Antegrade in situ laser fenestration of aortic stent graft during endovascular aortic repair:A case report
2022-03-15 07:12:28ZhiWeiWangZhenTaoQiaoMingXingLiHuaLongBaiYuanFengLiuTaoBai
World Journal of Clinical Cases 2022年4期
INTRODUCTION
An inadequate proximal neck is the most common anatomical challenge during the endovascular repair of juxtarenal abdominal aortic aneurysms (JAAAs)[1].Retrograde in situ fenestration (ISF) has been reported to preserve the major aortic branches during thoracic endovascular aortic repair (TEVAR) effectively and safely[2];however,because of the lack of downstream branch artery access,retrograde revascularization cannot be achieved easily in EVAR without a laparotomy or retroperitoneal incision[3-5].If endovascular therapy is deemed to be the best treatment option,antegrade ISF may be an ideal method to preserve the patency of visceral arteries.Many animal experiments[6-9],benchtop studies[10-12],and clinical studies[13-17] have demonstrated that the antegrade ISF of aortic stent grafts during EVAR is technically feasible.The following report describes a novel approach of antegrade in situ laser fenestration (ISLF) during EVAR.We found that the ostium of the right renal artery (RRA) could be accurately positioned by angiography in real time.Moreover,RRA perfusion could be maintained during the procedure.
CASE PRESENTATION
Chief complaints
A 55-year-old man presented to the emergency department of our hospital complaining of worsening lower abdomen pain.
34. A regular blow-out: Blow-out is a colloquialism97 from the UK meaning An excessive spree of drinking, eating, spending or sex (Duckworth 2003). Andrew Lang considers phrase this to be an example of Hansel s vulgarity in a footnote to the story in The Blue Fairy Book.
History of present illness
The patient’s symptoms started a week prior with recurrent episodes of lower abdomen pain and distention,which had worsened in the last 4 h.The patient had no fever or diarrhea.Color Doppler ultrasound in a community hospital showed an abdominal aortic aneurysm (AAA).
History of past illness
The patient had a clear previous medical history.
Personal and family history
The abdomen was soft,with mild periumbilical tenderness and no rebound tenderness.A pulsatile abdominal mass could be palpated.The liver and spleen were impalpable.
Physical examination
However,he had smoked at least five cigarettes a day for ten years.
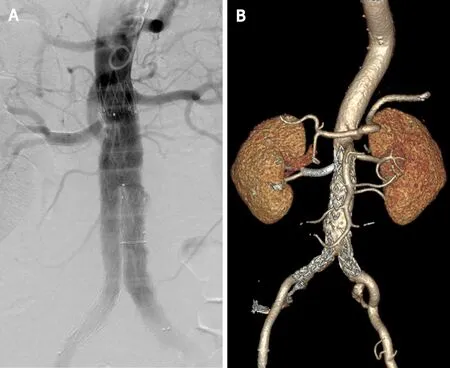
The patient had an uneventful recovery and was continued on aspirin daily.The total procedure time was 2 h.The fluoroscopy time was 45 min,and the total amount of contrast used was 100 mL.The estimated blood loss was 20 cc.Because the left renal artery was not involved,RRA perfusion was maintained during the operation.Postoperatively,there was no abnormal renal function,and the patient was discharged home on postoperative day 7.The 1-year follow-up CTA confirmed patency the of both renal arteries and the absence of endoleakage (Figure 3B).
Laboratory examinations
The patient’s blood pressure was approximately 108/80 mmHg.The blood routine examination findings were normal.The prothrombin and partial thromboplastin times were normal,and the D-dimer level was slightly increased,at 0.47 mg/L.The serum C-reactive protein level was increased,at 66.48 mg/dL (normal range:<5 mg/dL),and the erythrocyte sedimentation rate was 23 mm/h.The results of blood biochemistry,urinalysis,electrocardiography and arterial blood gas analysis were also normal.
Confirmed JAAA combined with PAUs.
