Inflammatory myofibroblastic tumor after breast prosthesis:A case report and literature review
2022-03-15 07:12:32PengZhouYiHaoChenJiangHaoLuChunChunJinXiaoHongXuXueHaoGong
World Journal of Clinical Cases 2022年4期
INTRODUCTION
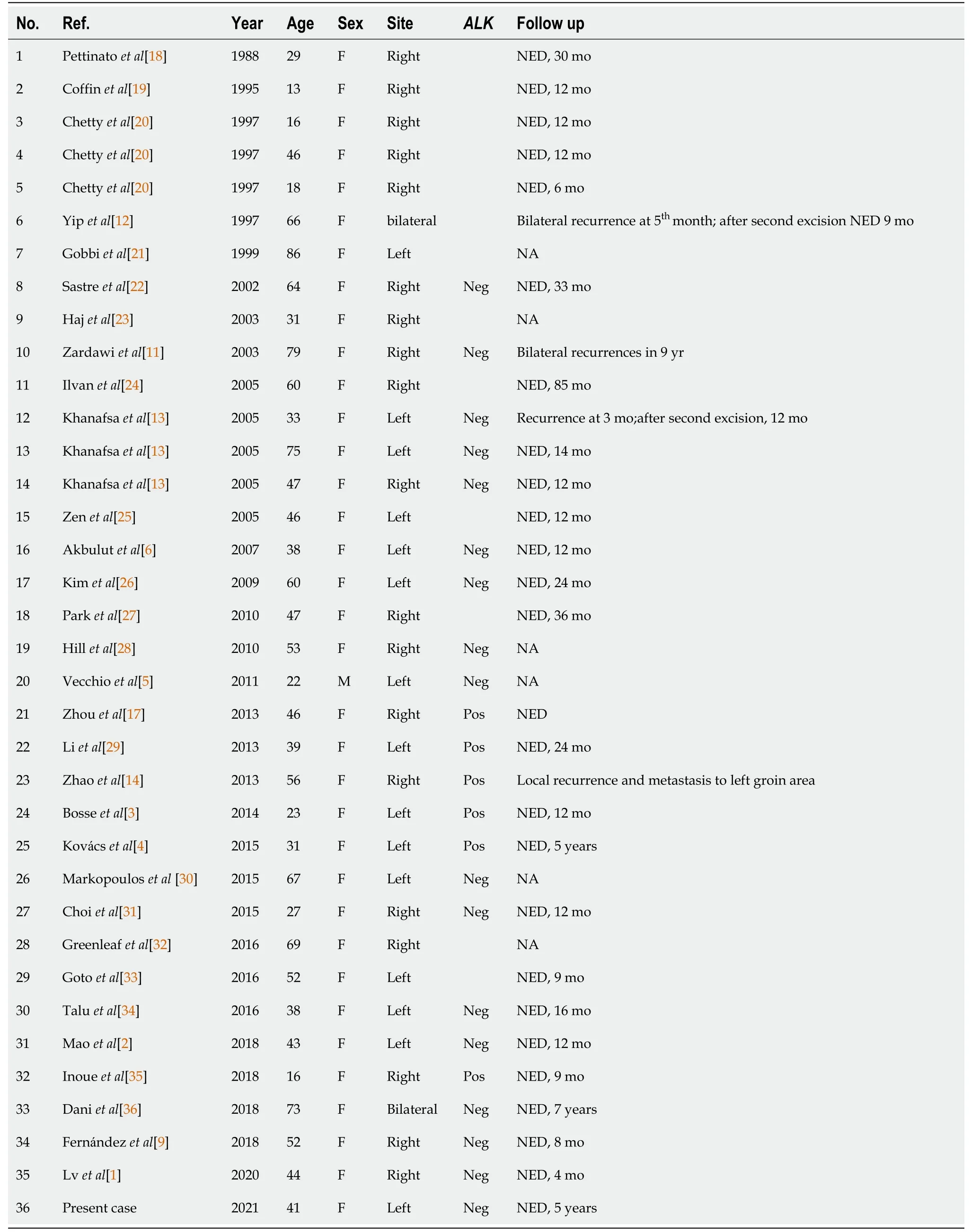
Inflammatory myofibroblastic tumors (IMTs) are rare lesions of mesenchymal origin,with a global incidence of approximately 0.04%–0.7%[1].They primarily occur in the lungs,abdomen,pelvis,and retroperitoneum of adolescents.Unlike IMTs in other organs,most breast IMTs occur in middle-aged women>40 years old[2].Although reported in various organs,the occurrence of IMT in the breast is rare,and to the best of our knowledge,only 35 cases have been reported.Herein,we report a case of IMT following resection of a malignant phyllodes tumor of the left breast and implantation of a prosthesis.In addition,we review current studies on breast IMT.
