步行,都要經過那里的紅綠燈。直行的綠燈,亮著,60秒后,切換為紅燈;左拐的綠燈亮起,30秒,然后切換。然后是交叉方向飄綠通行。然后又是直行的綠燈亮起,交替輪流,變換不息。
綜合以上對陳光明《馬克·吐溫幽默小品欣賞》譯本中的具體典例分析和效果賞析,我們將其方法歸納為以下兩點:
SUBJECTS AND METHODS
Pseudoexfoliative (PXF) glaucoma (
=5, 36%) was the most common form of glaucoma in our study group. It is typically a more aggressive type of glaucoma that requires more medications, glaucoma surgeries and subsequent revisions
.Its predominance in our study group might limit the real-world generalizability of the results.
This retrospective case series included adult patients with a failed superotemporal AGV (model FP7; New World Medical,Rancho Cucamonga, LA, USA) due to an encapsulated cyst.All patients underwent an ERC procedure at the Tel Aviv Medical Center (Tel Aviv, Israel) during a 3-year period(January 2017- December 2019) with a follow-up of at least 6mo.The preoperative evaluation and ocular examination included patients’ demographics, number of AGMs, indications for AGVI, best corrected visual acuity (BCVA) and IOP levels.The intraoperative evaluation included the documentation of complications and failures. Postoperative ocular examinations were scheduled at 1 and 7d, and 1, 3, and 6mo postoperatively. They included documentation of the postoperative complications, number of AGMs, the BCVA,and the IOP. Intraoperative complications were defined as tube truncation, intraocular hemorrhage and scleral perforation.Postoperative complications were defined as tube exposure or erosion, surgical wound leakage, hyphema, transient corneal edema, shallow anterior chamber, uveitis as well as visually devastating complications, including malignant glaucoma,endophthalmitis, persistent hypotony and suprachoroidal hemorrhage. AGV failure was defined when there was an IOP of ≥21 mm Hg despite optimal tolerated medical therapy.
There is no consensus on the management of uncontrolled high IOP after AGVI. Among the available options are aqueous suppressant glaucoma medications, such as beta blockers, carbonic anhydrase inhibitors, and alpha-2 agonists,which reduce the surface tension inside the bleb around the tube’s plate
. Lower pressure inside the bleb and lower surface tension may improve percolation of fluids through the formed capsule around the plate and thus reduce the cytokine production resulting from mechanical stress caused by increased IOP inside the bleb
. Surgical procedures aimed at lowering IOP after AGV failure include bleb needling,sequential insertion of a GDD and cyclophotocoagulation
.Since the capsule around the GDD plate is thick and impermeable, excisional bleb revision may offer a simple, less invasive and relatively safe alternative to the current surgical options. Data on the success and complications of ERC,however, are scant
. This study was designed to report the short-term outcome of ERC in the management of uncontrolled IOP due to encapsulation following AGVI by evaluating the success rate, change in IOP levels, number of anti-glaucoma medications (AGMs) and complications.
The excisional bleb revision with capsulectomy and mitomycin C (ERC) was performed under local anesthesia by topical oxybuprocaine hydrochloride 0.4% and subconjunctival injection of lidocaine 2%. A traction suture (Vicryl 6-0,Ethicon Limited, Edinburgh, UK with a BV needle, W9500)was used to rotate the globe inferiorly to improve visualization. A 4 mm incision was performed at the conjunctiva 8-9 mm from the limbus and 2 mm along the lateral nasal or temporal edge of the plate (Figure 1A). The underlying Tenon capsule was opened separately (Figure 1B). Careful hemostasis with cautery was conducted as needed. At least 50% of the entire capsular surface, including the area above the plate, was excised and removed using a crescent knife and Westcott scissors (Figure 1C). A careful dissection was needed to remove fibrovascular tissue from the valve outlet area and create a new space for future filtering. Balanced salt solution was injected into the tip of the tube by means of a 30G needle on a 1 mL syringe to evaluate tube flow and valve re-functioning. Viscoelastic material, sodium hyaluronate 1% (Biolon) was injected into the anterior chamber and retained there if shallowing was observed.Mitomycin C (0.15 mL, 0.4 mg/mL) was injected with a 1 mL syringe with a 27-gauge needle around the AGV plate and under the capsular remnant. It was irrigated 2min afterwards with balanced salt solution over the surgical area (Figure 1D).At the end of the procedure, the conjunctiva and Tenon capsule were carefully closed in 2 separate layers with 8-0 polyglactin sutures (Vicryl 8-0, Ethicon Limited, Edinburgh, UK; Figure 1E-1F). Vicryl 8-0 with a round head BV needle is strong enough to tightly close the Tenon and conjunctiva without leaks, buttonholes or subsequent inflammation. At the end of the operation, the patients received one drop of atropine 1%,dexamethasone 0.1% and ofloxacin 0.3%. The treated eye was patched with a plastic shield.