Imaging examinations
After a thorough patient evaluation,we discussed the possible treatment alternatives.The PAUs involved the RRA,so open surgery was likely to be more traumatic and technically complex than traditional infrarenal repair[18].EVAR has been widely accepted as the treatment of choice for patients who are unfit for open surgery.To achieve an adequate proximal seal,the RRA might need to be covered and then revascularized."Off-the-shelf" techniques (such as chimney,periscope,and sandwich techniques) have a high risk of type IA endoleakage and reintervention and are thus not preferred.Customized fenestrated and branched endografts are expensive and not available for the treatment of acute syndromes.Even physician-modified stent grafts still need to be rotated and moved as needed for cannulation of the visceral vessels.In this case,the enhanced abdominal pain and thick perivascular hematoma suggested that the risk of aneurysm rupture was high.Therefore,for early and minimally invasive treatment,after obtaining informed consent,EVAR with antegrade ISF was planned.
MULTIDISCIPLINARY EXPERT CONSULTATION
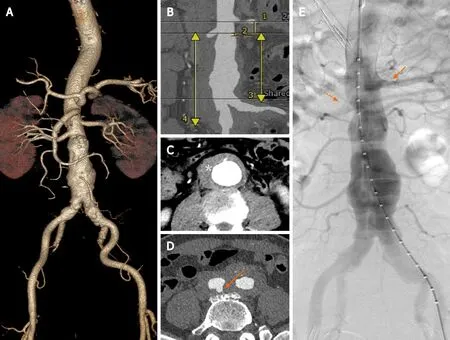
Preoperative computed tomography angiography (CTA) showed a JAAA with a diameter of 50.4 mm,a thick hematoma and multiple penetrating aortic ulcers (PAUs).Preoperative sizing showed an aortic ulcer with a hematoma below the right renal ostium,a short (4-mm-long) infrarenal aortic neck,and a proximal healthy landing zone of approximately 16.0 mm between the two renal arteries.The