Impact of COVID-19 on endourology surgical practice in Saudi Arabia:A national multicenter study
2021-12-31 01:35:26AblRmAliYyGzwniIbrimAlowiAzrMommAlomrAmAlzrniOssmAlsowynWissmKmlAbulrmnAllytAmBuisAbulzizAltunynAlzrniTrkKmlFkAimnAlSolumnyBinHmri
Asian Journal of Urology 2021年4期
Abl Rm Ali ,Yy Gzwni ,Ibrim Alowi ,R A.Azr ,Momm Alomr ,Am Alzrni ,Ossm Alsowyn ,Wissm Kml ,Abulrmn Allyt ,Am Buis ,Abulziz M.Altunyn ,M.Alzrni Trk ,Kml Fk ,Aimn Al-Solumny ,S Bin Hmri
a Urology Department,King Saud Medical City,Riyadh,Saudi Arabia
b Urology Department,Faculty of Medicine,Tanta University,Tanta,Egypt
c Devision of Urology,King Abdullah International Medical Research Center,College of Medicine,King Abdulaziz Medical City,King Saud Bin Abdulaziz University for Health Science,Division of Urology,King Abdulaziz Medical City,Riyadh,Saudi Arabia
d Urology Department,Faculty of Medicine,King Abdulaziz University,Jeddah,Saudi Arabia
e Department of Surgery,College of Medicine,King Saud University and King Saud University Medical City,Riyadh,Saudi Arabia
f Urology Department,Price Sultan Military Medical City,Riyadh,Saudi Arabia
g Urology Department,King Fahd Hospital,Imam Abdulrahman Bin Faisal University,Dammam,Saudi Arabia
h Urology Department,King Fahd Hospital,Jeddah,Saudi Arabia
KEYWORDS COVID-19;Endourology;Saudi Arabia
Abstract Objective:To identify the impact of COVID-19 on endourology surgical practice in Saudi Arabia.
1.Introduction
The World Health Organization(WHO)has announced the novel coronavirus 2019(COVID-19)as a worldwide pandemic on March 11,2020[1].Currently,the corona COVID-19 is affecting 216 countries and territories around the world,and the numbers of new cases and deaths are increasing rapidly.On July 14,2020,more than 13 340 000 confirmed cases and more than 578 000 deaths have been reported worldwide.In the Kingdom of Saudi Arabia(KSA),the number of confirmed cases and deaths due to COVID-19 infections exceeded 273 800 and 2280,respectively[2].This rapid increase of the infection rate has overwhelmed and negatively affected all healthcare systems.Additionally,most countries have taken several preventive and lockdown measures to combat the ability of coronavirus to spread[2,3].The important measures taken by the kingdom were suspension of the seasonal minor Umrah pilgrimage for national and international worshippers,and closure of mosques all over the country.Additionally,a partial curfew on March 23,and then a full curfew on 6 April 2020 to 21 June 2020 have been established between cities.
The COVID-19 pandemic represents a major challenge and threat to the healthcare systems all over the world.There has been a dramatic change in the medical and surgical priorities.To save the hospitals’facilities and resources for urgent cases,most of the outpatient’s activities and elective procedures have been postponed.Additionally,most of hospitals in the affected countries have adopted sufficient protection strategies and provided the healthcare workers with personal protective equipment(PPE)when dealing with COVID-19 patients to guard against infection[4].
Of note,the practice patterns of urologists for the management of different urinary tract disorders have been markedly changed due to COVID-19 pandemic.Recently,the European Association of Urology(EAU)guidelines office rapid reaction group has updated their recommendations to guide the urologists across the globe in the management of urological conditions during the current COVID-19 pandemic[5].Regarding the endourology surgical practice,several researchers have proposed different clinical algorithms,recommendations,and triages to categorize urinary stones treatment according to priority and urgency to interfere[6-9].The European Association of Urology Section of Urolithiasis(EULIS)collaborative research working group conducted a survey including 60 participants from 20 different countries whose main area of expertise was stone urinary disease.Almost half of the respondents changed their elective surgical treatment approach by 90%-100%after COVID-19;more than 85%of them reported a decrease of more than 50% in the workload of outpatient clinic;and 90% tended to change their treatment strategy for positive COVID-19 patients by drainage of the collecting system followed by an elective intervention later on[7].
The above-mentioned guidelines,algorithms,and surveys are of crucial importance to guide the treatment decision making by urologists during the COVID-19 pandemic.However,the real figures of how the COVID-19 affected the endourology surgical practice are still unknown and literature data are lacking in this regard.Thus,we aimed in the present study to determine the actual impact of COVID-19 on the endourology workload in KSA tertiary endourology centers.
2.Material and methods
2.1.Study ethics and design
The study protocol was approved by the local Medical Ethics Committee at King Saud Medical City and other participating centers(approval number:H1RI-09-082002).The study was designed as a retrospective national multicenter study.
2.2.Study population
The study population consisted of records of patients who received consultations,medical or surgical treatments at the urology departments of seven major hospitals located in the three largest cities of KSA(Riyadh,Jeddah and Damam).All hospitals are tertiary referral centers,which receive patients from surrounding hospitals and cities.
2.3.Data collection
We collected data regarding the urology outpatient department(OPD)visits and the endourology workload activity.The total number of OPD visits,the total number,and types of endourology surgical procedures(i.e.electiveand emergency)were gathered.The common types of elective endourology surgical procedures were assigned as follow:Percutaneous nephrolithotomy(PNL),retrograde intrarenal surgery(RIRS),ureteroscopy(URS),extracorporeal shockwave lithotripsy(SWL),transurethral resection of the prostate(TURP),transurethral resection of bladder tumor(TURBT),and cystoscopy.Cystoscopy records included several procedures such as injection therapies,JJ-stent insertion,removal or exchange,diagnostic cystoscopy,visual internal urethrotomy(VIU),and retrograde pyelography.Similarly,the records of emergency endourology surgical procedures were retrieved,such as interventions for treatment of urolithiasis,frank hematuria,suprapubic catheter(SPC)insertion,percutaneous nephrostomy(PCN)insertion,and pyelonephritis.
