Gastrointestinal amyloidosis in a patient with smoldering multiple myeloma:A case report
2022-03-15 06:05:00AiLingLiuXueLiDingHuaLiuWenJunZhaoXueJingXuanZhouTaoMaoZiBinTianJunWu
World Journal of Clinical Cases 2022年7期
lNTRODUCTlON
Amyloidosis is a clinical disorder of extracellular deposition of fibrillar proteins in one or more organs.More than 40 different types of proteins have been identified to form amyloid in humans.The most common protein found in amyloidosis is the light chain immunoglobulin.Amyloidosis(light chain)(AL)is the most common form of systemic amyloidosis,accounting for approximately 70% of all cases[1].The monoclonal light chain(κ or λ)originates from the abnormal proliferation of bone marrow plasma cells[2].Multiple myeloma(MM)is a hematologic malignancy characterized by uncontrolled proliferation of monoclonal plasma cells in the bone marrow.The common clinical manifestations of MM are bone pain,anemia,kidney injury,repeated infections,and extramedullary plasmacytoma[3].When the patient is asymptomatic,it is called smoldering MM(SMM).Approximately 10%-15% of MM patients develop overt AL[4].However,there are few reports of MM coexisting with gastrointestinal AL[4].Moreover,there are only two reported cases of SMM combined with gastrointestinal AL to date[5,6].Here,we report a case of an elderly woman with SMM and gastrointestinal AL who was successfully treated with chemotherapy.
CASE PRESENTATlON
Chief complaints
A 63-year-old woman was admitted to our hospital in November 2016 due to pedal edema lasting four months,abdominal distension and abdominal pain for one month,and hematochezia for one week.She had no nausea,vomiting,fever or weight loss.
History of past illness
The patient had no history of malignancy.
Personal and family history
This patient had no history of smoking or drinking,and no familial history of genetic diseases.
The beggar there, said her husband, has joys of his own whichseem to him great, and cause him as much pleasure as a king would find in the magnificence of his palace. And then do you not think thatthe beast of burden, which suffers blows and hunger, and worksitself to death, suffers just as much from its miserable fate? Thedumb creature might demand a future life also, and declare the lawunjust that excludes it from the advantages of the higher creation. Christ said: In my father s house are many mansions, sheanswered. Heaven is as boundless as the love of our Creator; the dumb animal is also His creature, and I firmly believe that no life will be lost, but each will receive as much happiness as he can enjoy, which will be sufficient for him.
Physical examination
