Perioperative anticoagulation and open distal corpora cavernosa shunt in the management of a case of stuttering idiopathic persistent childhood ischaemic priapism
2021-12-31 01:35:28JonathanTeoHanJieLeeJohnYuen
Asian Journal of Urology 2021年4期
Jonathan S.M.Teo ,Han Jie Lee ,John S.P.Yuen ,
a Department of Urology,Sengkang General Hospital,Singapore
b Department of Urology,Singapore General Hospital,Singapore
KEYWORDS Paediatric;Ischaemic priapism;Anticoagulation;Percutaneous distal shunt
Abstract Childhood priapism is a rare entity and there is currently no consensus regarding its contemporary management.The use of perioperative anticoagulation and open distal corporaglandular shunt procedure in the management of childhood priapism has not been reported in the literature.We present a stuttering case of a 13-year-old boy who presented with idiopathic ischaemic priapism lasting 13 h in duration,which recurred despite corporal aspiration and alpha-adrenergic agonist injections,percutaneous distal shunt surgery,and revision of percutaneous distal shunt surgery.He was eventually successfully managed with perioperative subcutaneous enoxaparin,oral aspirin and clopidogrel in conjunction with an Al-Ghorab shunt,which led to sustained detumescence but with spontaneous morning erections.In paediatric patients with sustained childhood priaprism failing stepwise treatments,an Al-Ghorab shunt with perioperative anticoagulation is a viable option.
1.Introduction
Childhood priapism is defined as a prolonged penile erection lasting more than 4 h unrelated to sexual stimulus,in patients younger than 18 years of age[1].Priapism is an emergency,and a delay in treatment can lead to fibrosis of the corpora cavernosa,resulting in penile disfigurement orshortening and erectile dysfunction.There is currently no consensus regarding the management of childhood priapism.In adults with ischaemic priaprism,the use of an Al-Ghorab(open distal corpora-glandular)shunt is an accepted surgical treatment[2-5].While the use of perioperative anticoagulation has been described[6],no studies have been reported on the combination of perioperative anticoagulation and Al-Ghorab shunt in the management of recurrent childhood priapism.We present a stuttering case of a 13-year-old boy who presented with idiopathic ischaemic priapism lasting 13 h,which recurred despite multiple modalities of management,and was eventually managed successfully with an Al-Ghorab shunt in conjunction with perioperative oral aspirin and clopidogrel.Informed consent was obtained from the patient and parents,and all identifiers were removed from all text and pictures included before presentation of this case report.
2.Case report
A 13-year-old Caucasian boy was referred to our Urology Service for spontaneous painful erection persisting for 13 h.He sustained no trauma or pelvic injuries.He was on oral calcium supplements,salbutamol and steroid inhalers for asthma,and there was no history of illicit drug consumption,malignancies,or any haematological disorders such as sickle cell disease(SCD)or leukaemia.
On physical examination,his penile shaft was erect and tender on palpation.The glans penis was soft and normal testes were palpable bilaterally in the scrotum.He had no abdominal masses or inguinal lymphadenopathy.
Initial investigations showed a normal haemoglobin level(13.6 g/dL),white blood cell(10.8×10/L),and platelet count(352×10/L),and his peripheral blood film showed normal erythrocytes.Serum electrolytes and creatinine were normal(58 μmol/L).His prothrombin time and activated partial thromboplastin time were within the normal range.
Prior to our consultation at the Accident and Emergency Department,he was initially treated with oral pseudoephedrine,and ice packs were applied to his penis in an attempt to achieve detumescence.As the initial management failed to cause resolution of the priaprism,an urgent urology consult was called for.A clinical diagnosis of ischaemic priapism was made based on history and examination findings,and immediate penile aspiration using an 18-gauge butterfly needle under aseptic technique and local anaesthesia was performed.A total of 105 mL of dark red deoxygenated blood was aspirated(Fig.1)until bright red blood was seen in the aspirate.Cavernosal blood gas analysis showed the following:pH 7.46,pO62.7 mmHg,pCO22.9 mmHg,base excess-5.6 mmol/L,bicarbonate 19.7 mmol/L,and SpO92.7%.This represented a mixed ischaemic and non-ischaemic(venous-arterial)picture likely because the specimen was not from initial aspirate but obtained after repeated aspirations.Penile aspiration initially resulted in rapid detumescence,but his penis became erect again within minutes.Intracavernosal injections of 100 mg of phenylephrine were subsequently administered at 5-min intervals up to 1 mg.Although there was partial detumescence at the end of the procedure,the erection recurred rapidly and persisted.Bedside penile Doppler ultrasound showed undetectable arterial flow and signal in the bilateral cavernosal arteries.The decision was then made for a shunt procedure under general anaesthesia after counseling the patient and his parents and informed consent was obtained.