2.4.Study duration
We collected the data over two periods of time,from January 1,2019 to April 30,2019,and from January 1,2020 to April 30,2020.
2.5.Study outcome measurements
The study endpoints were to analyze the trends,absolute number changes,and percentage(%)number changes of the OPD visits,and endourology workload in the first third of the year 2020 to compare with those in the same period of time during the last year,as well as during the full curfew time i.e.April 2020 compared to April 2019.
2.6.Statistical analysis
The absolute number change was calculated by subtracting the number of cases in 2019 from the number of cases in 2020.The percentage(%)number change was calculated by using the following formula=([2020’s number of cases-2019’s number of cases]÷2019’s number of cases)100.We used Chi-square test to compare the difference of OPD and endourology workload in the year 2019 versus that in the year 2020.Statistical significance was set at p-value of<0.05.All statistical analysis was performed using SPSS version 25 software(IBM SPSS Statistics,IBM Corp.,Armonk,NY,USA).
3.Results
The total number of OPD visits was approximately 46 093.The number of OPD visits in January-April 2020 was significantly lower than January-April 2019(19 499 vs.26 594,p<0.001)(Table 1,Fig.1A).The number of OPD visits in March 2020(4306)was compared to that in the same month last year(6255),with an absolute change of-1949 and a reduction rate of 31.2%(Table 2).In April 2020,the number of OPD visits has markedly decreased compared to that in April 2019(from 7055 to 1512,with a reduction rate of 78.6%)(Table 2).Among April OPD visits,1373(90.8%)were virtual clinics and carried out thought telephone consultations and 139(9.2%)patients had to visit the outpatient clinics by themselves(Fig.1B).
There were a total of 5013 elective endourology surgical procedures.The total number of elective endourology surgical procedures in the first third of 2020 was significantly lower than that in the same period of the last year(1988 vs.3025,p<0.001),with a reduction rate of 34.3%(Table 1,Fig.2A).Of note,there was a decrease by 38.1%in the number of elective endourology procedures in March 2020(465 procedures)compared with that in March 2019(751 procedures),while a maximum drop of 84.1% was noted in the number of elective procedures in April 2020(756 procedures)compared to that in April 2019(120 procedures).
Regarding the types of elective endourology surgical procedures performed in the full curfew period(i.e.April 2020),some procedures almost have stopped such as PNL,SWL,and TURP,with a decline by 94.2%,98.5%,and 93.8%,respectively.There were marked decreases of 78% in ureteroscopy and retrograde intrarenal surgery(URS/RIRS),and 85.5% in cystoscopic procedures,while TURBT had a mild drop by 41.4% compared to the same month last year(Table 3,Fig.3A).During the curfew time,most of elective cases 102/120(85%)were performed as day surgery/outpatient procedures,compared to 332/756(43.9%)in April 2019.
Of note,the total number of emergency surgical procedures in the first third of 2020 has fallen by 9.3%compared to the first third of 2019;however,this decrease was not statistically significant(p=0.286)(Table 1,Fig.2B).In March,2020,63 emergency surgical procedures were performed compared to 60 in the same month last year,with a reduction rate of 4.8%.While in the full curfew period(i.e.April 2020),57 emergency surgical procedures were performed compared to 76 in the same period last year,with a decrease rate of 25%(Table 3).During the full curfew period,urolithiasis was the commonest pathology presented to the emergency room,followed by hematuria(21.1%),bladder outlet obstruction(BOO)treated by SPC insertion(17.5%),and others(8.8%)(Fig.3B).Among urolithiasis disorders,nine patients(28.1%)had calcular anuria,and active stone treatment was performed 12.5%,of the patients.while temporarily drainage of the collecting system was performed in the remaining patients,either through JJ-stent insertion(59.4%)or nephrostomy tube(NPT)insertion(28.1%).
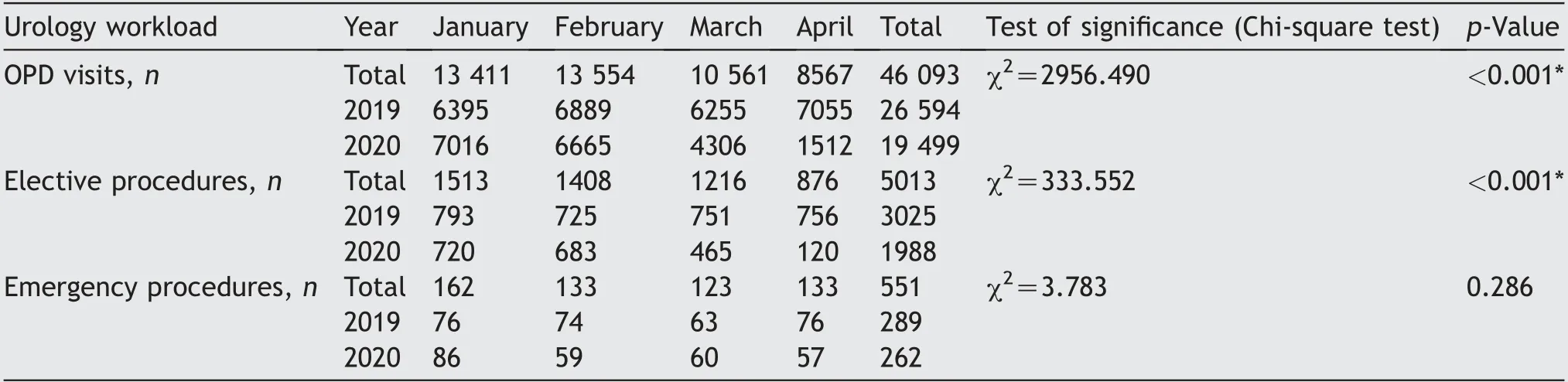
Table 1 The difference of the OPD visit and endourology work volume performed in first third of the year of 2019 and 2020.