With what a look she gazed up into his face, as with a prayer to Godfor help he breasted the waves, which rushed over the sinking ship!She uttered a cry, but she felt safe and certain that he would notleave her to sink

Laboratory examinations
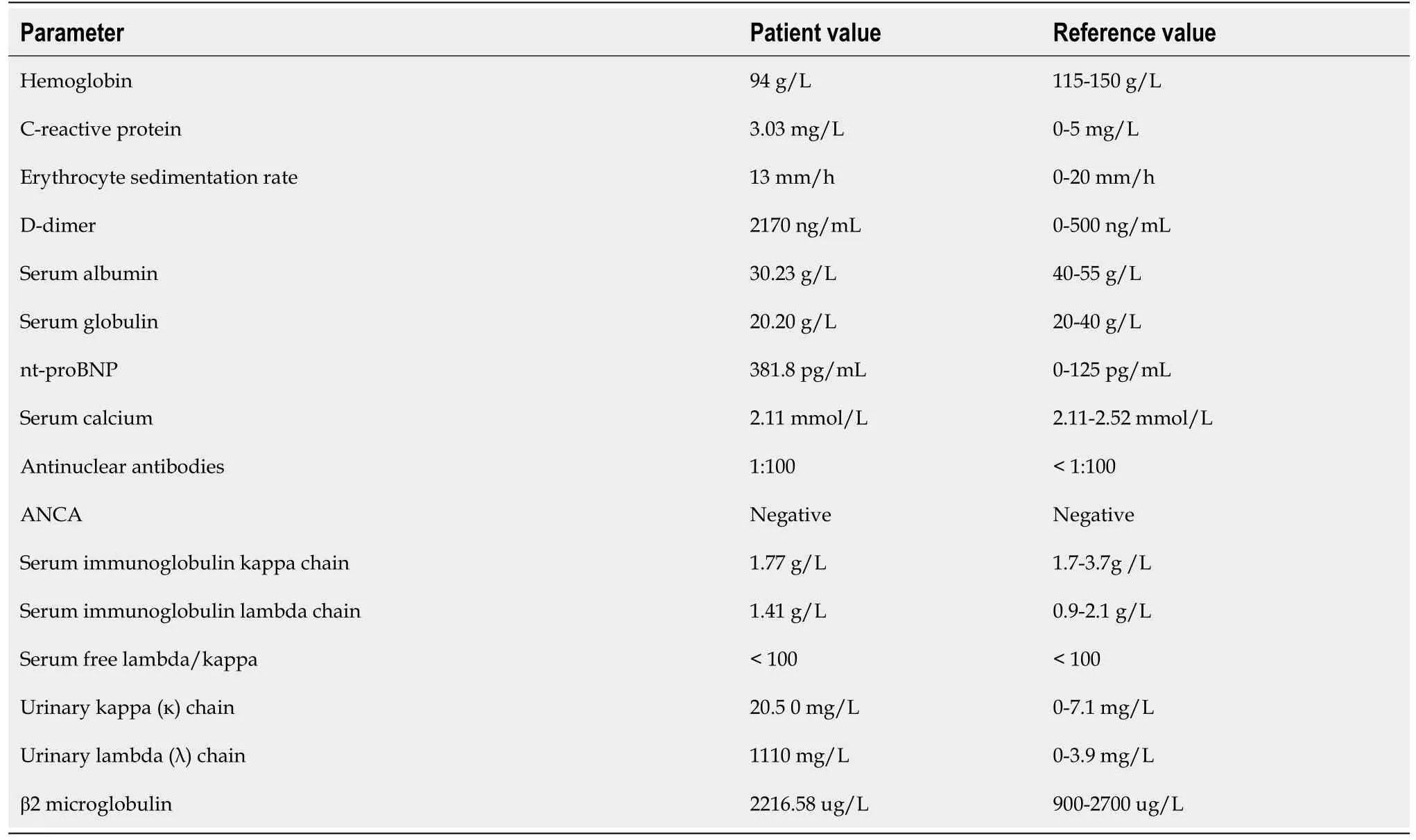
Laboratory investigations revealed normocytic anemia,hypoalbuminemia,and increased D-dimer.Stool occult blood was positive.Urinary kappa chain and lambda chain were elevated(Table 1).Serum protein electrophoresis and immunofixation were negative.
In summary,we report a rare case of SMM with gastrointestinal AL achieving long-term survival of about 5 years with medical therapy.Gastrointestinal amyloidosis should be considered in elderly patients with endoscopic findings of granular-appearing mucosa,ecchymosis,and submucosal hematoma.Once amyloidosis is diagnosed,further evaluation should be carried out to distinguish between primary and secondary amyloidosis,identify the subtype of amyloidosis,and determine the organ involvement.Timely diagnosis and treatment can help to improve the prognosis.
Imaging examinations
The electrocardiogram was normal.Echocardiography revealed normal left ventricular ejection fraction(61%)and slightly decreased left ventricular diastolic function.Computed tomography(CT)found marked thickening of the stomach and whole colon mild ascites,and pleural effusion.Doppler ultrasound revealed left lower limb venous thrombosis.Gastroscopy showed gastric retention,mucosal coarseness,hyperemia,and mild oozing of blood from the incisura angularis(Figure 2).Colonoscopy showed mucosal hyperemia,edema with multiple round and irregular ulcers,ecchymosis and hematoma in the distal descending and sigmoid colon(Figure 3).Histologic staining with Congo red stain(Figure 4)revealed positively staining deposits in the lamina propria of the gastric and colonic mucosa without plasmacytic infiltration.A bone marrow aspiration smear was hypocellular with reduced numbers of granulocytic and erythroid precursors in each stage.No gene mutation was tested.Bone marrow biopsy showed the presence of neoplastic plasma cells in small clusters accounting for 15%-20% of the marrow elements.Immunohistochemistry revealed lambda light chains in the neoplastic cells establishing the diagnosis of MM.X-rays of the head,lumbar spine,pelvis,and chest did not reveal any lytic lesions.



FlNAL DlAGNOSlS
The patient was regularly followed for roughly five years.During this period,the patient had occasional episodes of mild abdominal distension.The latest bone marrow biopsy in April 2021 showed that neoplastic plasma cells accounted for 20.5% of the marrow elements.Echocardiography revealed myocardial amyloidosis,suggesting progression of the disease.However,she is currently continuing chemotherapy and is doing well as of the last follow up in August 2021.