CASE PRESENTATION
Chief complaints
A 41-year-old female had a mass in the left breast for 3 mo.
He rested on the waves, he trod the water- infact, did everything he could think of, in order not to fatiguehimself, and to reserve strength enough to reach land
History of present illness
During the 3 mo,the breast mass had slowly enlarged,but the patient did not have clinical symptoms,such as fever and pain.
History of past illness
The patient had undergone implantation of a prosthesis five years prior and resection of a large mass in her left breast,pathologically diagnosed as a malignant phyllodes tumor.
Personal and family history
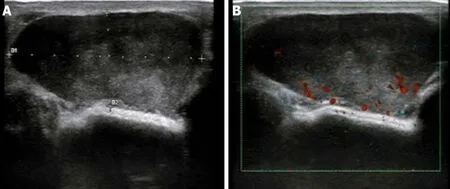
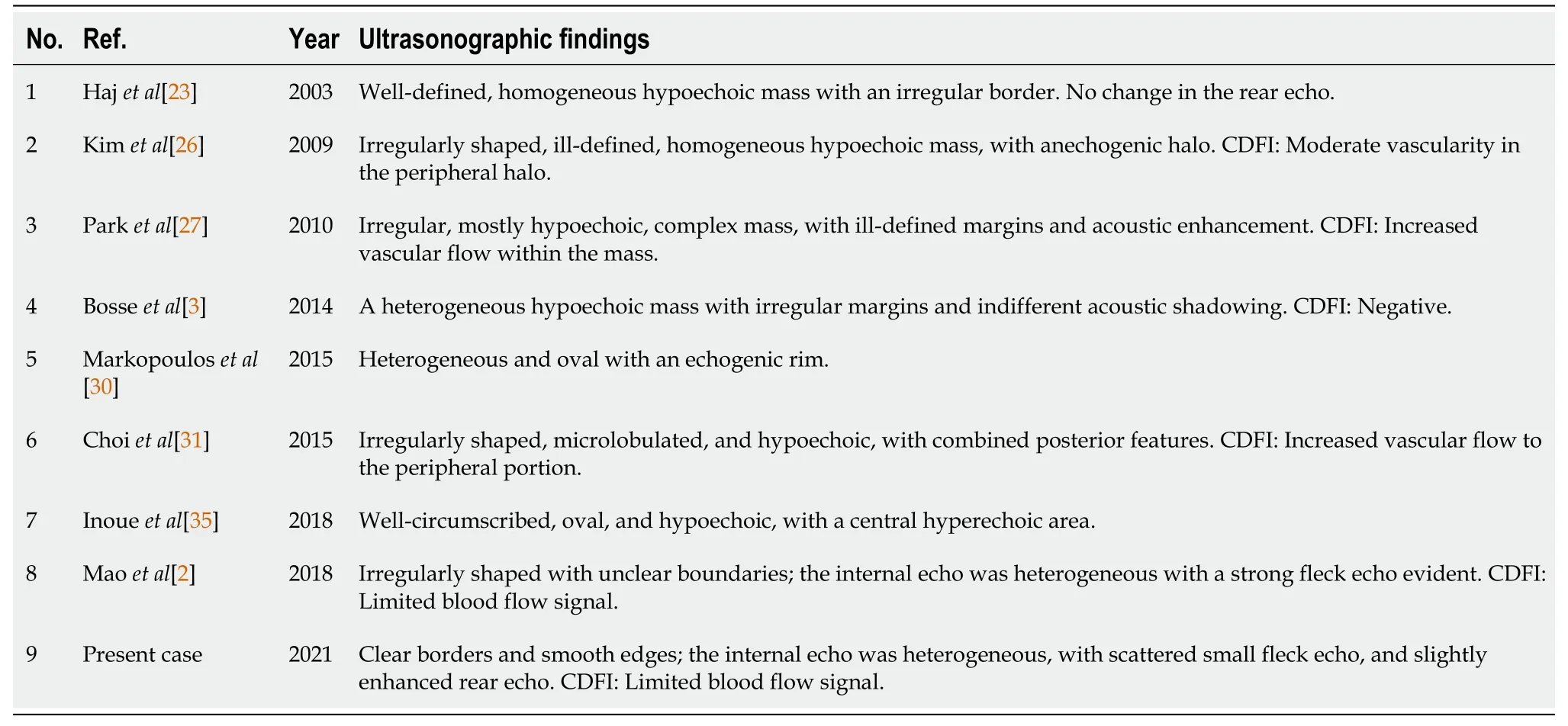
Ultrasonic examination (Esaote M7,Genova,Italy) revealed an oval,hypoechoic mass (approximately 4.2 cm × 1.8 cm in size) with clear borders and smooth edges at the 9 o'clock position in the left breast that is 3.5 cm from the nipple.Internal echo was heterogeneous,with scattered small fleck echo and slightly enhanced rear echo.A disc-shaped anechoic area was observed behind the left breast,with good internal sound transmission.Color Doppler flow imaging (CDFI) indicated a limited blood flow signal within the hypoechoic mass (Figure 1).
Physical examination
Physical examination revealed an abnormal shape of the left breast and prosthesis,which was palpable.Additionally,an approximately 4 cm × 3 cm non-tender mass,with a clear boundary and poor activity,was identified at the 9 o’clock position.
This case is a patient we diagnosed and treated five years ago.Due to insufficient experience and inefficient equipment at the time,we only performed gray-scale ultrasound and CDFI on the patient,which was insufficient.In current practice,we will recommend contrast-enhanced ultrasound (CEUS) to patients with similar cases before surgery.CEUS as a pure blood pool phenomenon technology,especially the rapid development of high-frame-rate CEUS in recent years,can show the richness of the blood supply and the blood supply pattern of the tumor,which help differentiate benign and malignant tumors.In addition,CEUS can further clarify the boundary of the tumor and show whether the surrounding normal tissues have been invaded.If there is an invasion,it can show the range of invasion,which helps determine the scope of surgical resection and ensure that the resection margin is negative.
Laboratory examinations
No abnormalities were found in the patient’s laboratory examinations.
Imaging examinations
The patient had no relevant family history.
