Periorbital necrotizing fasciitis accompanied by sinusitis and intracranial epidural abscess in an immunocompetent patient
2022-05-15 05:40:42SuYounSuhJungHyoAhn
Dear Editor,
We have presented the unusual case of periorbital necrotizing fasciitis (NF) coexisting with sinusitis and intracranial epidural abscess in a healthy young patient that was successfully managed with medical and surgical treatments. The authors obtained informed consent in person and adhered to the tenets of the Declaration of Helsinki.
其中indexSy(T′(y),0)是在空間Sy上線性算子T′(y)在0點的指標,σ是T′(y)在Sy上的大于1的特征值的代數重數之和。
Periorbital NF is a rapidly progressive and potentially lifethreatening soft tissue infection characterized by extensive necrosis and gas formation in the fascia and subcutaneous tissue. Periorbital NF usually occurs in traumatic injuries,in postsurgical wounds, and under immunocompromised conditions, such as advanced age, diabetes mellitus, human immunodeficiency virus (HIV) infection, alcohol abuse,chronic renal failure, and chemotherapy for malignancies.It has also been reported in healthy patients
. Previous studies on periorbital NF have reported precipitating events such as blunt trauma or penetrating injury, blepharoplasty,dacryocystorhinostomy, tooth extraction, retrobulbar injection,and dexamethasone intravitreal injection
. However,there have been rare reports of periorbital NF associated with sinusitis, extended into the epidural space in the immunocompetent patients
.
A 43-year-old male patient visited our Emergency Center with complaints of a right painful lid swelling and headache that started a day earlier. He had no chronic disorder,such as diabetes mellitus, HIV infection, alcoholism, and systemic malignancy. Further, he had no history of trauma or surgery. He was receiving intermittent treatments for chronic sinusitis for over 5y. His vital signs were 142/76 mm Hg(blood pressure), 86 beats per minute (heart rate), 18 breaths per minute (respiratory rate), and 36.2℃ (body temperature).The white blood cell count and C-reactive protein level were 19.4×10
/L (normal: 4-11×10
/L) and 20.68 mg/dL(normal: 0-0.5 mg/dL), respectively, indicating severe acute infection or inflammation. Erythrocytes sedimentation rate(ESR) was 6 mm/h (normal: 0-10 mm/h). Furthermore, we performed the systemic evaluation to exclude the sinusitis related to autoimmune disease. The chest radiograph and abdomen computed tomography were normal. Serologic tests such as antineutrophil cytoplasmic antibodies (ANCA) and angiotensin converting enzyme (ACE) showed no abnormality.We admitted the patient and initiated empirical intravenous antibiotic treatment (ceftriaxone, vancomycin, metronidazole).His best-corrected visual acuity was 20/20 in the left eye, but it could not be examined for the right eye because of the severe erythematous swelling of the eyelid. No abnormality was found on B-scan ultrasonography of the right eye.
依那西普聯合環磷酰胺對類風濕性關節炎合并間質性肺炎患者相關指標的影響 ………………………… 陳良敏等(2):236
OPNET采用離散事件驅動的模擬機理和混合建模機制,并提供了包括模型設計、仿真和統計量收集、分析的各種研究工具,同時它還引入了面向對象的編程技術。OPNET的特點是建模方便,功能強大,尤其是在大規模網絡模擬中表現卓越。

The patient was diagnosed with periorbital NF accompanied by sinusitis and intracranial epidural abscess. We performed an emergent surgical debridement with the cooperation of the neurosurgery and otolaryngology teams. First, the epidural abscess connected to the right frontal sinus was identified and extensively debrided using craniotomy. Second, large amounts of the abscess were drained from the right ethmoid, sphenoid,and maxillary sinuses using endoscopic sinus surgery. Finally,debridement of the necrotic skin and soft tissues in the eyelid was performed. Culturing the specimens from the brain, sinus,and eyelid revealed
as the causative agent. Therefore, the empirical antibiotic regimen was replaced with ampicillin, to which
is highly susceptible.Eyelid swelling and purulent discharge from the wound decreased gradually after frequent wet dressing. The visual acuity of the patient’s right eye was preserved at 20/20. A skin graft was successfully performed a month after the surgery(Figure 3). There were no other complications in the brain,orbit, and sinuses. At 2y after surgery, there was no evidence of recurrence of the orbital cellulitis and sinusitis.
In our case, periorbital NF was provoked by sinusitis extending to intracranial epidural abscess in a healthy young male patient.He had suffered from chronic sinusitis for >5y. It is presumed that the chronic sinusitis abruptly induced periorbital NF and spread into the intracranial epidural abscess through a bony defect in the frontal sinus wall.