Only few studies have described the efficacy of shunt revision and capsule excision, with success rates ranging from 42%-75%
. Those studies had small numbers of patients,short follow-up periods and qualified success rates, similar to those in our study. However, they all differ from our study in their younger population (age range 37.6-57.9y), glaucoma types, number and types of previous surgeries, a higher baseline IOP (30-34 mm Hg), longer intervals between the AGVI and the ERC (1-3y), as well as the extent and location of capsule excision and the use of anti-fibrotic agents. The median age of our study group was 69.5y. We speculate that milder inflammatory reaction in the relatively older population might explain a higher success rate. A prospective comparative study is needed to validate this assumption.

Categorical variables were reported as numbers and percentages.Continuous variables were evaluated for normal distribution by means of histograms and reported as median and interquartile range (IQR). Changes in the IOP and number of medications during the follow-up were assessed with the Friedman test.The Wilcoxon signed ranks test was used to compare each time point to preoperative values. A Kaplan-Meier curve was used to describe surgical failure during the follow-up period. The univariate Cox regression was used to study the association between age and positive surgical outcome. The Mann-Whitney test was applied to compare the change in the IOP percentage between the female and male patients.Spearman’s rank correlation coefficient was employed to study the association between age and change in the IOP percentage.All statistical tests were 2-sided, and