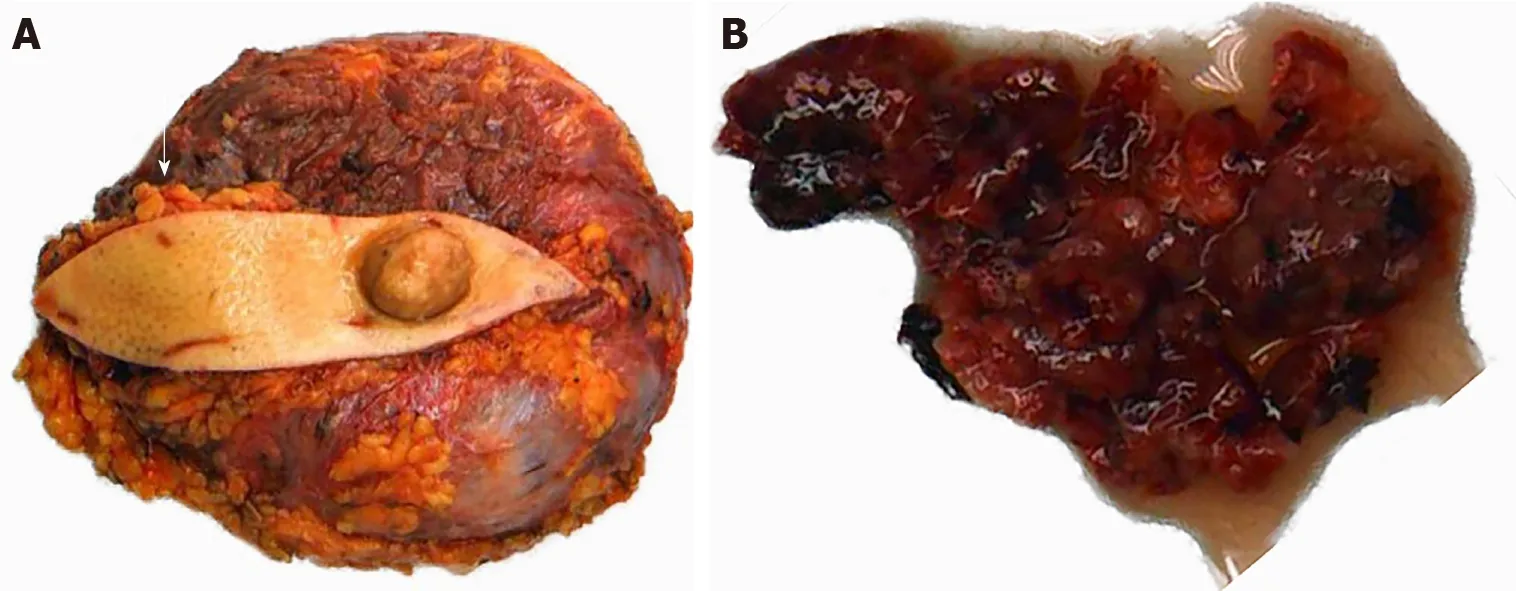
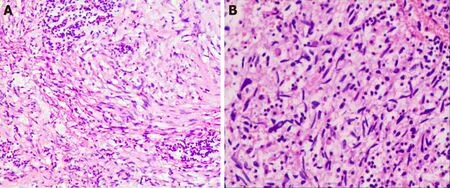
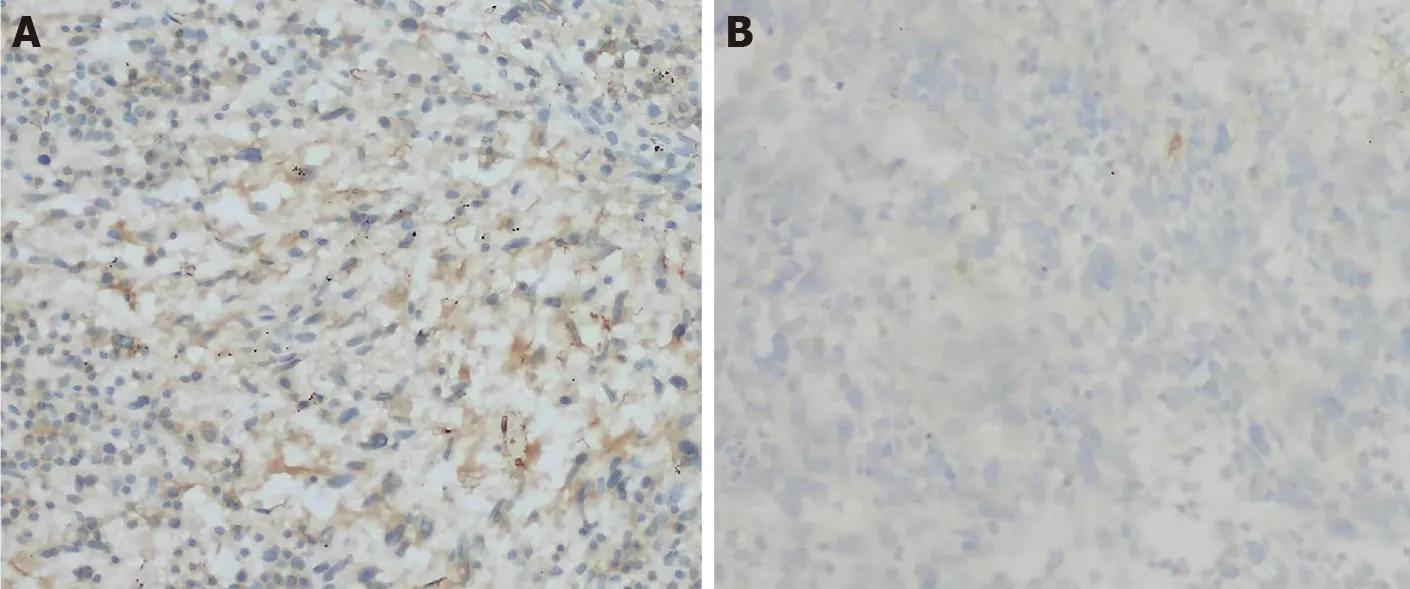
The patient underwent left breast mass resection and prosthesis removal in our hospital due to the abnormal shape of the left breast and the large mass.Specimens mainly included the breast glandular tissue,tumor tissue,prosthesis,spindle-shaped flap,and nipple (Figure 2).A complete prosthesis was identified behind the breast tissue,with a knot observed under the skin 3.5 cm from the nipple section (2.5 cm × 2.5 cm × 1.5 cm),which was gray-red and soft,with missing central tissue.Light microscopy revealed that the spindle cells to be diffusely proliferated,irregularly arranged,and scattered in the nucleus.Additionally,mildly atypical cells,mitosis,interstitial vascular proliferation,and dilation and congestion with hemorrhage were evident,as well as a large number of neutrophils and lymphocytes and plasma cell infiltration (Figure 3).Immunohistochemical staining revealed that the spindle cells were partially positive for smooth muscle actin (SMA),positive for BCL-2 and cluster of differentiation (CD) 99 but were negative for anaplastic lymphoma kinase (),cytokeratin (CK),S-100 protein,desmin,and CD34.The Ki-67 score was approximately 5%,which is atypical for an IMT (Figure 4).
FINAL DIAGNOSIS