The causative organism in periorbital NF is usually Group A β-hemolytic
, occasionally in combination with
. However, the pathogen in our case was
, a member of the
group.
group organisms are commonly found on the mucous membrane of the oropharyngeal and upper respiratory tract. However, they can be aggressive pathogens with a propensity for abscess formation and periocular extension of the infection after mucosal disruption.
(3)根據現場遺留物及被撞車輛痕跡、人體痕跡等推斷逃逸車輛裝載物、接觸部位和損壞部位,從而使追擊、堵截工作更具針對性。
In previous studies, approximately 47% patients with periorbital NF were healthy without any underlying comorbidities
.In several case reports, periorbital NF was also triggered by infections such as dacryocystitis, sinus infection, carbuncle,pneumonia, and parotid gland infection
.
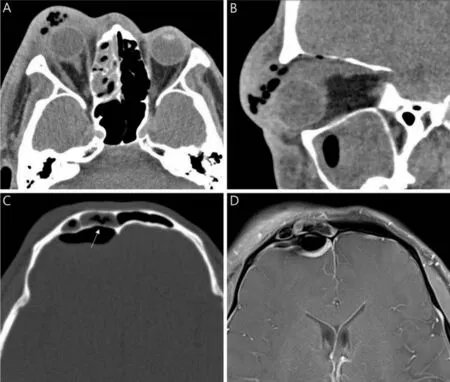
Eyelid skin necrosis and pus developed a day after admission(Figure 1). Orbital computed tomography (CT) revealed marked swelling and increased fat infiltration with gas bubbles in the right eye accompanied by ethmoid and sphenoid sinusitis. In addition, the sagittal CT view showed maxillary sinusitis with air bubbles, whereas the coronal CT view revealed pneumocephalus with a suspicious bony defect at the frontal sinus wall. Brain magnetic resonance imaging showed frontal sinusitis at the posterior surrounding minimal fluid collection within the right epidural space, which represented an epidural abscess (Figure 2).
The major morbidities of periorbital NF are loss of vision,meningitis, and other neurological disorders; death may also occur. However, we prevented blindness and an escalation to meningitis, toxic shock, or multiorgan failure by prompt surgical debridement and drainage of the abscess with administration of systemic intravenous antibiotics.
In conclusion, we have presented a rare case of periorbital NF accompanied by sinusitis and intracranial epidural abscess in an immunocompetent patient with no history of trauma or surgery. The fact that patient was immunocompetent is actually in favor of good recovery of the patient without loss of vision or any systemic complications.
None;
None.
1 Amrith S, Pai VH, Ling WW. Periorbital necrotizing fasciitis —a review.
2013;91(7):596-603.
2 Lazzeri D, Lazzeri S, Figus M, Tascini C, Bocci G, Colizzi L, Giannotti G, Lorenzetti F, Gandini D, Danesi R, Menichetti F, del Tacca M, Nardi M, Pantaloni M. Periorbital necrotising fasciitis.
2010;94(12):1577-1585.
3 Danan J, Heitz A, Bourcier T. Periorbital necrotizing fasciitis following dexamethasone intravitreal implant injection.
2016;134(1):110-111.
4 Jeong HM, Jun KH, Lee SH, Lee JH. A case of periorbital necrotizing fasciitis occurred in a diabetes mellitus patient accompanied with chronic sinusitis with nasal polyp.
-
2014;57(3):194.
5 Luksich JA, Holds JB, Hartstein ME. Conservative management of necrotizing fasciitis of the eyelids.
2002;109(11):2118-2122.
6 Sud R, Sharma P, Garg G, Takkar B, Khanduja S. Periorbital necrotizing fasciitis due to Klebsiella pneumoniae in an immunocompetent patient.
2019;67(10):1721-1722.
7 Lin PW, Lin HC. Facial necrotizing fasciitis following acute dacryocystitis.
2003;136(1):203-204.
8 Akcay EK, Cagil N, Yulek F, Anayol MA, Cetin H, Cag Y, Altintas AGK, Simsek S. Necrotizing fasciitis of eyelid secondary to parotitis.
2008;18(1):128-130.
9 Comaish I, Thaller V, Newman P. Necrosis of the lid due to Pseudomonas aeruginosa.
(
) 2000;14 (Pt 3A):387-389.
登錄APP查看全文
 International Journal of Ophthalmology
2022年5期
International Journal of Ophthalmology
2022年5期
- International Journal of Ophthalmology的其它文章
- Multimodal imaging in immunogammopathy maculopathy secondary to Waldenstrom’s macroglobulinemia: a case report
- Multimodal imaging in Purtscher-like retinopathy associated with sarcoidosis: a case report
- Can a sneeze after phacoemulsification cause endophthalmitis? A case report
- Persistent macular oedema following Best vitelliform macular dystrophy undergoing anti-VEGF treatment
- Genetic, environmental and other risk factors for progression of retinitis pigmentosa
- lnflammation and dry eye disease—where are we?