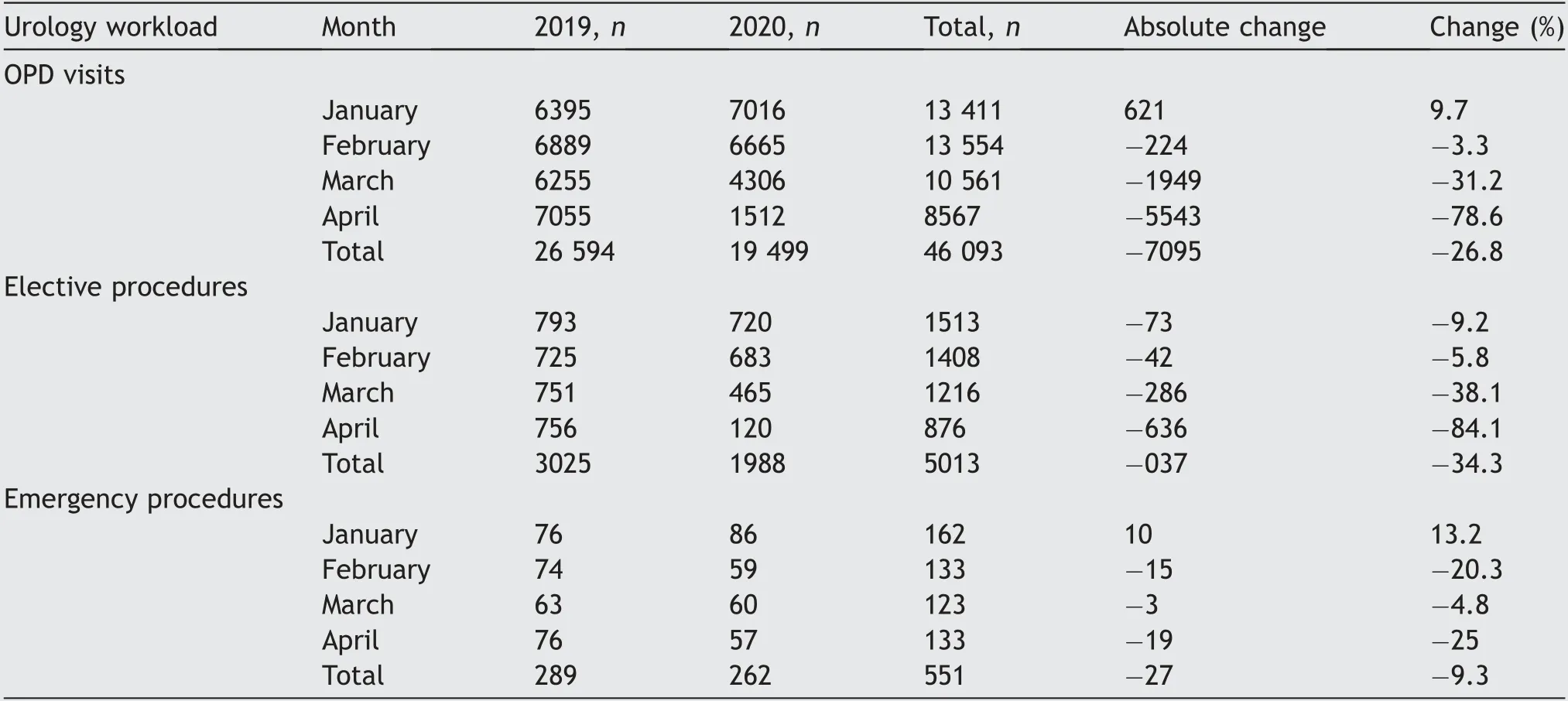
Table 2 The absolute and percentage(%)change of the OPD visits and endourology work volume performed in first third of the year of 2019 and 2020.
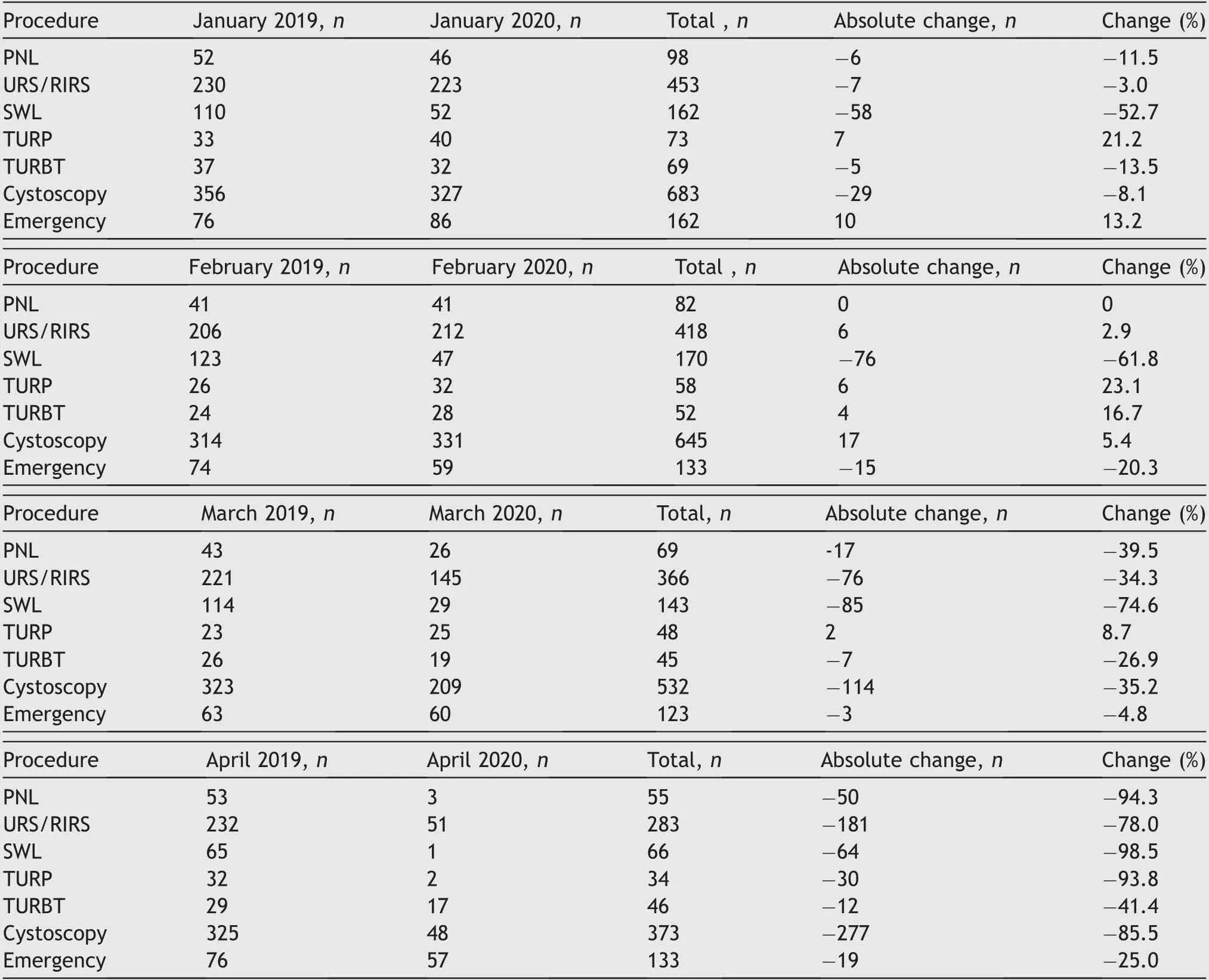
Table 3 The absolute and percentage(%)change between the type of endourology surgical procedures performed in first third of the year of 2019 and 2020.
