Tuberculous pericarditis-a silent and challenging disease:A case report
2022-03-18 02:16:36OscarDavidLuceroMarlonMauricioBustosDarwinJhoanArizaRodrguezJuanCamiloPerez
World Journal of Clinical Cases 2022年6期
lNTRODUCTlON
Tuberculosis(TB)is a transmissible disease and it is the main cause of morbimortality and one of the ten leading causes of death worldwide.It is also the leading cause of death from a single infectious agent[ahead of human immunodeficiency virus(HIV)/AIDS].A quarter of the world’s population is infected withand thus is at risk of developing the disease[1].In developing countries,coinfection with the HIV is associated with a higher mortality[2].Although the lung is the target organ for TB,any other organ can be affected.Extrapulmonary TB accounts for 10%-20% of the clinical presentation suffered by immunocompetent patients[3].Approximately 1% to 2% of patients with pulmonary TB have tuberculous pericarditis(TP)and this carries a high mortality rate(17% to 40% over 6 mo)[4].
Pericarditis can be caused by infectious agents(,viral and bacterial)or can be non-infectious in origin(,systemic inflammatory diseases,cancer,and post-cardiac injury syndromes).TB is a major cause of pericarditis in developing countries,but accounts for less than 5% of cases in developed countries,where viral causes are responsible for 80% to 90% of the cases[5].TP accounts for approximately 4% of acute pericarditis,7% of cardiac tamponade and 6% of constrictive pericarditis cases[6].usually affects the pericardium by retrograde lymphatic spread from the peritracheal,peribronchial,or mediastinal lymph nodes or by hematogenous spread of a primary TB infection and is rarely affected by contiguous spread of a tuberculous lesion in the lung or hematogenous spread of a distant focus[7].
CASE PRESENTATlON
Chief complaints
A 49-year-old woman came to the emergency room for unquantified fever peaks and intermittent chest pain lasting 2 mo.
History of present illness
Unquantified fever peaks and intermittent chest pain lasting 2 mo which increased in intensity.
Peter promised faithfully he wouldn t, and the old woman continued: This evening at sunset go to yonder pear-tree which you see growing at the cross roads
History of past illness
Written consent was provided by the patient.
Personal and family history
The patient had a surgical history of liposuction and augmentation mammoplasty.
Physical examination
The first visit he paid was to the hyaenas, who trembled at the sight of him, and whispered to each other, How shall we escape from this terrible beast? Meanwhile the little hare did not trouble himself about them, but just asked where the king of the hyaenas lived, and made himself quite at home there
I had a complete mastectomy and the cancer has not spread to any other part of my body. The doctors told me if the cancer had gone undetected even six more months, it would have been too late.
Laboratory examinations
Electrocardiogram was done(Figure 1)and showed sinus tachycardia and low-voltage complexes in the limb and precordial leads.There were no alterations in PQ interval or ST-segment.Deaminase level in the pericardial fluid of 36.50 U/L(reference range,0 to 9 U/L).The cytology of the pericardial fluid was of lymphocytic predominance and examination of the pericardial fluid revealed acid-fast bacilli.Polymerase chain reaction(PCR)study of pericardial fluid was positive for.

Imaging examinations
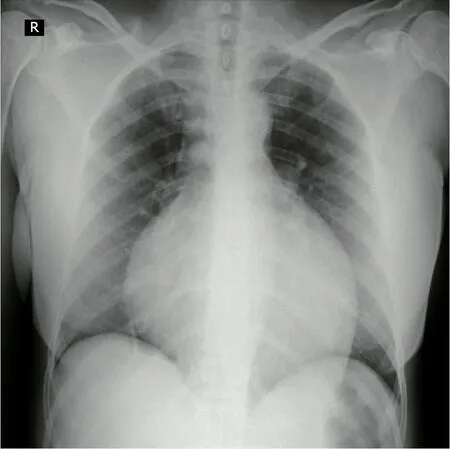
Chest x-ray was done(Figure 2)showing a generalized increase of the mediastinal cardiac silhouette,suggestive of pericardial effusion.There was an adequate pulmonary vascularization pattern.Pleuropulmonary lesions were not seen.Transthoracic echocardiography revealed a large and free-looking pericardial effusion,with an anterior interface of 17 mm and a posterior interface of 27 mm.The right cavities had a partial diastolic collapse,between 20%-30%(Figure 3).High-resolution chest tomography revealed a heart of normal size and there was evidence of pericardial effusion without alteration of the ventricular walls with a thickness of up to 25 mm(Figure 4).