diameter of RRA was 6.1 mm.The diameter of the aortic bifurcation was 32 mm.The diameter of the vessel at the lower edge of the left renal artery was 20.9 mm.The diameter of the vessel at the lower edge of the RRA was 20.5 mm.The distance from the lower edge of the RRA to the aortic bifurcation was 91.2 mm.The distance from the lower edge of the RRA to the bifurcation of the right iliac artery was 124.3 mm (Figure 1A-D).
FINAL DIAGNOSIS
Then they came to a stream of rushing water; but the little man drew out a wand and touched the waves, whereupon the waters parted and stood still, and the two crossed the river with dry feet
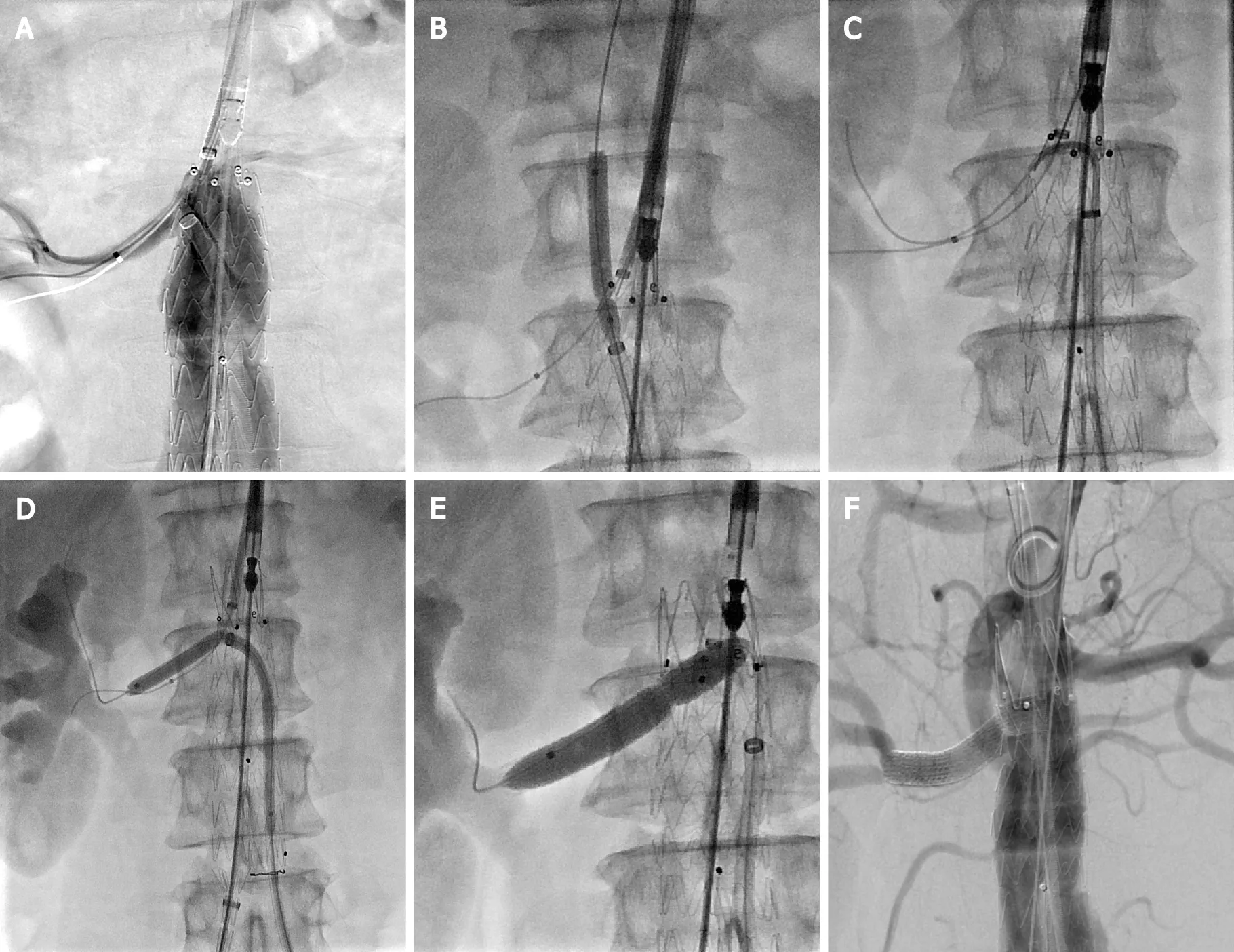
Emergency surgery was performed 24 h after admission.The surgical procedure was as follows.A sizing catheter was advancedleft femoral access,allowing for angiography and pertinent measurements to be achieved (Figure 1E).A long sheath (Flexor,Cook Medical) was used to deploy a guidewire and a balloon catheter into the RRAbrachial access to allow RRA salvage in case of fenestration failure.First,the right internal iliac artery was embolized.An Endurant II stent graft (25 mm × 13 mm × 166 mm,Medtronic Vascular,Inc.) was advanced through the right femoral sheath and deployed just below the left renal artery.The short leg of the stent graft was released while leaving the bare stent in place.Thereafter,a 10-F steerable sheath (FuStar,Lifetech Scientific Corp.) was inserted into the stent graft from the left groin through the short leg.The ostium of the RRA was displayed