Giant infected hepatic cyst causing exclusion pancreatitis:A case report
2022-03-15 06:04:58TsuneakiKenzakaYuSatoHogaraNishisaki
World Journal of Clinical Cases 2022年7期
lNTRODUCTlON
The gradual dilation of remnant abnormal intrahepatic bile ducts supposedly forms the hepatic duct from the embryonic period[1].The prevalence of simple hepatic cysts is 4.5%-7%[2,3],and they tend to be more common in women than men at a ratio of 1.5:1[4].They are often incidentally observed in adults aged ≥ 40 years who have undergone computed tomography(CT)and ultrasonography[5].
An infected hepatic cyst is a condition characterized by clinical symptoms such as fever and abdominal pain.Routes of infection include the biliary tract,hematogenous,nearby infection foci,trauma,and unknown[5].Overall,the routes of infection are most commonly unknown[5].The risk factors for infected hepatic cysts are female sex,age ≥ 40 years,diabetes mellitus,biliary calculus or stenosis,and post-pancreatic head duodenal surgery[5].A cyst diameter > 10 cm increases the likelihood of exclusion symptoms in adjacent organs[6].However,there are no previous reports involving the pancreas.
The male have so much love for the female, when you wanted to touch the female, he would rush out in a fighting posture3, no matter how far away the female was. Of course they were always close together, and would look at anyone who near by their tank. So if you did it again he quickly responded4 as well. I tried many times, but he always did that to protect the female. Sometimes he used his head to push the female to hide behind the rock in the tank, sometimes he was a little angry and jumped up above the water surface. When he was fighting with you, he looked very violent5, sometimes I wore gloves to try to touch the female, and the male bravely bit my gloves. When the staff fed them the male always looked out as a guard and waited for the female to have the food first …
Herein,we report a case of pancreatitis caused by an infected hepatic cyst.
When they had gone some distance on the road home, the girl turned to her husband and said: Till you step inside the house, be sure you do not look back, whatever you may hear or see
CASE PRESENTATlON
Chief complaints
The authors have read the CARE Checklist statement,and the manuscript was prepared and revised according to the CARE Checklist statement.
I told him he was not the only one who had lost a leg, even if mine was still attached to me. I showed him newspaper clippings of my accident. ‘So if you think I m going to let you feel sorry for yourself for the rest of your life, think again. There is a whole life waiting for us out there! I don t intend to be sorry for myself. But I have enough on my plate as it is, so you d better snap out of it too. And I am not going to carry you-you are going to walk yourself. Grandma giggled12, a surprisingly girlish sound coming from an old lady with white hair.
History of present illness
The patient was an 88-year-old woman who could independently perform activities of daily living.She had previously been diagnosed with polycystic liver disease,with a giant cyst > 10 cm in diameter.She was examined by a local doctor for upper abdominal pain that persisted for 4 d before consultation.She had a fever of 37.4°C,and a blood test showed a C-reactive protein level of 23 mg/dL.She was referred to our hospital for further examination and treatment when abdominal ultrasonography indicated a giant hepatic cyst and intracystic debris.She had a history of hypertension and dyslipidemia.She was taking oral amlodipine 5 mg/d,azilsartan 20 mg/d,and rosuvastatin 2.5 mg/d.Her family history was unremarkable with respect to hepatic or renal cysts.
Then he went away, after saying, Good-by, Beauty; good-by, old man ; and though Beauty was beginning to think with great dismay of her father s departure, she was afraid to disobey the Beast s orders; and they went into the next room, which had shelves and cupboards all round it
Physical examination
Thereafter,the abdominal symptoms,inflammatory response,and elevated levels of pancreatic enzymes improved,and the patient was discharged on hospitalization day 31.No recurrence was observed over the following year.