TREATMENT
The patient was started on proton pump inhibitors and somatostatin which significantly reduced her gastrointestinal symptoms.Subsequently,she received one session of inpatient chemotherapy with vindesine,epirubicin and dexamethasone.Thalidomide was added to prevent angiogenesis.Low molecular heparin and warfarin were given for lower extremity venous thrombosis.Bacterial pneumonia developed during the treatment.However,the patient improved after anti-infective therapy.She was discharged after a hospital stay of one month when the symptoms of lower limb edema,abdominal distension and abdominal pain improved.Later,she received outpatient chemotherapy with hypodermic injection of bortezomib(2.2 mg)on days 1,4,8,and 11,and intravenous dexamethasone(40.5 mg)on days 1,4,8,and 11 every month for about 5 years.After 10 mo,the patient was improved.The hemoglobin level increased to 127 g/L,and β2 microglobulin,urinary kappa chain,and lambda chain returned to normal.Bone marrow biopsy revealed hyperplastic medullary images without neoplastic plasma cells.
OUTCOME AND FOLLOW-UP
The patient was finally diagnosed as SMM with AL(λ subtype),involving tongue,skin,stomach and colon.
DlSCUSSlON
AL can be primary amyloidosis or secondary to myeloma.The proportion of λ and κ light chain is about 3:1[7].The incidence of AL is estimated to be 3 to 5 per million per year.The mean age of onset is about 65 years.AL can affect multiple organs such as heart,kidney,liver,tongue,gastrointestinal tract,skin and nerves.The digestive system is affected in about 3.2% patients with amyloidosis of any type[8],and roughly 10% patients with AL[9].The parts of digestive system most commonly affected are tongue,esophagus,stomach,small intestine,large intestine,liver,and spleen.The corresponding clinical manifestations include enlarged tongue,nausea,vomiting,abdominal pain,diarrhea,hematochezia,abdominal distension,constipation,and hepatosplenomegaly.The complications include mesenteric infarction,intestinal obstruction,and intestinal perforation.In the index case,tongue(enlargement)and skin(purpura)were affected with AL.Abnormal gastric motility resulted in gastric retention.Colonic ulcers and hematoma led to hematochezia.She did not have myocardial amyloidosis until nearly 5 years later.
On endoscopy,gastrointestinal amyloidosis can mimic inflammatory bowel disease,ischemic colitis,and gastrointestinal tumors.Amyloidosis can appear as granular-appearing mucosa,polyps,erosions,ulcers,and submucosal hematomas[10].The endoscopic manifestation of amyloidosis depends on the location and the amount of amyloid deposition.When a small amount of amyloid is deposited in the submucosa,the mucosal layer remains intact.As the amyloid deposition gradually increases,the elasticity of tissue decreases,the mucosa becomes erythematous with the development of erosions and ecchymosis.When there is abundant amyloid deposition,submucosal hematomas develop.After the absorption of hematoma,shallow ulcers and hyperplastic polypoidal lesions can be seen.When all layers of the intestinal wall are affected,fibroblast hyperplasia occurs which can cause intestinal stenosis and obstruction.The gastrointestinal bleeding from amyloidosis occurs due to local ischemia,infarction,and mucosal injury causing erosions,hematomas,and ulcerations.Gastrointestinal bleeding caused by submucosal hematoma can be obscure or overt,or sometimes life-threatening[5].