in real time by contrast injection from the brachial access point.Meanwhile,the tip of the steerable sheath was adjusted to align with the ostium of the RRA (Figure 2A),and the site of perforation was determined2 different fluoroscopic projections.A 4-mm balloon catheter (Bard Rival,Bard Peripheral Vascular) was passedthe sheath followed by a laser fiber (GIGAA Laser,Wuhan,China),which was calibrated to deliver energy pulses of 18 W in 3 s,to fenestrate the membrane of the thoracic aortic stent graft[2].After fenestration,the laser was removed and replaced with a 0.035-inch guide wire that was advanced into the proximal abdominal aorta.A 4-mm balloon was passed along the wire across the opening,and balloon dilation was achieved (Figure 2B).Due to the straight angle,after trying a variety of catheters,we finally used a trimmed pigtail catheter (Merit Medical Systems,Inc.) to reach the RRA (Figure 2C).An angioplasty balloon (5 mm × 10 mm,Mustang,Boston Scientific Corp.) was passed from the opening into the renal artery,followed by balloon dilation.Then,the balloon was deflated to 2 atmospheres,with no residual waist,while the bare stent was fully released.The stent was opened smoothly,without any balloon kinking (Figure 2D).Thereafter,a covered stent (8 mm × 50 mm,GORE VIABAHN) was deployed.Then,a 7-mm angioplasty balloon was used to “flare” the RRA stent (Figure 2E).Angiography demonstrated that the RRA was patent,with no endoleakage (Figure 2F).Then,the contralateral iliac limb was placed,with no issues.Repeat ballooning of the regions of stent overlap was performed with a Codaballoon (Cook Medical).Imaging on completion demonstrated good renal perfusion,with no evidence of endoleakage or stenosis (Figure 3A).