Laboratory examination
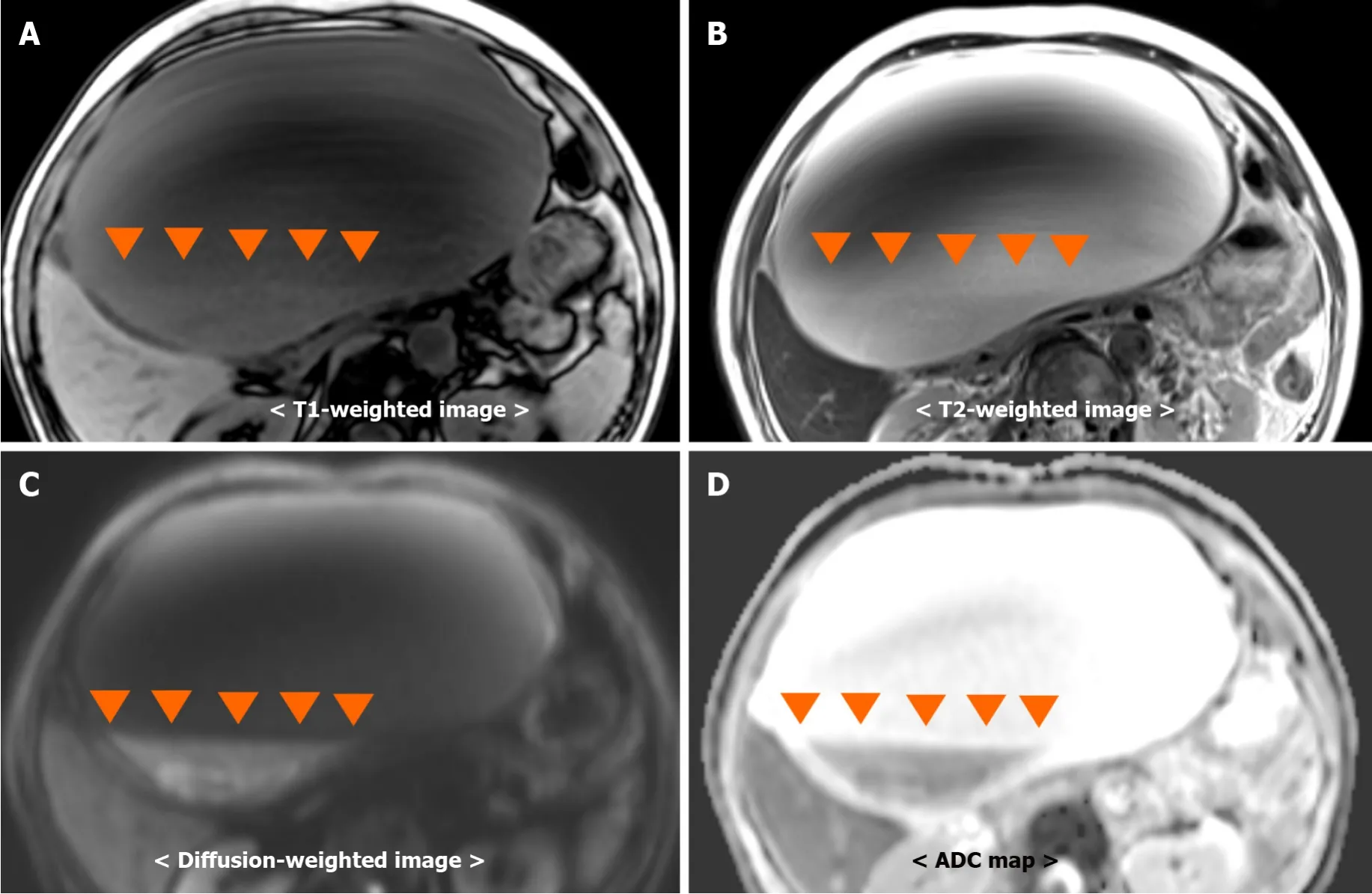
Blood examination showed elevated leukocyte(5300/μL)and neutrophil(66.2%)levels.Similarly,she presented with aspartate aminotransferase level of 18 U/L,alanine aminotransferase level of 15 U/L,lactate dehydrogenase level of 153 U/L,amylase level of 31 U/L,C-reactive protein level of 28.3 mg/dL,and procalcitonin level of 5.89 ng/mL.Other test results are shown in Table 1.