MULTlDlSClPLlNARY EXPERT CONSULTATlON
TP was made.HIV was negative.
FlNAL DlAGNOSlS
Tuberculous pericarditis.
TREATMENT
The patient received treatment each day with isoniazid 300 mg,rifampin 600 mg,pyrazinamide 1600 mg,and ethambutol 1100 mg for 2 mo.This was followed by rifampin and isoniazid for an additional 4 mo along with prednisolone for 6 wk.
The authors have no conflict of interest.
Treatment of TP is based on the use of rifampicin,isoniazid,pyrazinamide,and ethambutol for 2 mo,followed by isoniazid and rifampicin(a total of 6 mo of treatment)[22].The effectiveness of treatment with corticosteroids in TP remains controversial.Steroids have not yet been found to have overwhelming beneficial effects on reabsorption of pericardial effusion or in the progression to constrictive pericarditis[23].
OUTCOME AND FOLLOW-UP
In the days following pericardiocentesis and initiation of tetraconjugate management for TB,the patient progressed satisfactorily with improved hemodynamic parameters and fever resolution.
DlSCUSSlON
TP has a diverse clinical picture and should be considered in the evaluation of non-self-limiting pericarditis cases.Despite the fact that the prevalence of TB has been reduced in general,the cases of extrapulmonary TB remains stable;approximately 1050000 new cases were reported in the world in 2018[8].In developing countries,one to two percent of pulmonary TB patients develop TP.However,it can also appear as an isolated extrapulmonary form[9].There are few studies that evaluate the prevalence of TP in Colombia,and generally,it is considered that there is an underdiagnosis of the disease.13626 new cases of TB were reported during 2020,of which 83% corresponded to pulmonary TB and 17% to extrapulmonary TB,while 1.6% of these corresponded to TP[9].Furthermore,in Colombia,a progressive increase in the extrapulmonary TB rate has been observed:2.1 cases/100000 inhabitants in 1997;3.7/100000 in 2006 and 4.4/100000 in 2018.Less than 1% of these cases correspond to TP,and generally,it occurs in patients coinfected with HIV who constitute about 85% of cases[10].
TP usually develops insidiously and with nonspecific systemic symptoms such as fever,night sweats,fatigue and weight loss.Although chest pain,cough,and dyspnea are common,the severe acute-onset pericardial pain characteristic of idiopathic pericarditis is rare[10].Large pericardial effusion should be suspected when micro voltage is observed on the electrocardiogram.This is seen in complexes < 5 mm in the limb leads and < 10 mm in the precordial leads[11].Chest radiography generally shows a widening of the cardiac silhouette in more than 90% of cases,with a globular image described as “Bottle of water” configuration.Generally,these findings are observed in conjunction with active lung TB and pleural effusion in 30% and 60% of cases,respectively[12].On the echocardiogram,TP usually comes accompanied by pericardial effusion with thickening of the visceral pericardium and it is possible to identify fibrin bands or fibrosis that heals the pericardium[13].
TP diagnosis is confirmed if one of the following criteria is present:Positive culture for the bacillus of Koch in pericardial fluid,positive direct examination for Koch bacillus,or value greater than 50 IU/L on the Adenosine deaminase(ADA)test[14].Furthermore,the diagnosis can be confirmed if the pericardial biopsy shows the following findings:Positive culture for the Koch bacillus and granulomas with caseous necrosis,or presence of Langhans-type multinucleated giant cells,or presence of tubercle bacilli in the sample[15].
The patient was febrile with a temperature of 39.5 °C.Her heart rate 117 beatsminute,blood pressure 100/60 mmHg,respiratory rate of 24 breathsminute and her oxygen saturation was 80%.The patient’s neck veins were distended and heart sounds were muffled.
The authors have read the CARE Checklist(2016),and the manuscript was prepared and revised according to the CARE Checklist(2016).
Pericardial ADA levels ≥ 35 U/L are diagnostic of TP with a sensitivity and specificity of 90% and 74%,respectively[20].On the other hand,it has been shown that IFN-γ,which is produced by CD-4 +and CD-8 + T lymphocytes in the context of TP,could be a precise diagnostic biomarker[21].