4.Discussion
The novel corona virus was first reported by WHO in March 2020[1,10].And since that time,COVID-19 is spreading rapidly worldwide,disrupting the healthcare services,and jeopardizing the medical system’s ability to respond to routine patients’needs.In the United States(US),a recent report based on analysis of more than 2 000 000 patient visits from 228 hospitals in 40 states revealed that there was a 54.5%decrease in the number of patients who sought care in hospitals during a 2-week period in March and April 2020.There was a 57%,55%,and 37% decline in cardiology volume,breast health volume,and cancer care,respectively.A larger decline was experienced in other subspecialties.Ophthalmology,gynecology,orthopedics,otolaryngology,urology,and vascular fell by 81%,75%,74%,72%,62%,and 59%,respectively.Additionally,COVID-19 has affected the US health care economy,and the report showed that hospitals are losing$60 billion per month[11].
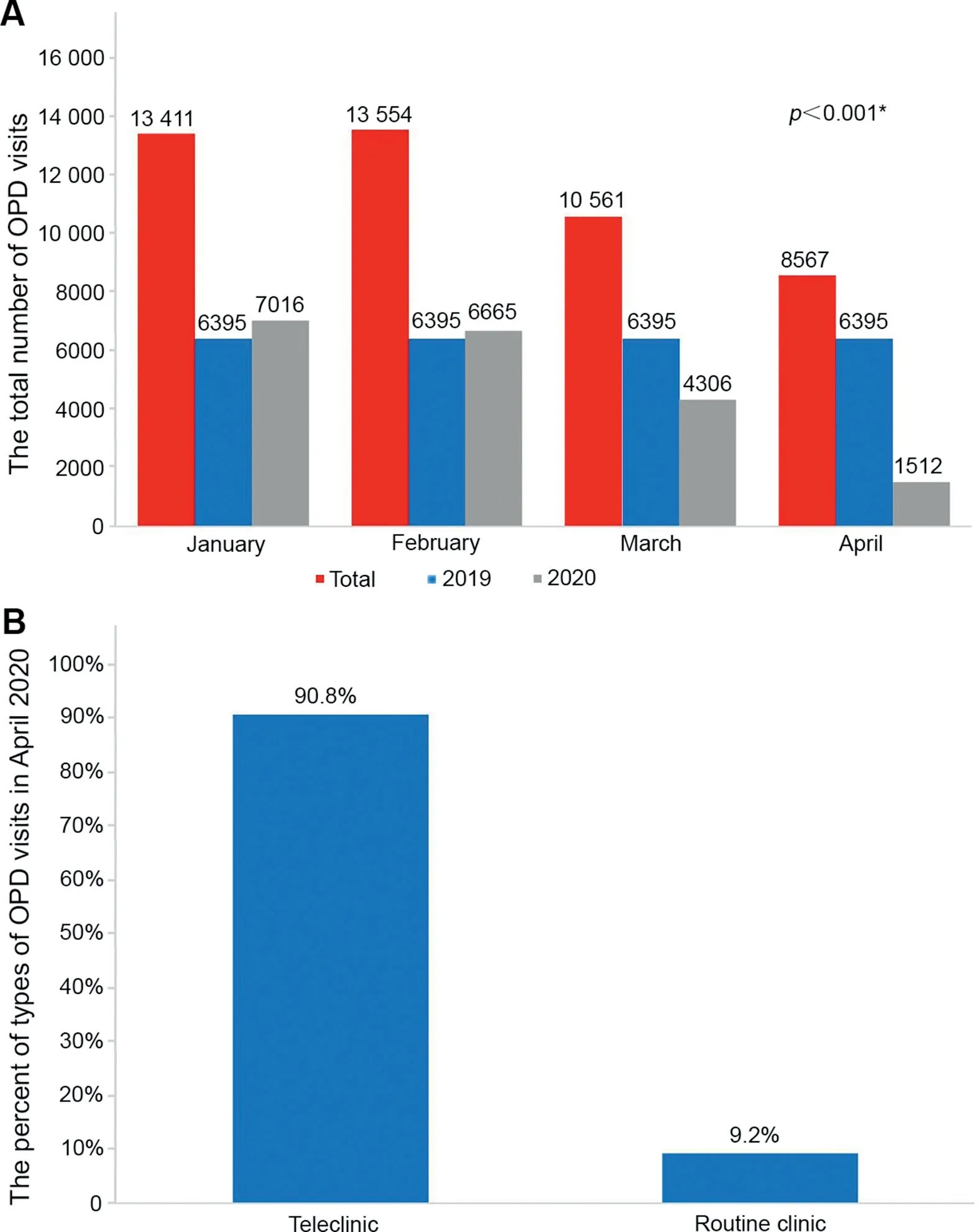
Figure 1 The total number of OPD visits in the first third of 2019 and 2020(A),and the percent of types of OPD visits in April 2020(B).OPD,outpatient department.