The authors declare that they have no conflicts of interest
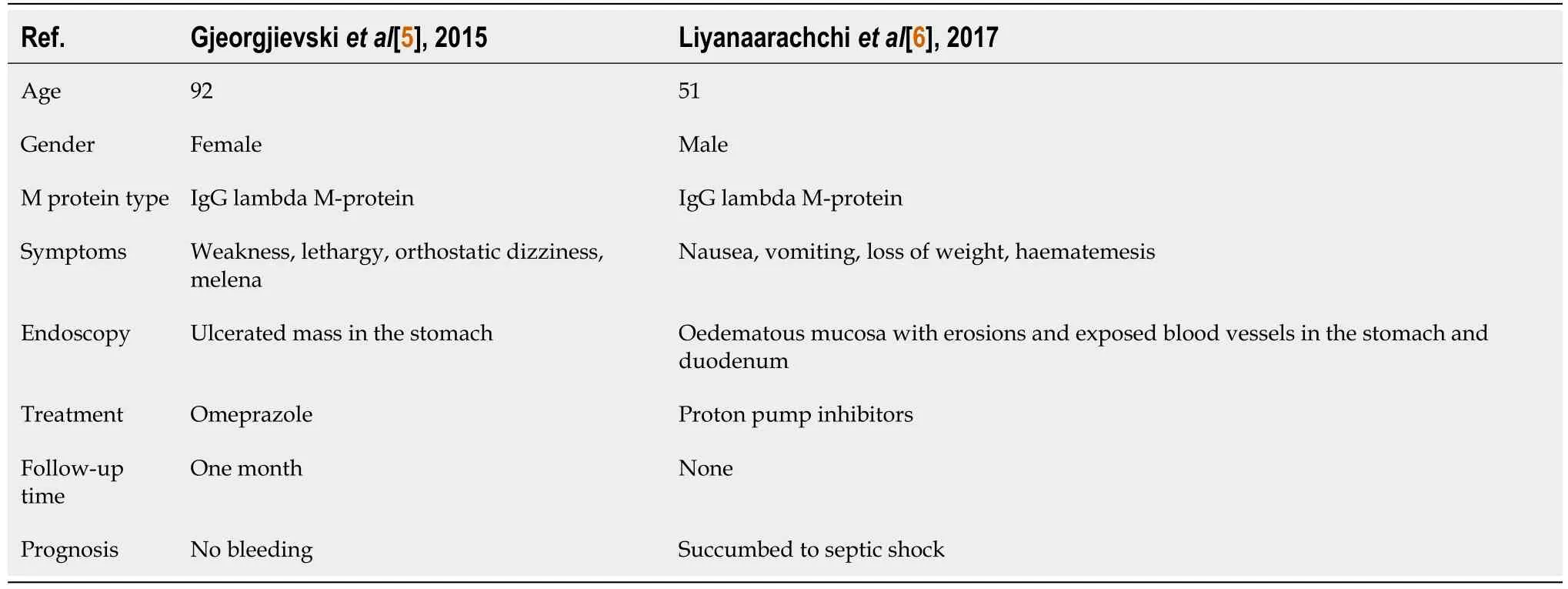
SMM is a transitional stage between monoclonal gammopathy of undetermined significance and MM.The diagnostic criteria of SMM are as follows[11]:monoclonal protein level ≥ 30 g/L ,or 24 hr urine immunoglobulin light chain ≥ 0.5 g(or both),or 10%-60% clonal marrow plasmacytosis with theabsence of end-organ damage and biomarkers of malignancy.The CRAB features of hypercalcemia,renal failure,anemia,and destructive bone lesions suggest end-organ failure.Biomarkers of malignancy(SLiM criteria)include plasma cells greater than 60% in the bone marrow,elevated serum free light chain ratio,and the presence of bone lesions on MRI[3].In our patient,the urinary lambda(λ)chain was 1110 mg/L and the bone marrow biopsy showed neoplastic plasma cells accounting for 15%-20% of the marrow elements.Though our patient had anemia and occult blood in stools,the anemia improved once the gastrointestinal bleeding ceased.Therefore,the cause of anemia in the present case was gastrointestinal bleeding rather than bone marrow failure due to MM.Although the patient did not undergo MRI,the X-ray revealed no lytic lesions.Hence,the patient had no CRAB or SLiM criteria.The patient was finally diagnosed as AL secondary to SMM.A comprehensive literature search was conducted with publication dates from January 1,1990,to August 31,2021.There are only two reported cases of SMM combined with gastrointestinal AL(Table 2).Gjeorgjievski[5]reported a 92-year-old female with a history of SMM who presented with progressive fatigue,dizziness,and melena.Bone marrow biopsy showed numerous plasma cells with λ light chain on immunohistochemical staining.Endoscopy revealed an ulcerated mass in the gastric body.Tissue biopsy with positive Congo red staining was consistent with gastric AL(λ)amyloidosis.Gastrointestinal bleeding stopped when she was given intravenous omeprazole.However,the patient’s reported follow-up time(one month)was very short.Liyanaarachchi[6]reported a 51-year-old male who was admitted with nausea,vomiting,loss of weight,and haematemesis for 2 mo.Bone marrow aspiration and biopsy revealed hypercellular marrow with more than 30% plasma cells.Endoscopy showed an unhealthy oedematous mucosa with erosions and exposed blood vessels in the stomach and duodenum.He was diagnosed as SMM causing AL amyloidosis.The patient was given proton pump inhibitors.However,he rapidly deteriorated and succumbed to septic shock.
But as he was very angry at what he had been told, he declared that he was going to make an example of this young man, and intended to teach him that even poor travelling pedlars could get justice in his country, and be protected from such lawlessness
The authors have read the CARE Checklist(2016),and the manuscript was prepared and revised according to the CARE Checklist(2016).