TREATMENT
Quietly the husband stated, I don t have anything on my list. I think that you are perfect the way that you are. I don t want you to change anything for me. You are lovely and wonderful and I wouldn t want to try and change anything about you.
OUTCOME AND FOLLOW-UP
Then said he, I am thy betrothed bridegroom, whom thou sawest as Bearskin, but through God s grace31 I have again received my human form, and have once more become clean
She caught sight of Kay; she recognised him, and ran and put her arms round his neck, crying, Kay! dear little Kay! I have found you at last! But he sat quite still and cold
DISCUSSION
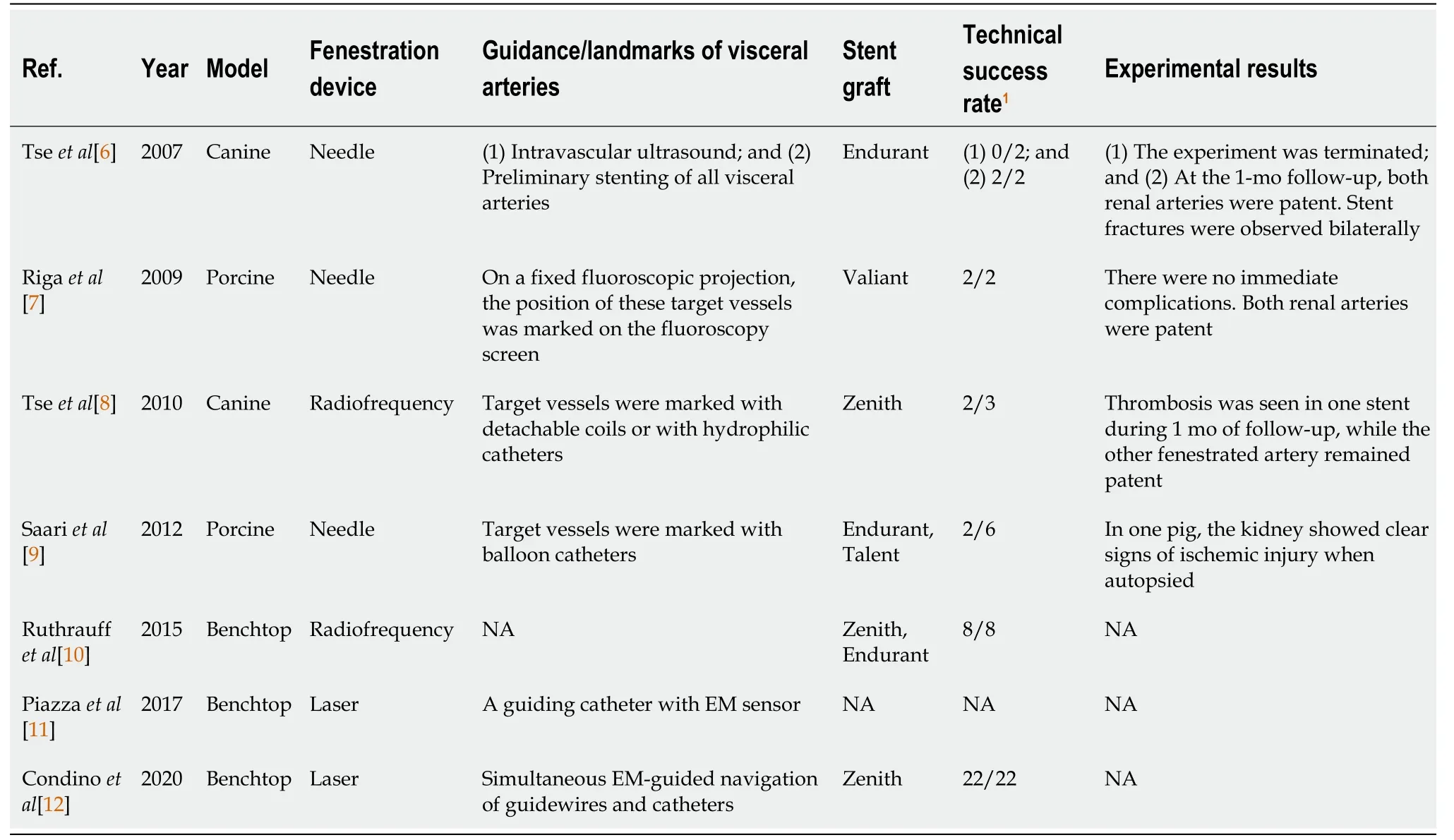
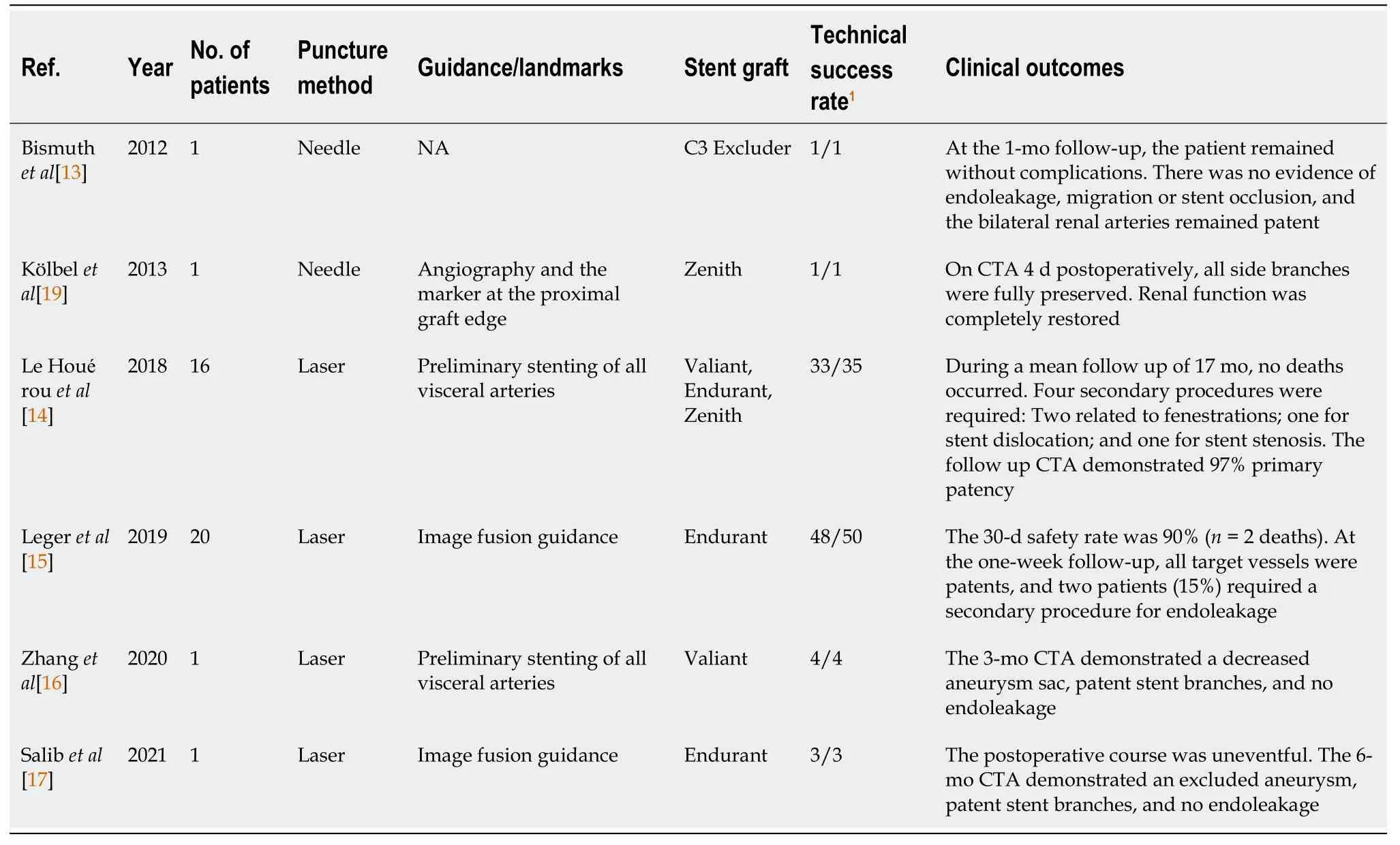
The endovascular repair of complex aortic aneurysms involving renal and/or visceral branches usually requires combination treatment with various types of stent graft modifications to preserve side branch patency.These techniques feature devices with parallel grafts,fenestrations,or branches.The parallel graft technique has a high risk of type 1A endoleakage,especially when multiple arteries require reconstruction[17].The use of such customized systems,including those involving fenestrated grafts and branched endografts,requires accurate preoperative imaging and planning.During the procedure,alignment of the vessel ostia with the fenestrations