IMTs of the breast are rare and unique;however,whether they are reactive or neoplastic in nature remains unelucidated.IMTs were widely considered inflammatory lesions and have been referred to as inflammatory pseudotumors,plasma cell granulomas,fibrous xanthomas,and inflammatory myofibrohistiocytic proliferation.Conversely,cases of local recurrence and metastasis have challenged the theory of reactive post-inflammatory lesions.As proven through cytogenetic analysis,approximately 50% of IMTs are positive for rearrangements involving thegene,while cytogenetic abnormalities support the neoplastic nature of IMTs[3].Nevertheless,the pathogenesis of-negative IMT remains controversial.These lesions might not undergo gene rearrangements and might be caused by trauma,surgery,infection,or other factors that cause excessive inflammation in human tissues,which activate the abnormal proliferation of myofibroblasts[4].
TREATMENT
The king was frightened indeed, and thought she was raving13, but in order to please her, he said, Well, of these three things I shall choose the last; if you die, I shall lay you at once in a plain wooden chest, and have it set in the church, and every night I shall place a sentinel beside it
OUTCOME AND FOLLOW-UP
The patient was followed up every year.Each follow-up examination included a physical examination,a chest X-ray,a breast ultrasound (US),an abdominal US,and a routine blood examination.During the 5-year postoperative follow-up,the patient had no symptoms or imaging evidence of recurrence or metastasis.
DISCUSSION
The diagnosis was IMT.
Gretel is not the only fairy tale sister to rescue her brother. Also read Brother and Sister and The Six Swans on SurLaLune to read tales in which sisters rescue their brothers from spells or death.