A recent report by Naspro and Da Pozzo[12]from Bergamo,Italy,showed that two-thirds of the hospital beds were occupied by patients with COVID-19 within 10 days from the first reported case.The urology surgery volume was reduced by 30% within 15 days,and then there was a total shut-down on March 19,2020.Even the ability to perform some emergency urological surgeries has been limited by the lack of anesthesiologists,ventilators,and operating rooms,which are being used for critically ill patients[12].As hospitals are overwhelmed with COVID-19 patients,many hospitals have begun to prioritize the surgical cases to preserve the hospital beds and(personal protective equipment)PPEs,maintain emergency surgical capabilities,and keep patients and health care workers safe[8].
KSA announced first case of coronavirus on March 2,2020.Since that time,the numbers of daily new cases and deaths are increased gradually;on July 14,2020 more than 273 800 new cases and more than 2280 deaths were reported,placing KSA the 4th among Asian countries and the 14th worldwide most affected countries by COVID-19[2].Our study showed that OPD and elective endourology surgical workload in KSA reduced by more than 75% during April 2020 compared to April 2019,i.e.during complete lockdown time.Although we included analysis of April month only,nevertheless,we do not expect change or recovery of work volume in OPD clinics and number of surgical procedures during May and June months,as these months together with July represent the peak of COVID-19 infection in KSA as shown in Fig.4.
During COVID-19 pandemic,all clinics should be converted into a virtual/telephone clinic to keep our patients at home and to reduce the risk of cross contamination.An active clinic environment increases potential exposure of patients and health care personnel and violates social distancing.Telehealth is a safe and effective telecommunication that will allow complete virtual OPD evaluations soon[13,14].In our study,the OPD visits in the full curfew period declined by 78.6%compared to April 2019,and 90.8%of these visits were teleclinics through telephone consultations.In KSA,we implemented several measures to reduce the OPD visits.Scheduled OPD visits were reviewed;patients with stable conditions were consulted via telephone and rescheduled within 3-4 months;and then prescriptions were delivered to them.In our OPD clinics,we prioritized patients with obstructive uropathy,known or suspected malignancy,and those who were operated recently.
Recently,several researchers published recommendations to help prioritize urological procedures during the COVID-19 pandemic[5-9,15,16].A recent systematic review of 14 urology guidelines and recommendations for standard of patients’care during the COVID-19 pandemic has been published and differences among the guidelines were minimal.According to nine guidelines that addressed endourology surgical practice,obstructed infected kidneys should be immediately decompressed,whereas non-obstructing urinary stones and stent removal should be rescheduled[16].Of note,the EAU guidelines classified urological diseases into four categories according to their surgical priority:Low priority(i.e.clinical harm very unlikely if postponed for 6 months),intermediate priority(i.e.clinical harm possible if postponed for 3-4 months,but unlikely),high priority(i.e.clinical harm very likely if postponed for>6 weeks),and emergency(i.e.lifethreatening conditions)[5].Others framed their recommendations for urological surgery triage based on the rationale of proceed or delay surgery[9].In addition,several triage systems have been introduced based on recommended surgical priority tiers[6,8].Metzler et al.[6]categorized the urgency for prioritization of urinary stone procedures into five groups from 0 to 4.Cases with life-or organ-threatening conditions such as obstructing ureteral stone in a solitary kidney,with infection,intractable symptoms,or bilateral obstructing ureteral stones,were defined as group 0-emergent,and must be immediately resolved in<24 h,either with drainage or treatment.In the contrary,cases with non-obstructing asymptomatic renal stones and majority of stones requiring PNL,were defined as group 4-postpone and should receive no treatment[6].Of note,the delay in management of obstructed infected kidney can lead to severe septic complications and increase the workload on emergency services.Up to 15% of these patients need(intensive care unit)ICU admission,and the mortality rate may reach up to 10%[17].
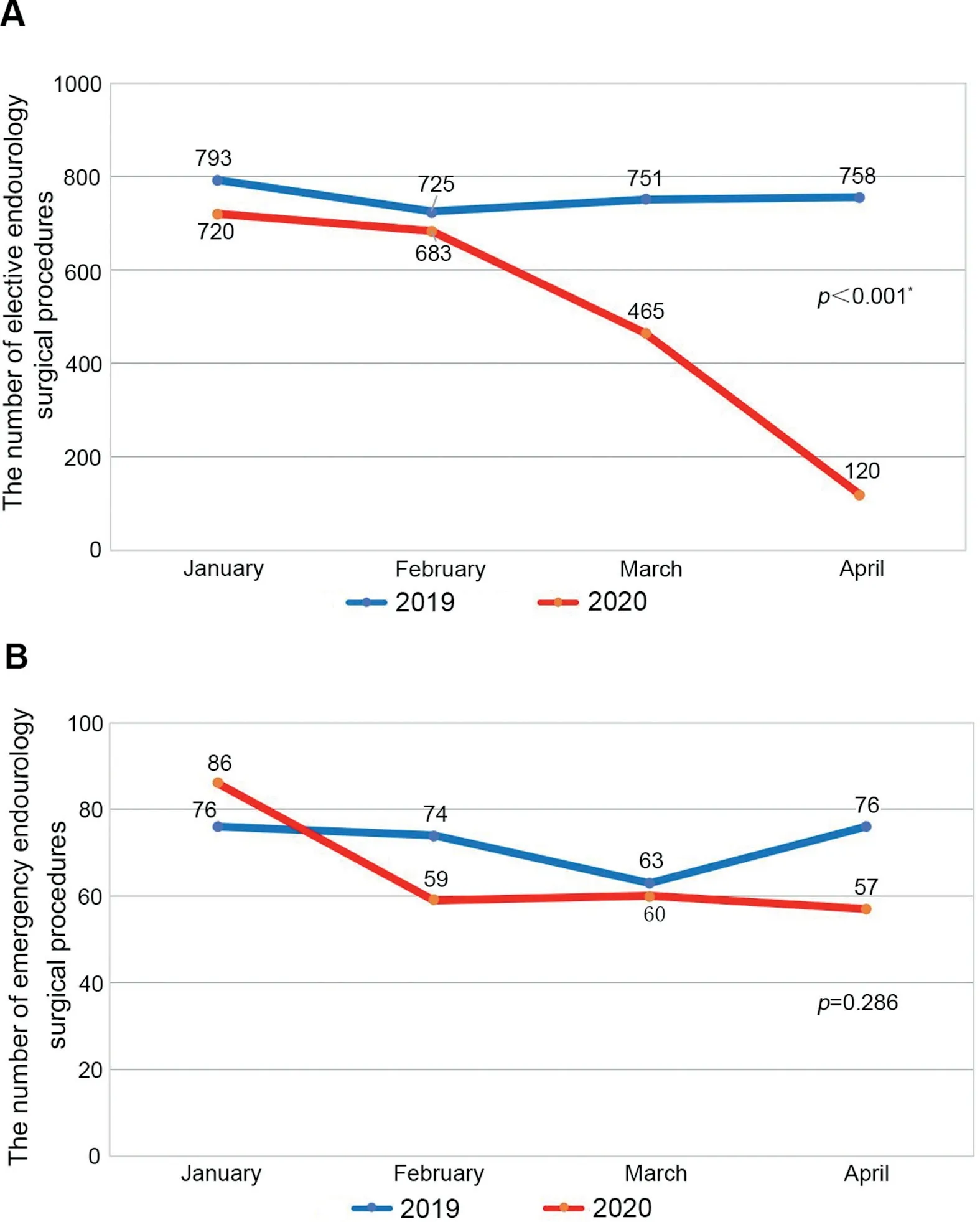
Figure 2 The number of elective(A)and emergency(B)endourology surgical procedures in the first third of 2019 and 2020.