<0.05 was considered statistically significant. SPSS software was used for all statistical analyses (IBM SPSS Statistics for windows, ver. 24,IBM corp., Armonk, NY, USA, 2016).
科研績效評價方面:第一,考核指標的權重分配是難點,權重的分配影響評價結果的準確性。第二,研究方法一般為定性分析或簡單定量研究,在數學模型基礎上展開績效評價的研究相對較少,在模型分析結果的基礎上展開對策研究的也不多見。第三,已有研究大多集中在高校科研傳統管理模式上,針對科研經費管理系統平臺的績效評價模塊研究較少。如何在科研經費管理系統的大數據環境下,逐步建立起合理準確的評價體系模塊也是本課題的研究重點。
RESULTS
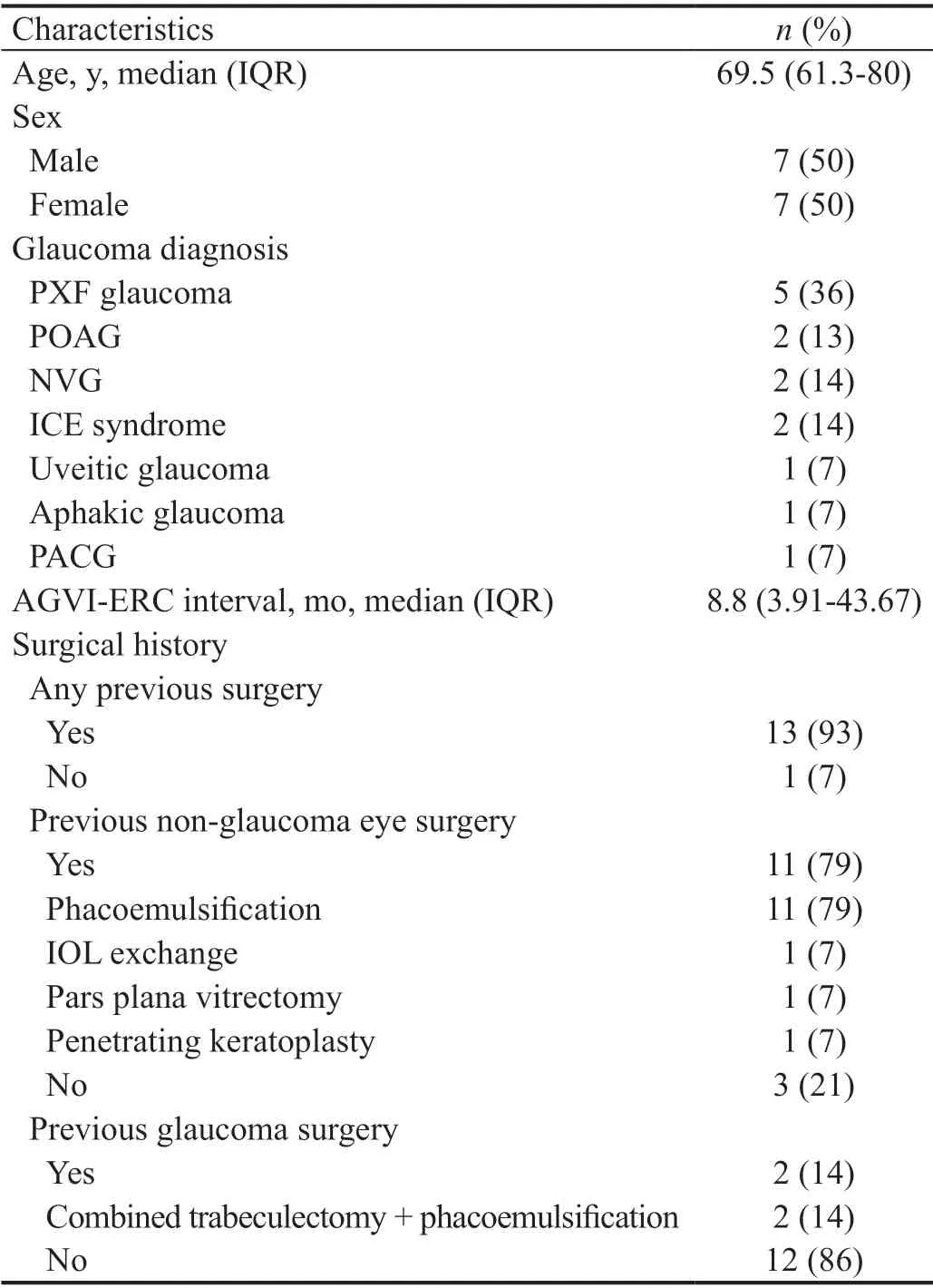
A total of 14 patients (14 eyes) of 7 males and 7 females whose median age was 69.5y (IQR 61.3-80y) underwent ERC during the study period. Patient demographics, including types of glaucoma and surgical history, are presented in Table 1.Pseudoexfoliative glaucoma (
=5, 36%) was the most common form of glaucoma. AGVI was the first ophthalmic surgery in one eye, while the other 13 had a history of ophthalmic surgery. AGVI was the first glaucoma surgery in 12 eyes(86%), while 2 eyes (14%) had a previous glaucoma procedure(both consisting of a combined cataract-trabeculectomy surgery; Table 1).
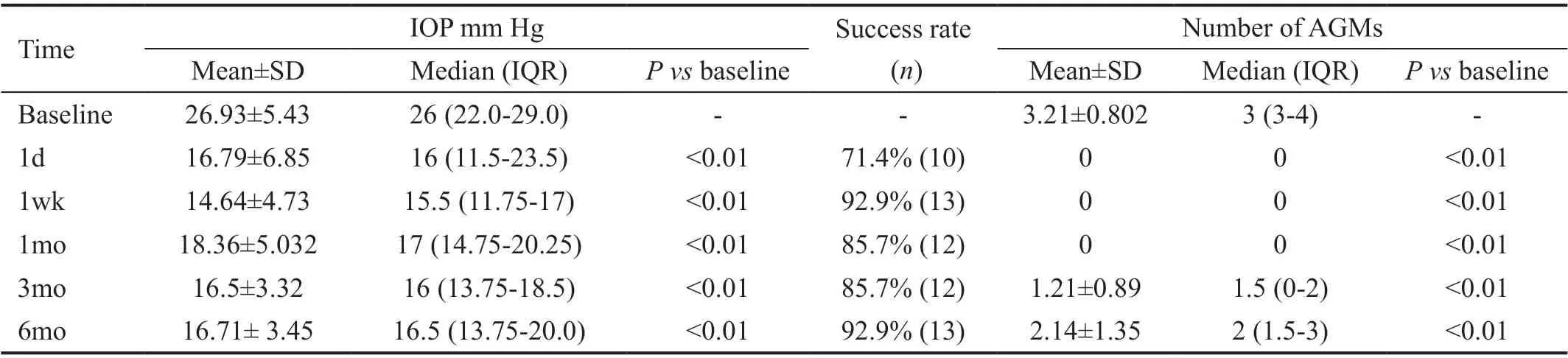
The median interval between AGVI to ERC was 8.8mo (IQR 3.91-43.67mo). The median IOP decreased from 26 mm Hg(IQR 22-29 mm Hg) to 16.5 mm Hg (IQR 13.75-20 mm Hg,
<0.01) at the 6-month follow-up (Table 2). The median number of AGMs decreased from 3 (IQR 3-4) to 2 (IQR 1.5-3,
<0.01) at the 6-month follow-up. The median IOP and the AGMs at baseline and during follow-up are presented in Table 2. Reduction in IOP levels and the number of AGMswas statistically significant at the 1- and 7-day, and 1-, 3- and 6-month follow-up visits (
<0.01).