She had not a button- that she knew right well, and therefore she remained standing9 sorrowfully outside, till all the others had seen the grave and had gone away; then she sat down, held her little brown hands before her eyes, and burst into tears; this girl alone had not seen Puggie s grave
Among the 35 cases of breast IMT reported in the literature,all but one occurred in females[5].The patients’ ages ranged from 13 to 86 years,with a mean age of 47.1 years (Table 1).In our case,the patient was a 41-year-old middle-aged woman who sought medical attention due to a palpable mass.Retrospective analysis of the ultrasonograms revealed that the uneven,low echo in the mass was primarily related to the diffuse proliferation and irregular array of spindle cells in the tumor.Conversely,the scattered and small high echo could have been caused by considerable mixed acute and chronic inflammatory cell infiltration,while the spotty blood flow signal detected in the mass may be related to interstitial vascular hyperplasia with hemorrhage determined via light microscopy.The above-mentioned ultrasound manifestations lacked specificity;thus,it was difficult to distinguish them from those of phyllodes tumors or giant fibroadenomas.IMTs may also manifest with the imaging features of malignant tumors and show the diversity and lack of specificity in ultrasound imaging (Table 2).Furthermore,some scholars believe that the definitive diagnosis of IMT is difficult based on cytology alone.A reliable diagnosis may require histological samples because IMT cytology may mimic other benign or malignant breast lesions without specific features[6].Therefore,the final diagnosis still requires postoperative histopathological examination.
Before we were married, Patricia and I could not see each other as much as we would have like during the week. The weekends always went too fast, and the days in between dragged on forever. I decided5 that I needed to do something to make the weekdays go faster, or at least to give us something to look forward to during the week.
The patient had undergone prosthesis implantation in our hospital 5 years prior and resection of a large mass (approximately 10 cm × 10 cm × 5 cm in size) pathologically diagnosed as a malignant phyllodes tumor following a surgery in the left breast.Due to this history of phyllodes tumor,we first considered the possibility of lobular tumor recurrence.Histological analysis of phyllodes tumors indicates that they are typically arranged in a slit-like epithelial bilayer component rich in cells surrounding the mesenchymal overgrowth and interstitial inflammatory cell-free components.In the present embodiment,the optical microscope did not meet the performance;thus,phyllodes tumor recurrence may be excluded.Since metaplastic breast carcinoma appears similar to IMT under the light microscope,there is a marked difference in management and prognosis.Therefore,immunohistochemistry should be performed to rule out this possibility.Following an immunohistochemical assay,we found that the spindle cells were reactive for SMA,while the tumor cells were negative for CK,which ruled out the possibility of metaplastic carcinoma.Based on a comprehensive assessment of the patient history and histopathological and immunohistochemical results,IMT was considered the final diagnosis.
This case presented the opportunity to critically review the literature regarding the cases of breast IMTs (Table 1) to determine whether they are reactive lesions due to an exaggerated response to tissue injury or indicate a true neoplastic process.Although approximately half of all IMTs across anatomical sites undergo clonal rearrangements of thegene on chromosome 2p23 activating ALK protein expression (Table 1),overexpression in breast IMTs is rare.In this article,we discuss-negative breast IMT especially its possible etiology of trauma and surgery,which could challenge the theory that the tumorigenic nature of chromosomal abnormalities supports IMTs.The patient had undergone left breast mass resection and prosthesis implantation due to a large malignant lobular tumor of the left breast.Moreover,newly developed IMT presented 5 years following surgery.Notably,most cases of breast IMT are spontaneous,and only a few cases that had a history of trauma and tumor resection before IMTs have been reported[5].Vecchio[5] reported a male patient with breast IMT that had developed 4 mo following mechanical trauma;its location was consistent with the site of the trauma.Mao[2] reported a 43-year-old female who developed IMT 18 mo following resection of a left breast fibroadenoma.Both studies of Vecchio[5] and Mao[2] speculated that trauma and surgery could be important factors that promote the development of IMT.Moreover,Vecchio[5] reported that IMT was essentially reactive due to an absence ofexpression and benign clinical behavior without any evidence of metastasis.IMT and inflammatory pseudotumors are thus different variants of the same disease[5].Based on the view that chronic inflammation is considered the cause,we humbly propose a new viewpoint that prosthesis implantation also causes IMT.