The prognosis of gastrointestinal amyloidosis is poor,and mainly depends on the underlying disease and organ involvement.In a study of 155 patients with systemic amyloidosis,24 patients had gastrointestinal involvement and 131 patients had no gastrointestinal involvement[14].Median overall survival in patients with gastrointestinal involvement was shorter(8 mo)than in those without gastrointestinal involvement(16 mo).Our patient has survived for nearly five years after diagnosis.As far as we know,the index case has the longest follow-up and the best prognosis among reported cases of MM and gastrointestinal AL.The good outcome of our patient was probably due to early diagnosis and absence of organ involvement other than the digestive tract.
CONCLUSlON
The dove then flew up on his shoulder and sat there and the prince thanked it, and stroked and caressed12 its white feathers, and kissed its little red beak
FOOTNOTES
Zhao WJ,Jing X,and Zhou X contributed to the manuscript investigating;Liu AL,Ding XL,and Liu H wrote original draft;Tian ZB,Mao T,and Wu J contributed to the reviewing and editing.
Written informed consent from the patient was obtained.
Amyloidosis is diagnosed by histological examination of tissue biopsies of the affected organs with Congo red staining and apple-green birefringence using polarized microscopy.It is necessary to identify the subtype and etiology of amyloidosis for treatment.In our case,AL was confirmed by positive Congo red staining of gastric and colonic tissues.
The overall risk of progression of SMM to MM is about 10% per year in the first 5 years,3% per year in the next 5 years and 1% per year thereafter[12].SMM does not require active treatment as the endorgan damage is absent.Therapy of AL includes traditional chemotherapy(melphalan,prednisone),novel drugs such as protease inhibitors(bortezomib),immunosuppressants(thalidomide,lenalidomide)and autologous stem cell transplantation[7].The treatment of amyloidosis-induced bleeding is difficult.Proton pump inhibitors and somatostatin maybe effective.Endoscopic injection of noradrenaline at the bleeding site can be performed but is often ineffective.Surgical intervention may be required for refractory bleeding for localized lesions[13].Our patient did not have recurrent bleeding after proton pump inhibitors and somatostatin therapy.She then received chemotherapy and was discharged when the symptoms were relieved.
Do not thus afflict yourself, my good master. You have nothing else to do but to give me a bag13 and get a pair of boots14 made for me that I may scamper through the dirt and the brambles, and you shall see that you have not so bad a portion in me as you imagine.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
On physical examination,her tongue was swollen with teeth prints and skin purpura was present in the right neck and periumbilical region(Figure 1).There was mild edema in both lower extremities.
China
Ai-Ling Liu 0000-0003-0165-0710;Xue-Li Ding 0000-0003-4021-2246;Hua Liu 0000-0002-0621-5358;Wen-Jun Zhao 0000-0002-2189-8564;Xue Jing 0000-0001-6957-1811;Xuan Zhou 0000-0002-5888-5329;Tao Mao 0000-0002-5294-5474;Zi-Bin Tian 0000-0002-3211-2934;Jun Wu 0000-0002-8962-9694.
Autumn is the third season of the year, or the season between summer and winter, often called ``the fall. Astronomically46, it begins in the northern temperate47 zone at the autumnal equinox, about September 23, and ends at the winter solstice, about December 23; but in popular language, autumn, in America, comprises September, October, and November (Webster s 1990). Return to place in story.
This story has a postscript10. After thirty years, I called directory assistance and found that Annie Mae still lived in Tuscaloosa. I called her, and later my second husband and I visited her, and I had that chat I never had thirty years ago. What a joy it was! Annie Mae had become a family and children’s worker for the state of Alabama and retired11 in May of 1996.
Xing YX
Filipodia
Xing YX
 World Journal of Clinical Cases2022年7期
World Journal of Clinical Cases2022年7期
- World Journal of Clinical Cases的其它文章
- Relationship between treatment types and blood-brain barrier disruption in patients with acute ischemic stroke:Two case reports
- Ultrasound-guided rectus sheath block for anterior cutaneous nerve entrapment syndrome after laparoscopic surgery:A case report
- Spontaneous dissection of proximal left main coronary artery in a healthy adolescent presenting with syncope:A case report
- Acute esophageal obstruction after ingestion of psyllium seed husk powder:A case report
- Novel mutations of the Alstr?m syndrome 1 gene in an infant with dilated cardiomyopathy:A case report
- Cutaneous leishmaniasis presenting with painless ulcer on the right forearm:A case report