Notably,the number of elective endourology surgical procedures decreased by 84.1%-120 procedures during the full curfew period compared to that in April 2019.Among them,the majority(85%)were day surgery or outpatient procedures such as URS,RIRS,and cystoscopy.Only three(2.5%)PCNL procedures were performed,as we preferred to choose less invasive procedures in the management of renal stones(e.g.RIRS or JJ-stenting),to make the hospital stay short and reduce the patients’risk of contracting COVID-19 during their hospital stay.Metzler et al.[6]introduced a new stone care triage during COVID-19 at the University of Washington.They recommended that most renal stones requiring PNL to be postponed and PCNL maybe indicated if there are recurrent infections,indwelling nephrostomy tube with tube-related complications,or chronic renal deterioration.
Interestingly,we performed one SWL and 51 URS/RIRS procedures during the curfew time,with a reduction of 98.5%and 78%compared to those in April 2019,respectively.In the time of COVID-19 and if we decide to treat an elective case,we preferred to choose the treatment with a high stone-free rate and less retreatment rate,for example,if a patient had a small renal stone that could be treated by either SWL or RIRS.Although SWL seems an ideal option for patients and may use less PPE for a single procedure compared to RIRS,and RIRS procedure was preferred in our hospitals,due to its higher stone-free rate compared to SWL,and thus lower the need for auxiliary treatments and hospital readmissions during COVID-19 pandemic[18].
Our study showed that the number of elective TURBT procedures during the curfew time were 17 while 29 in the same period last year,with a change rate of-41.4%.Indeed,radical treatment for patients with muscle invasive bladder cancer(MIBC)should not be delayed and were given a high priority to treat in recent COVID-19 recommendations[9].Delayed cystectomy for MIBC by 90 days was associated with decrease in overall survival and progression free survival[19,20].In patients with suspected cT1 bladder tumors(i.e.very high risk non-MIBC),solid bladder tumors,and actively bleeding tumors,TURBT is strongly recommended to be performed as an outpatient procedure without delay[9,21].Generally,cT1 tumors are understaged in up to 50% of patients,and this represents a significant risk of missed MIBC[22].
On the other hand,21.1% of the emergency procedures in our study were for management of hematuria,including diagnostic cystoscopy,clot evacuation,and bleeding control.Of note,clot retention was classified as tier 0(i.e.emergency intervention is needed)in the triage system of Cleveland clinic[8].In a recent triage system of officebased urology procedures,Katz et al.[15]recommendedperforming diagnostic cystoscopy and full evaluation without delay for assessment of patients with frank hematuria,as diagnostic yield of bladder cancer and upper tract malignancy is high in this group of patients.In the setting of microscopic hematuria with risk factors(such as smoking,occupational/chemical exposure,and irritative voiding symptoms),unless the patient has symptoms,consideration should be given to deferring the evaluation up to 3 months[15].