Figure 1 Aspiration of dark red blood using large bore 18-gauge butterfly needle inserted at the peno-scrotal junction at 9 o’clock position.
A bilateral percutaneous distal(glandular-corporal)T shunt was performed 14.5 h from presentation(Fig.2).Intraoperatively,upon deepening of the glans incision into the tip of the corpora cavernosa bilaterally,dark red deoxygenated blood was seen to spurt out and immediate detumescence was achieved.Additional dark red blood was“milked”out through the incision and detumescence was observed for 15 min before the glans incision was closed with interrupted 3-0 absorbable sutures.A 12 Fr two-way Foley indwelling catheter was inserted.
However,his priapism recurred on review 6 h after the shunt procedure,and penile ultrasound demonstrated poor flow and absent Doppler signal in the cavernosal arteries.The patient was counselled for and underwent a revision of the shunt.Tunnelling of the corpora cavernosa was performed by passage of Hegar dilators up to 4 Fr through existing glans incisions to proximal cavernosa bilaterally.Detumescence was achieved almost immediately and observed for 15 min before closure of the incisions.Postoperatively,a referral to the Haematology service was made.Blood film showed normochromic and normocytic red blood cells and haemoglobin electrophoresis was unremarkable.A magnetic resonance imaging of the abdomen and pelvis revealed no mass or secondary features of advanced SCD.
His priaprism recurred again the following day.The possibility of premature shunt closure,possibly by blood clots at the corpora-spongiosum site was considered,and a dose of subcutaneous enoxaparin and oral acetylsalicylic acid were given before proceeding to a definitive shunt procedure.An open Al-Ghorab shunt(Fig.3)was performed under general anaesthesia.Intraoperatively,a small clot was observed at the corpus spongiosum.Postoperatively,he was kept on an anticoagulation regimen of subcutaneous enoxaparin for 48 h,and oral acetylsalicylic acid(50 mg once daily)and clopidogrel(37.5 mg once daily)for a week.

Figure 2 Bilateral percutaneous distal T shunt after closure of incisions on glans penis.
There were no further episodes of priapism and a repeat Doppler ultrasound the next day showed return of arterial perfusion to the bilateral corpora cavernosa.He was discharged on Day 5 of admission and reviewed in clinic 2 and 4 weeks later.He remained well and reported spontaneous morning erections 1 month postoperatively.
3.Discussion
In ischaemic priapism,the pathophysiology involves an occlusion of venous outflow and subsequent cessation of arterial inflows in the corpora cavernosa.Hypoxia,hypercarbia,and acidosis occur resulting in corporal fibrosis and erectile dysfunction[3].