or branches can be difficult[3-5,19].In addition,the high cost and long waiting time reduce the accessibility of these technologies to patients,particularly in emergent cases.In retrograde ISF,as the site is approached from within the target vessel,it is easy to place the stent graft at the correct site,and this method has been confirmed to be effective and safe for use in major aortic branches[2].Unfortunately,retrograde endovascular revascularization cannot be easily achieved in visceral arteries[3,4,20].Since Tse[6] first reported the feasibility of antegrade ISF in the placement of abdominal aortic stent grafts to preserve the patency of the renal arteries in a canine model,many studies have explored this technique (Tables 1 and 2).
Fenestration devices are important components of antegrade ISF.Graft perforation is achieved easily with most devices,including mechanical and energetic fenestration devices.Mechanical fenestration requires rigidity to transfer force from the operator’s hands to the graft.If the angulation of the needle is not sufficiently acute,target vessel cannulation becomes difficult[6,9].Additionally,the rigidity of the needle may make it difficult to cross the typically tortuous and diseased iliac vessels.However,the occurrence of complications,such as retroperitoneal hematoma,has been rarely reported in previous studies[6,7,9].Compared with needles,radiofrequency probes and laser fibers have been found to be sufficiently compliant for perforation[8].Therefore,we decided to perform ISLF in this case.