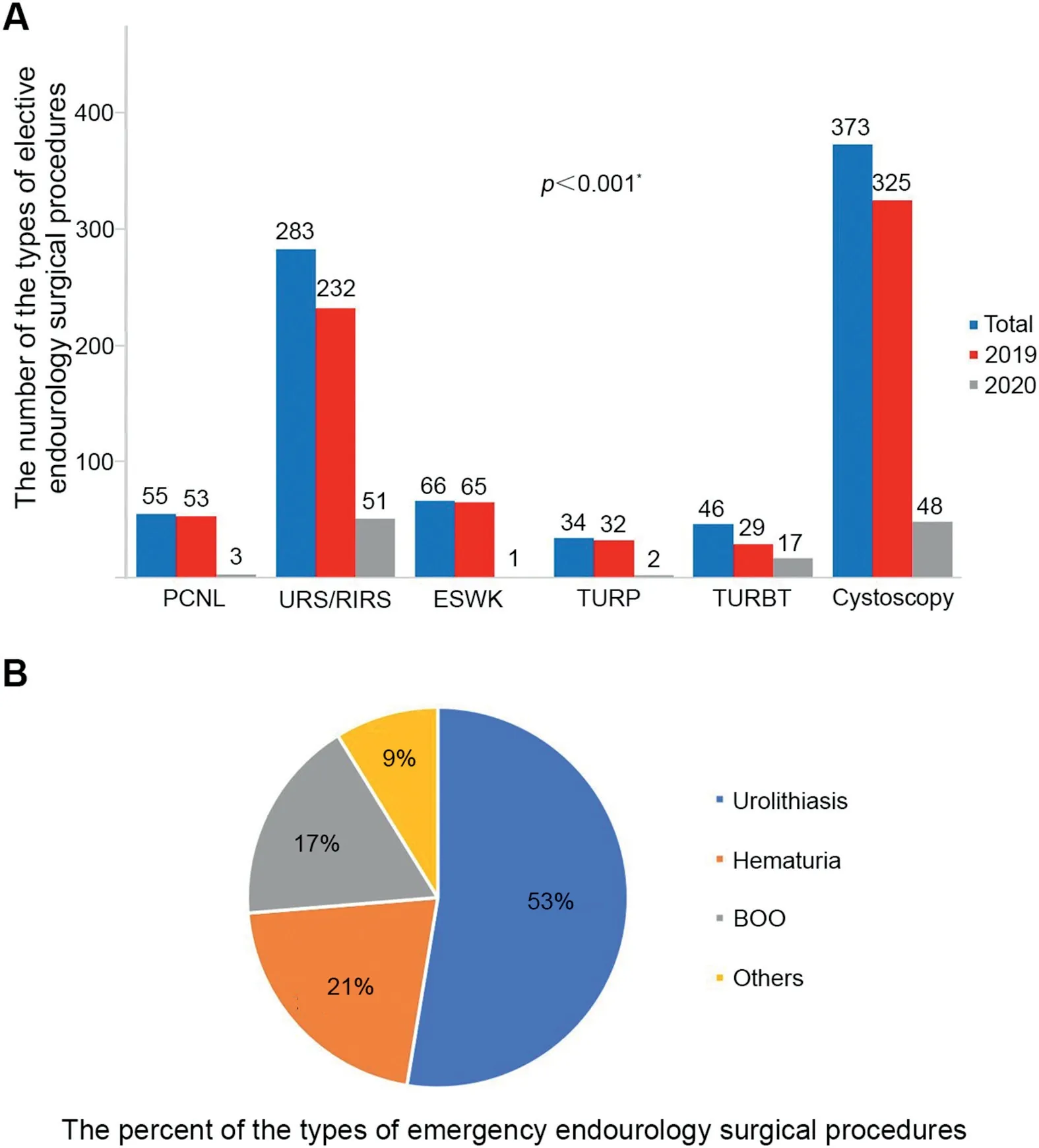
Figure 3 The statistical results of endourology surgical procedures.(A)The number of the types of elective endourology surgical procedures;(B)The percent of the types of emergency endourology surgical procedures.PCNL,percutaneous nephrolithotomy;URS/RIRS,ureteroscopy and retrograde intrarenal surgery;ESWL,extracorporeal shock wave lithotripsy;TURP,transurethral resection of prostate;TURBT,transurethral resection of bladder tumor;BOO,bladder outlet obstruction.
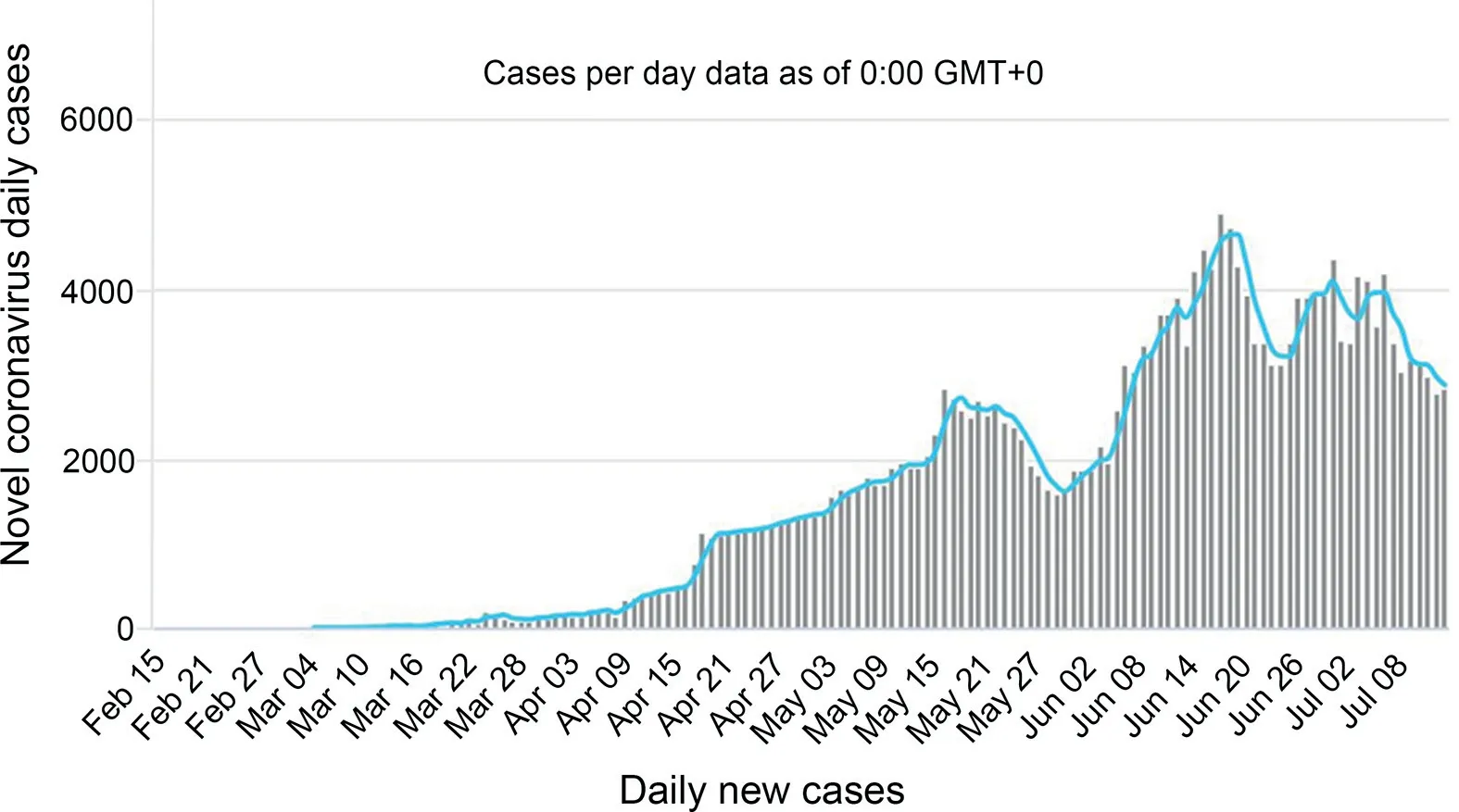
Figure 4 Peak of COVID-19 infection in KSA during May,June and July(Coronavirus update(live).Last updated:July 14,2020,18:39 GMT.https://www.worldometers.info/coronavirus/country/saudi-arabia/)[accessed on 23/06/2020][23].