There was no statistically significant change in the median BCVA. The median logMAR at the 6-month follow-up was 1.3(IQR 0.37-1.92) compared to 1.8 (IQR 0.37-2.3) at baseline(
<0.62). The ERC success rate was 71.4% (
=10), 92.9%(
=13), 85.7% (
=12), 85.7% (
=12), and 92.9% (
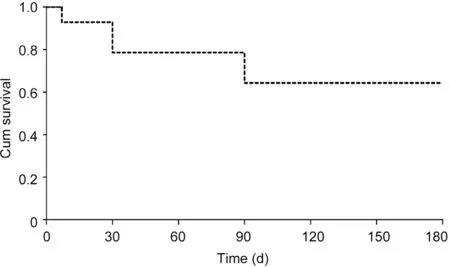
=13) at the 1- and 7-day, and 1-, 3- and 6-month follow-up visits,respectively (Table 2). The IOP at the 6-month follow-up had been maintained below 21 mm Hg without any AGMs in 3 eyes (21.42%). The Kaplan-Meier analysis of cumulative survival success for ERC is shown in Figure 2. The cumulative proportion of survival rate was 93%, 79%, 64%, and 64% at 1wk,and at 1, 3, and 6mo, respectively. We chose to omit the 1-day follow-up results in the Kaplan-Meier survival curve (Figure 2)since the IOP at that time is affected by various factors, such as lid edema, conjunctival injection and difficulties in measuring the IOP, none of which reflect surgical outcome.
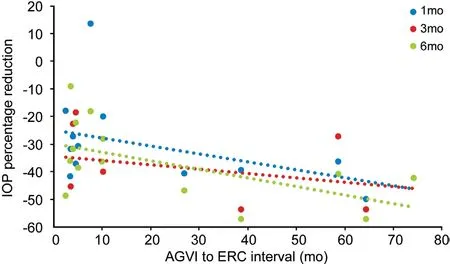
At the 6-month follow-up, there was no correlation between the IOP percentage reduction and sex (
=0.26), the BCVA at admission (
=0.807), age (
=0.76), the number of glaucoma medications at baseline (
=0.167), or the IOP at baseline(
=0.025). Although not statistically significant, a higher IOP percentage reduction at 1mo (
=-0.508,
=0.063) and at 6mo(
=-0.486,
=0.078) tended to be associated with a longer interval between AGVI and ERC (Table 2 and Figure 3).
Several studies have shown that AGV is safe and effective in reducing IOP in patients with primary, secondary, and refractory glaucoma
. Following a short-lived normal tension phase lasting from 7 to 10d, early IOP rise (so-called “hypertensive phase”) is a common phenomenon after GDD implantation,appearing in 30%-80% of cases
. Inadequate IOP control and bleb fibrosis were found in the Ahmed versus Baerveldt study to be more common in the AGV, as a valved GDD, than in the Baerveldt glaucoma implant
. It was speculated that the higher rate of increased IOP is related to the stimulation of fibrosis by pro-inflammatory cytokines in the initial flow of aqueous humor, which is immediately filtered in valved shunts as opposed to the delayed filtration of ligated non-valved implants
. In addition, the smaller plate surface of the AGV is more susceptible to restriction by fibrotic tissue
. Aqueous humor contains various growth factors and pro-inflammatory cytokines, such as the TGF-β, the basic fibroblast growth factor(bFGF), epidermal growth factor (EGF), insulin-like growth factor-1 (IGF-1), chemokines (CCL-2, CXCL1,
) and different types of interleukins
. These cytokines contribute to the wound-healing response, serving as chemotactic or mitogenic factors for fibroblasts forming a capsule
. The collagen-rich capsule is responsible for the major resistance to aqueous humor flow through GDD. The postoperative IOP is poorly controlled by a thicker bleb
. Significantly higher levels of cytokines were found in aqueous humor retrieved from encysted blebs following tube shunt implants in which the IOP was higher, suggesting that their levels increase with an increase in the IOP
. It was also suggested that encysted blebs produce cytokines
.