How lofty the houses seemed, and what a number of people there were in the streets! some pushing this way, some that- a perfect maelstrom of citizens and peasants, monks and soldiers- the jingling of bells on the trappings of asses and mules, the chiming of church bells, calling, shouting, hammering and knocking- all going on at once
CONCLUSlON
TP occurs in 1%-2% of patients with pulmonary TB and carries a high mortality rate.The diagnosis of TP remains difficult due to the absence of a simple,rapid and accessible diagnostic test despite its associated morbidity and mortality.Treatment of TP consists of rifampicin,isoniazid,pyrazinamide,and ethambutol for 2 mo,followed by isoniazid and rifampicin(total of 6 mo of therapy).Early diagnosis of this entity will allow physicians to initiate timely treatment,avoid complications and improve the patient’s clinical outcome.
FOOTNOTES
Bustos MM participated in the conception of the work and review of the final version;Lucero OD contributed to the conception of the work and the preparation of the manuscript;Ariza Rodríguez DJ participated in the preparation of the manuscript and the bibliographic review;Perez JC participated in the design of the work and analysis;all authors have read and approved the final manuscript.
During the 2 wk prior to admission,the patient experienced dyspnea,cough and hyaline expectoration.
The very minute that the compact with the devil had come to an end his beard was shaved, his hair was cut, and his rags were burned, and day and night he lay in a bath of clear warm water
The diagnosis of TP remains difficult due to the absence of a simple,rapid and accessible diagnostic test despite its associated morbidity and mortality.A protein-rich lymphocytic exudate that is often grossly hemorrhagic is a typical finding in the pericardial fluid.However,the TP fluid is paucibacillary and the estimated diagnostic accuracy based on the smear is only 5%[16].The sensitivity of pericardial fluid culture ranges from 53% to 75%[17].However,results are obtained in an average of 3 wk.PCR test forDNA or RNA in pericardial fluid is more accessible and faster,and it has a lower cost than pericardial tissue PCR,but it also has a lower sensitivity(15%80% respectively),and can yield up to 20% false positives[18].PCR has been very useful since it is capable of identifying different nucleic acid sequences in samples with low bacilli concentrations and in addition,it identifies resistance to rifampicin encoded in thegene,which can be useful in settings where there is a high prevalence of multidrug-resistant TB.Finally,in recent years,the performance of the immunoassay has been studied which quantifies the release of interferon gamma(IFN-γ)(QuantiFERON?,ELISpot)for the diagnosis of pulmonary TB,extrapulmonary TB and latent TB.The sensitivity of pericardial biopsy varies from 10% to 64%[19].
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:http://creativecommons.org/Licenses/by-nc/4.0/
The girl had to ride for a great many days, and for a long and wearisome time, before she got there; but at last she did arrive, and then she asked the East Wind if he could tell her the way to the Prince who dwelt east of the sun and west of the moon
No wonder the shoemaker becomes wealthy with so many pairs of shoes to sell so quickly! No doubt the elves can easily make 512 pairs of shoes just as easily as 2 since they are magical beings
Colombia
Oscar David Lucero 0000-0002-4100-3529;Marlon Mauricio Bustos 0000-0002-1746-6398;Darwin Jhoan Ariza Rodríguez 0000-0003-2852-4669;Juan Camilo Perez 0000-0003-3332-248X.
Fan JR
Filipodia
As soon as he had got into the court-yard, he moved very softly, and theladies were so much engrossed21 with counting the kisses, that all might go onfairly, that they did not perceive the Emperor. He rose on his tiptoes.
Fan JR
 World Journal of Clinical Cases2022年6期
World Journal of Clinical Cases2022年6期
- World Journal of Clinical Cases的其它文章
- Vaginal enterocele after cystectomy:A case report
- Acute kidney injury due to intravenous detergent poisoning:A case report
- Bilateral pneumothorax and pneumomediastinum during colonoscopy in a patient with intestinal Behcet’s disease:A case report
- Successful embolization of an intrahepatic portosystemic shunt using balloon-occluded retrograde transvenous obliteration:A case report
- lmplant site development using titanium plate and platelet-rich fibrin for congenitally missed maxillary lateral incisors:A case report
- Primary duodenal dedifferentiated liposarcoma:A case report and literature review