22 It was a pity that Bearskin s face was covered with dirt and with hair, for if not they might have seen how delighted he was when he heard these words
When using an antegrade approach in visceral arteries,finding the right puncture site can be challenging.To allow for fluoroscopic visualization,various landmarks can be deployed in target arteries prior to endograft deployment.In Tse[6]’s first report,bare stents were deployed in both renal arteries;however,stent fractures were observed bilaterally.No renal stent fractures were observed in a second study by the same team[8],in which the modified stent grafts had an unsupported portion in the fenestration area.In this study,they marked target vessels with detachable coils or hydrophilic catheters.However,thrombosis of the renal artery was observed after the procedure,which was likely related to partial coil deployment.Le Houérou[14] confirmed the feasibility of preliminarily stenting each target artery in a large clinical study[14].Hsiao[21] found that overlapping stents exhibited lower fatigue resistance during respiration than a single stent.In Saari[9]’s study,deflation of the balloon in the renal artery indicated successful puncture,but a long warm ischemia time for the left kidney caused infarction.Furthermore,stents,balloons,and coils result in additional costs.
To avoid using invasive landmarks,Riga[7] marked target vessels on a fluoroscopy screen on a fixed projection with robot-assisted antegrade ISF.Leger[15] and Salib[17] succeeded under fused CT guidance.However,the configuration of the aorta may change after stent graft insertion[5].To accurately position stent grafts in real time,various navigation devices have been tested for guidance during antegrade ISF.Intravascular ultrasound probes were not able to visualize the renal orifices for fenestration both within the stent graft and within the inferior vena cava[6].However,electromagnetically guided endovascular instrumentation was successful intrials[11,12].Therefore,in our case,fenestration was performed while the stent graft was positioned well with the bare stent region unreleased,allowing real-time positioning by angiography.
Blocking a visceral artery may cause visceral ischemia[9].Le Houérou[14] implanted an undersized stent graft at the level of the visceral aorta to avoid temporary visceral ischemia.Tse[8] thought that,in theory,the marking catheter could serve to cold-perfuse renal arteries during the fenestration procedure.Bismuth[13] performed antegrade ISF with a constrained stent graft.In our case,fenestration was performed while the bare stent region was unreleased,and RRA perfusion was maintained during the procedure.
The stability of supporting devices is also important for correct positioning of the perforation site.Tse[6] described that support for the needle was provided by inflating a balloon catheter against the contralateral aortic wall.However,this catheter does not provide sufficient needle angulation.In most studies,a steerable catheter or sheath has been used to support fenestration devices.Riga[7] used a remotely controlled robotic steerable catheter system to improve accuracy and stability.Piazza[11] also proposed some design solutions for catheter stabilization.In this study,a FuStar steerable sheath was used.In addition,the main body of the stent graft was fixed,and the space in the proximal part was limited,which improved the stability of the fenestration system.
Other aspects,such as fatigue resistance[21],are also important issues in antegrade ISF.Our technique may be suitable for use in select JAAA patients with the involvement of only one renal artery.Due to the length limitation of the bare area,whether other visceral arteries can be cannulated in the same fashion needs further study.
CONCLUSION
This study suggests the feasibility and short-term safety of this novel antegrade ISF technique as an off-label technique for use in select JAAA patients.Renal artery perfusion was maintained during the procedure,and accurate positioning was achieved using angiography.This technique could serve as an alternative approach for the management of hostile proximal aortic necks during EVAR.However,the longterm effects of this method require further study in a larger cohort with long-term follow-up.
 World Journal of Clinical Cases2022年4期
World Journal of Clinical Cases2022年4期
- World Journal of Clinical Cases的其它文章
- Surgical treatment of acute cholecystitis in patients with confirmed COVID-19:Ten case reports and review of literature
- Rituximab as a treatment for human immunodeficiency virusassociated nemaline myopathy:What does the literature have to tell us?
- Eustachian tube involvement in a patient with relapsing polychondritis detected by magnetic resonance imaging:A case report
- Endoscopic clipping for the secondary prophylaxis of bleeding gastric varices in a patient with cirrhosis:A case report
- Inflammatory myofibroblastic tumor after breast prosthesis:A case report and literature review
- Langerhans cell histiocytosis presenting as an isolated brain tumour:A case report