Regarding BOO,only two TURP procedures were performed in April 2020 compared to 32 procedures in April 2019,with a 93.8% decrease.While we inserted SPC as a temporarily procedure in 10 cases to relieve BOO,then an active treatment will be followed at the earliest possible time.As most urologists,we believe that the elective treatment of benign prostatic hyperplasia(BPH)and urethral stricture diseases have low priority during COVID-19 pandemic and not considered an emergency unless the patient has develop acute urinary retention with inability to pass a urethral catheterize.Recently,Stensland et al.[9]recommended that all prostatic procedures be delayed,and urinary obstruction can be treated via a urethral or suprapubic catheter using local anesthesia.Similarly,Goldman and Haber[8]from Cleveland clinic classified the management of urinary outlet obstruction into tiers(0-4)according to surgical priority.If a patient has a urinary retention and unable to pass catheter,it is considered tier 0(i.e.emergency intervention is needed).While if a patient has BPH on self-catheter or self-voiding,it is considered tier 4(i.e.intervention is not essential)[8].
In our study,there was a slight decrease by a 9.3% in the number of emergency surgical procedures in the first third of 2020 compared to the same period in 2019(p=0.286).This might be explained by the decrease in number of referred patients from other cities due to the full curfew between cities,as well as,our careful selection of the emergency cases based on high priority to intervene.During the curfew period,more than half of the emergency procedures were related to urolithiasis treatment.Generally,our decision to schedule patients for stone surgical intervention was based on several parameters,including stone size and site,renal function parameters,severity of symptoms,duration of obstruction,collecting system drainage(i.e.presence of JJ-stent or stent or NPT),and other related factors(e.g.solitary kidney).The common indications of interventions were ureteral obstruction associated with infection and/or elevated renal function,and calcular anuria.We preferred to choose the least invasive intervention for the treatment of these urgent cases by offering active stones treatment in only 12.5%,and the remaining of cases(87.5%)were treated temporarily by drainage of the collecting system using JJ-stent or NPT insertion.A recent survey discussed the practice patterns of expert endourologists for the treatment of urolithiasis following the COVID-19 pandemic,and 90% of them tended to change their treatment strategy for positive COVID-19 patients by drainage of the collecting system followed by an elective intervention[7].
There are few urology recommendations and triages that have been published recently to help prioritize urological procedures in the time of COVID-19 pandemic.Some endourology procedures are emergent and must be done immediately,and some are urgent,while the remaining of procedures can be delayed for months.These recommendations from experts need to be tailored according to locally available facilities,resources,health care workers,as well as burden of COVID-19 for each institute and city.
The main limitation of our study was its retrospective design.However,several strength points are present.Tothe best of our knowledge,this is the first study that addresses the actual impact of COVID-19 on endourology surgical practice in a country.In addition,it is a multicenter study,with participation of the largest tertiary endourology centers in KSA.Moreover,the sample size was large,and more than 46 000 OPD visits and 5000 surgical procedures were included in our analysis.
5.Conclusions
In summary,during COVID-19 pandemic urology services in KSA tertiary hospitals slashed by more than 75%,including OPD visits and elective endourology surgical procedures.Certain procedures almost were stopped such as PNL,SWL,and TURP.However,there was a mild decrease of 25%in the emergency endourology surgical procedures.To reduce the risk of infection and maintain resources,most hospitals have changed their strategic measures by increasing the rate of telephone clinics by more than 90% and outpatient elective procedures up to 85%.To ensure the maximum benefits to patients,endourologists should consider during their treatment the recent recommendations and triage systems according to surgical priority.
Author contributions
Study design:Abdel Raheem Ali,Yahya Ghazwani,Ibrahim Alowidah,Saeed Bin Hamri.
Data acquisition:Raed A.Azhar,Yahya Ghazwani,Mohammed Alomar,Ahmed Alzahrani,Ossamah Alsowayan,Wissam Kamal,Abdulrahman Alalayet,Ahmad Bugis,Abdulaziz M.Althunayan,M.Alzahrani Tarek,Kamel Fadaak,Aiman Al-Solumany.
Data analysis:Abdel Raheem Ali,Ibrahim Alowidah,Saeed Bin Hamri.
Drafting of manuscript:Abdel Raheem Ali.
Critical revision of the manuscript:Ibrahim Alowidah,Yahya Ghazwani,Saeed Bin Hamri.
Conflicts of interest
The authors declare no conflict of interest.
 Asian Journal of Urology2021年4期
Asian Journal of Urology2021年4期
- Asian Journal of Urology的其它文章
- Radical cystoprostatectomy with orthotopic neobladder for a case of treatment emergent neuroendocrine prostate cancer presenting as bladder mass with hematuria-a rare instance of tumor remission after local control
- Late upper urinary tract urothelial carcinoma following radical cystectomy,presenting as page kidney
- Metachronous chest wall metastasis from clear cell renal cell carcinoma-A rarity
- Perioperative anticoagulation and open distal corpora cavernosa shunt in the management of a case of stuttering idiopathic persistent childhood ischaemic priapism
- Effect of tamsulosin versus tamsulosin plus tadalafil on renal calculus clearance after shock wave lithotripsy:An open-labelled,randomised,prospective study
- A novel spherical-headed fascial dilator is feasible for second-stage ultrasound guided percutaneous nephrolithotomy:A pilot study