Imaging examinations
When antibiotics are exclusively used to treat infectious hepatic cysts,the treatment success and recurrence rates are 30% and 20%,respectively[9].The treatment success rates of combining antibiotics with percutaneous cyst puncture/drainage or surgery are 65% and 100%,respectively[9].In this case,the giant hepatic cyst location on the hepatic margin made it difficult to install a drain during the first puncture.Therefore,only a single puncture was performed.The symptoms did not improve with antibiotic therapy alone and recurred after cyst puncture.Therefore,surgical fenestration was performed.
FlNAL DlAGNOSlS
The patient was diagnosed with an infected hepatic cyst.
TREATMENT
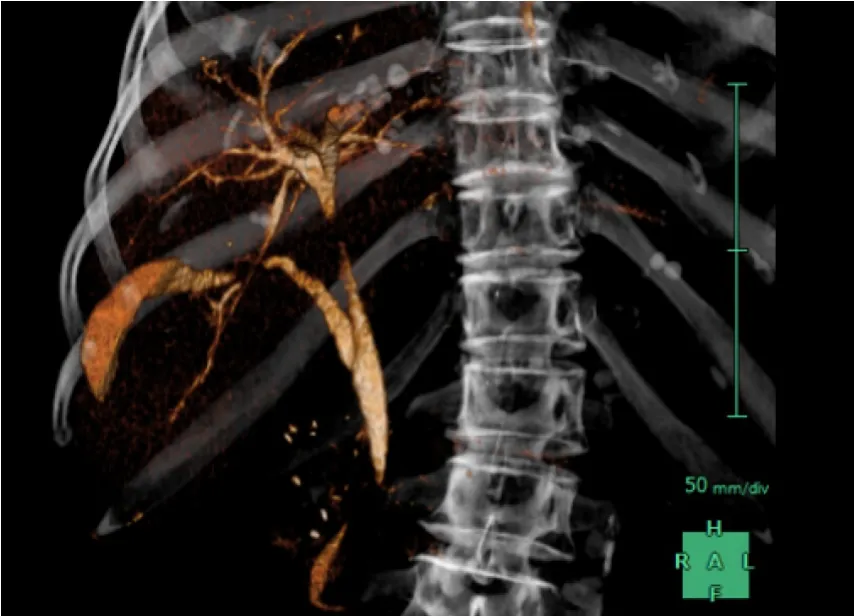
The patient was started on antibacterial therapy with vancomycin and meropenem.Both blood and urine cultures were negative.Despite the antibacterial therapy,her abdominal pain gradually worsened starting around hospitalization day 3.Back pain appeared on hospitalization day 7,and blood amylase and lipase levels increased to 1150 U/L and 850 U/L(reference value;13-55 U/L),respectively.CT showed hepatic cyst growth,signs of pancreatic exclusion,dilation of the pancreatic duct,and increased adipose tissue density around the pancreas(Figure 4).In addition,three-dimensional drip infusion CT cholangiography showed no organic abnormalities in the common bile duct(Figure 5).These findings led to the diagnosis of exclusion pancreatitis.A percutaneous cyst puncture produced 500 mL of purulent fluid.was detected in a culture of the puncture fluid;therefore,the antibiotic was changed to cefmetazole.Despite the use of an effective antibiotic,cyst growth persisted.Therefore,on hospitalization day 20,we performed a laparoscopic hepatic cyst fenestration.Figure 6 shows the clinical course of the patient.
25.The old King: This tale honors age and wisdom through the actions of the old King. He has the experience to see beyond the surface of the events surrounding him and ultimately helps restore the princess to her rightful position.Return to place in story.


OUTCOME AND FOLLOW-UP
Her consciousness was clear during examination.Physical findings were as follows:Blood pressure 160/90 mmHg,pulse 94 bpm/regular,body temperature 37.7°C,respiratory rate 19/min,and SpO2 97%(room air).The upper abdomen was protruded and soft during abdominal examination.No increase or decrease in bowel sounds was observed.The right hypochondriac region was tender,with no rebound pain,Murphy's sign,or pain from liver percussion.