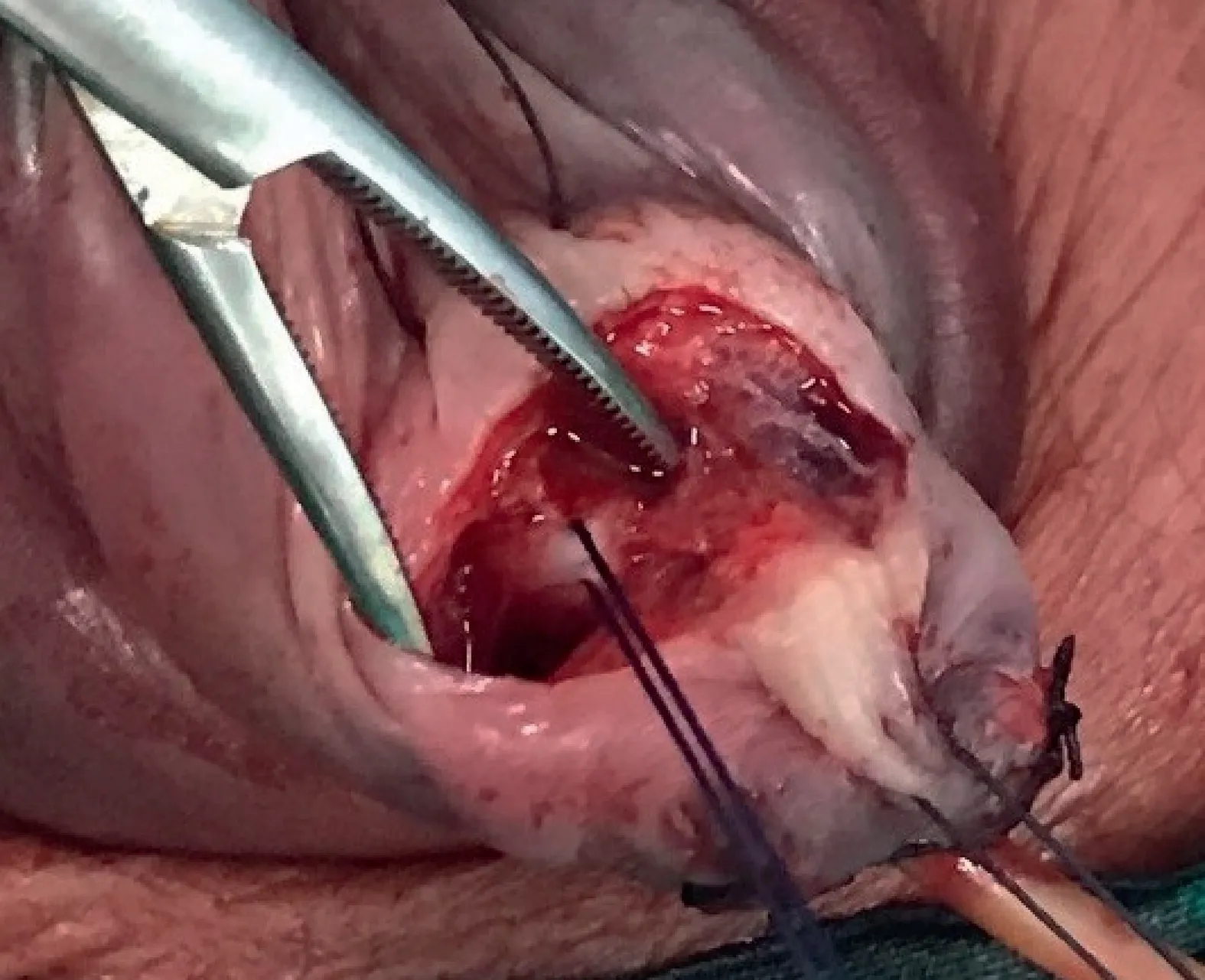
Figure 3 Open distal Al-Ghorab shunt with the white tunica albuginea layer covering the corpora cavernosa.
Childhood priapism is rare.Population studies in adults have estimated the incidence to be between 0.34 per 100 000 person-years in Finland[7]and 1.5 per 100 000 person-years in the Netherlands[8].There are no generalizable data on its prevalence.The commonest causes of priapism in children are SCD(65%),leukaemia(10%),trauma(10%),idiopathic(10%),and pharmacologicalinduced(5%)[9].In paediatric population with SCD,the reported prevalence was up to 3.6%[10],and the incidence in paediatric SCD clinics is estimated to be between 2%and 6%[11].This patient was investigated for SCD,haematological dyscrasias,and other diseases that might predispose him to priapism,all of which were negative.In addition,medications like antidepressants,anticoagulants and antihypertensives,as well as ilicit drugs can cause priapism,but he was not on any such medication and there was no history of substance abuse.Although animal/insect bites might be a potential cause as well,it was unlikely in this case.Thus,the cause of ischaemic priapism was likely idiopathic.