參與本次實驗的1424例冠心病患者所有數據均行SPSS17.0軟件處理,診斷準確率、靈敏度、特異度對比用率(%)的形式表示,行卡方檢驗,當數據對比呈現為P<0.05的差異性時,統計學意義存在。
DISCUSSION
The findings of this retrospective, non-comparative, interventional case series study demonstrated the short-term effectiveness and safety of an ERC procedure designed to decrease the IOP in cases of AGV failure. The median IOP and number of AGMs was significantly decreased. The success rate at 6mo was 92.9%. No intraoperative complications and mild postoperative complications were identified and resolved spontaneously during the first week of follow-up.
The literature on doses and modes of application of Mitomycin C in glaucoma procedures is sparse
. There are a few therapeutic techniques to remedy GDD failure as a result of excessive fibrosis. The most common management starts with AGMs when the IOP begins to rise above 15 mm Hg
,although there is evidence of benefits starting even as early as 10 mm Hg
. Aqueous suppression medications, such as topical acetazolamide, alpha-2 agonists, and beta blockers are then administered. A surgical procedure is needed when the IOP is still above target. Bleb needling with an antifibrotic agent, such as mitomycin C or 5-fluorouracil (5-FU),is a simple procedure which can be performed in an office setting. However, the reported results are disappointing and the procedure usually has to be repeated
. Placement of a second GDD in the sub-Tenon or supra-Tenon space is a common management approach in the case of initial shunt failure
.A second tube is usually placed in the lower quadrants of the eye globe, and the reported success rate is 59%-92.9% after 1y of follow-up
. However, there is a high rate of corneal decompensation (16%-45%). Cyclophotocoagulation with a diode laser is a procedure usually carried out on advanced or end-stage glaucoma patients
. It is a procedure with unpredictable results and bears its own risks of visual acuity deterioration, hypotony and phthisis bulbi, and is therefore usually reserved as a last resort.
地勘單位測繪成果使用與保密管理工作的探討(陳曉芳) .............................................................................5-35
There were no intraoperative complications. None of the eyes were re-operated for glaucoma during the 6 postoperative months. Five of the 14 eyes (43%) exhibited early postoperative complications, including transient corneal edema (4 eyes, 28.6%) which might be explained by the corneal traction suture pulling the eye or possible mild erosion by the plastic drape while the eye was rotated downwards, and transient shallow anterior chamber which might be due to over filtering at the space created around the plate immediately following the surgery (one eye, 7.14%).All of these complications resolved spontaneously during the first week following revision. There were no tube or plate exposures as well as no leaks due to the tight tenon and conjunctival closure. No visually devastating complications,such as endophthalmitis, persistent hypotony, phthisis bulbi or deterioration of visual acuity to no light perception were observed during the follow-up.
To address this problem of scarring and dense capsule formation around a well-functioning GDD, the required procedure should involve a safe excision of the dense capsule combined with application of an anti-fibrotic agent
, such as mitomycin C
, to prevent recurrent fibrosis. We injected 0.15 mL of 0.4 mg/mL mitomycin C at the site of the excised capsule followed by a 2-minute wash with saline solution.
要借鑒建設項目水資源論證的工作實踐和經驗,吸收各級水行政主管部門的管理人員、科研人員及建設項目水資源論證從業人員以及社會各方力量,組織規劃水資源論證隊伍和專家隊伍,搭建規劃水資源論證技術交流平臺。……
登錄APP查看全文
猜你喜歡
辦公室業務(2020年18期)2020-09-29 12:15:58
勞動保護(2019年7期)2019-08-27 00:41:26
領導決策信息(2018年50期)2018-02-22 06:17:16
商周刊(2017年5期)2017-08-22 03:35:26
中國衛生(2016年2期)2016-11-12 13:22:16
中國商論(2016年33期)2016-03-01 01:59:53
中國工程咨詢(2016年4期)2016-02-14 07:28:28
中國鄉鎮企業會計(2015年9期)2015-12-30 16:47:21
中國工程咨詢(2015年5期)2015-02-16 05:35:26
體育師友(2011年5期)2011-03-20 15:29:53
 International Journal of Ophthalmology
2022年6期
International Journal of Ophthalmology
2022年6期
- International Journal of Ophthalmology的其它文章
- Intraocular lens removal or not during vitrectomy for acute infectious endophthalmitis after cataract surgery
- Vitreous function and intervention of it with vitrectomy and other modalities
- Evaluation of nintedanib as a new postoperative antiscarring agent in experimental extraocular muscle surgery
- Multimodal imaging of experimental choroidal neovascularization
- A novel Nance-Horan syndrome mutation identified by next-generation sequencing in a Chinese family
- Procollagen C-proteinase enhancer 1 promotes physiologic retinal angiogenesis via regulating the process of collagen