Considering the origin cells of IMTs,myofibroblasts are mainly involved in the growth,repair,and scarring of normal tissue.An abnormal inflammatory response induces the over proliferation of myofibroblasts,thereby forming IMTs.In this case,a large number of acute and chronic inflammatory cells,such as neutrophils,lymphocytes,and plasma cells,were observed under the light microscope.We hypothesized that this abnormal inflammatory response could have been attributed to the surgical trauma caused by the resection of the large malignant tumor and the prolonged stimulation of the prosthesis as a foreign body.Previous studies reported that prosthesis implantation was closely related to the incidence of breast fibromatosis[7].Notably,breast fibromatosis and IMT originate from myofibroblasts.In addition,this case and those reported by Vecchio[5] and Mao[2] were negative for,indirectly indicating thatgene fusion may not have occurred.This supports the speculation that these mammary lesions are reactive in nature;however,through genetic testing,some studies have observed thatgene fusion can occur in very few-negative IMTs from the lung[8].Whether a similar phenomenon can occur in-negative breast IMT has not been reported.Unfortunately,genetic testing was not performed in this case aswas not expressed,with no evidence to prove thatgene changes had occurred.While it can be inferred from Table 1 that-negative IMT has almost no recurrence,whether-negative expression is a good prognostic factor for IMT remains unelucidated[9].
The malignant potential of IMT is incompletely characterized.Radical resection is the preferred method of treatment for breast IMTs.Kovach[10] confirmed that the recurrence rate of the primary surgical approach was 8%.Moreover,if there are no contraindications related to patient anatomy or morbidity,surgical resection of all lesions is recommended.In our review of 35 cases of breast IMTs,all tumors were initially treated with surgery,and the outcome of most breast IMTs is favorable.Recurrences occurred in four cases[11-14],including two cases of bilateral metastasis[11,12].In one case,local recurrence occurred,and metastasis to the groin area was confirmed[14].In addition to surgery,some scholars believe that ALK-targeted inhibitors,such as,are used to treat patients with metastatic or unresectable ALK-positive IMT and provide surgical opportunities[15].Sporadic cases show that treatment with corticosteroids improves the outcome[16];however,these results are still under discussion,whereas adjunctive therapy after surgery needs further clinical investigation.Although most patients achieved satisfactory results,follow-up remains essential.Notably,no clear molecular cytogenetics or clinical characteristics following resection could predict the risk of recurrence or metastasis[17].Therefore,ultrasonography has great value in the timely detection of breast IMTs,preoperative lesion range determination,postoperative monitoring,and follow-up due to its convenience and radiation-free nature.
CONCLUSION
Breast IMT is extremely rare;prosthesis implantation may cause IMT,although further investigation is necessary to prove it.Its clinical manifestations lack specificity,and imaging manifestations are diverse.Therefore,Sonographers should perform a comprehensive analysis of the medical history for the diagnosis,especially in patients with pathogenic factors,such as trauma or prosthesis implantation surgery,the possibility of IMT should be considered.Radical resection and postoperative close follow-up are recommended,although the pathogenesis and biological behavior of IMT remain unelucidated.
 World Journal of Clinical Cases2022年4期
World Journal of Clinical Cases2022年4期
- World Journal of Clinical Cases的其它文章
- Surgical treatment of acute cholecystitis in patients with confirmed COVID-19:Ten case reports and review of literature
- Rituximab as a treatment for human immunodeficiency virusassociated nemaline myopathy:What does the literature have to tell us?
- Eustachian tube involvement in a patient with relapsing polychondritis detected by magnetic resonance imaging:A case report
- Endoscopic clipping for the secondary prophylaxis of bleeding gastric varices in a patient with cirrhosis:A case report
- Langerhans cell histiocytosis presenting as an isolated brain tumour:A case report
- Hoffa’s fracture in an adolescent treated with an innovative surgical procedure:A case report