Although the management of ischaemic priapism in adults has reached consensus,there remains no clear guidelines for childhood priapism.A review article evaluated all 293 publications on childhood(defined as younger than 18-years-old)priapism searched for in the English literature from 1980 to 2013 and suggested a step-wise treatment approach of ischaemic priapism to consist of initial analgesia,“first aid”:Exercise,urination,cold bath,ejaculation,followed by corporal aspiration and 0.9%saline lavage with or without sympathomimetic injections[1].If these steps were unsuccessful,the following will be considered:Bilateral distal T shunts,mid-corporal corporotomies with or without“Snake maneuver”(dilatation of shunts using a Hegar dilator)and lastly Quackels Shunt.
In this patient,the sequential treatment protocol of corporal aspiration and alpha-adrenergic agonist injections,percutaneous distal shunt surgery,revision of percutaneous distal shunt surgery with dilatation,and lastly perioperative anticoagulation with Al-Ghorab shunt,was employed with successful sustained detumescence.Although the use of Al-Ghorab shunt is widely accepted for treatment of ischaemic priapism in adults[2-5],there has been no reports on its use in treating childhood priapism.
The use of anticoagulation to maintain fistula patency in adults is controversial and has not been reported in children.Lue and Garcia[6]proposed that post-shunting recurrence in ischaemic priapism could be due to postoperative thrombosis of the newly created shunt.Damages to tunica albuginea and endothelial lining of the corpus cavernosum during creation of the shunt could result in the propagation of the coagulation cascade.Therefore,use of perioperative anticoagulation for shunt surgery in the treatment of ischaemic priapism was proposed with the aim to keep the newly created shunt patent,to allow continuous high blood flow and thereby preventing thrombus formation.The author suggests preoperative oral Aspirin 325 mg and subcutaneous Heparin injection 5 000 units before any shunting procedure,followed by postoperativeoral aspirin 81 mg daily for 2 weeks in adults.In our paediatric case,the anticoagulation regimen was modified for his age and weight.This likely played an important role in maintaining shunt patency and prevented priapism recurrence.
In summary,ischaemic priapism in the paediatric population shares the same basic pathophysiology as in adults.The efficiency in achieving sustained detumescence would govern postoperative outcome[12].This case involving a paediatric patient illustrated the use of a stepwise treatment approach to recurrent priapism that culminated with Al-Ghorab shunting with a dose-adjusted perioperative anticoagulation regimen to prevent premature shunt closure,likely a factor leading to failure of earlier shunt procedures.This case illustrated is one of a few employing a surgical Al-Ghorab shunt in the paediatric population,and despite the apparent success in our experience,it would certainly be beneficial to see more paediatric cases with a longer follow-up in order to determine the true feasibility of this management protocol for persistent priaprism.
Author contributions
Study concept and design:Jonathan S.M.Teo,Han Jie Lee,John S.P.Yuen.
Data acquisition:Jonathan S.M.Teo,Han Jie Lee.
Data analysis:Jonathan S.M.Teo,Han Jie Lee.
Drafting of manuscript:Jonathan S.M.Teo,Han Jie Lee.
Critical revision of the manuscript:John S.P.Yuen.
Conflicts of interest
The authors declare no conflict of interest.
 Asian Journal of Urology2021年4期
Asian Journal of Urology2021年4期
- Asian Journal of Urology的其它文章
- Radical cystoprostatectomy with orthotopic neobladder for a case of treatment emergent neuroendocrine prostate cancer presenting as bladder mass with hematuria-a rare instance of tumor remission after local control
- Late upper urinary tract urothelial carcinoma following radical cystectomy,presenting as page kidney
- Metachronous chest wall metastasis from clear cell renal cell carcinoma-A rarity
- Effect of tamsulosin versus tamsulosin plus tadalafil on renal calculus clearance after shock wave lithotripsy:An open-labelled,randomised,prospective study
- A novel spherical-headed fascial dilator is feasible for second-stage ultrasound guided percutaneous nephrolithotomy:A pilot study
- Impact of COVID-19 on endourology surgical practice in Saudi Arabia:A national multicenter study