Liver cysts with bacterial infections often have larger diameters[7].A cyst diameter > 10 cm increases the chances of exclusion symptoms in adjacent organs[6].Reported symptoms of exclusion include abdominal pain,nausea,vomiting,obstructive jaundice due to biliary obstruction[5],superior vena cava thrombosis[8],and acute pulmonary embolism[5].Acute pancreatitis is extremely rare,and only a single case report describes it as being caused by a giant non-infected hepatic cyst[6].In this case,pancreatitis improved with puncturing,indicating that the increased hepatic cyst size due to bacterial infection was responsible for acute exclusion pancreatitis.
DlSCUSSlON
Kenzaka T managed the case and redacted and corrected the manuscript;Sato Y and Nishisaki H assisted with redaction,correction,and reconstruction of the manuscript;all authors read and approved the final manuscript.
What I hadn’t counted on were the people with enormous orders who chose to use the drive-thru window, or the women who felt that the coffee was much too creamy, or the men who wanted their iced coffees remade again and again until they reached a certain level of perfection. There were moments when I was exasperated4 with the human race as a whole, simply because I couldn’t seem to please anyone. There was always too much sugar, too little ice, and not enough skim milk. Nevertheless, I kept at it.
Abdominal ultrasonography revealed multiple cysts in the liver,including a giant one(Figure 1).A nonuniform hyperechoic region inside the cyst was considered debris.Abdominal dynamic CT revealed a contrast effect in the hepatic parenchyma around the cyst(Figure 2).There was no ring enhancement indicating an abscess.The maximum cyst diameter was 203 mm,and the main pancreatic duct at the pancreatic tail was slightly dilated.A simple abdominal magnetic resonance imaging showed a fluidfluid level from the debris inside the hepatic cyst(Figure 3).
CONCLUSlON
We reported a case of exclusion pancreatitis associated with the growth of an infectious hepatic cyst.In rare cases,a giant infected hepatic cyst may cause exclusion pancreatitis;therefore,the appearance of symptoms and elevation of pancreatic enzymes should be carefully observed.In case of poor improvement in clinical symptoms and imaging findings with antibiotic therapy alone or when there is exclusion of surrounding organs,percutaneous cyst puncture and drainage or surgical therapy can be considered.Given the possibility of recurrence,close follow-up is recommended.
FOOTNOTES
We report a case of exclusion pancreatitis associated with the growth of an infected hepatic cyst.To our knowledge,this is the second case report of pancreatitis occurring as organ damage associated with hepatic cyst growth.The other study referred to exclusion pancreatitis caused by a non-infected hepatic cyst[6].
Written informed consent was obtained from the patient for publication of this case report and accompanying images.A copy of the written consent is available for review by the Editor of this journal.
The authors declare that they have no competing interests.
Upper abdominal pain,fever.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:http://creativecommons.org/Licenses/by-nc/4.0/
Japan
Tsuneaki Kenzaka 0000-0002-3120-6605;Yu Sato 0000-0002-0797-5973;Hogara Nishisaki 0000-0002-2327-7198.
” It was quite early when she kissed her old grandmother, who was still asleep; then she put on her red shoes, and went quite alone out of the town gates toward the river
Liu JH
A
Liu JH
 World Journal of Clinical Cases2022年7期
World Journal of Clinical Cases2022年7期
- World Journal of Clinical Cases的其它文章
- Relationship between treatment types and blood-brain barrier disruption in patients with acute ischemic stroke:Two case reports
- Ultrasound-guided rectus sheath block for anterior cutaneous nerve entrapment syndrome after laparoscopic surgery:A case report
- Spontaneous dissection of proximal left main coronary artery in a healthy adolescent presenting with syncope:A case report
- Acute esophageal obstruction after ingestion of psyllium seed husk powder:A case report
- Novel mutations of the Alstr?m syndrome 1 gene in an infant with dilated cardiomyopathy:A case report
- Cutaneous leishmaniasis presenting with painless ulcer on the right forearm:A case report