Mild moxibustion plus loratadine tablets for children with allergic rhinitis: a randomized controlled trial
2021-12-17 10:52:28LiYong李勇GuoXiaoqing郭曉慶
Li Yong (李勇), Guo Xiao-qing (郭曉慶)
Wuhan Hospital of Traditional Chinese Medicine, Hubei Province, Wuhan 430014, China
Abstract
Keywords: Moxibustion Therapy; Moxa Stick Moxibustion; Loratadine; Rhinitis, Allergic; Randomized Controlled Trials;Child
Allergic rhinitis (AR) is a chronic inflammatory disease of nasal mucosa mainly mediated by immune globulin E(IgE), with nasal obstruction, nasal itching, runny nose and paroxysmal sneezing as typical symptoms[1]. As a common chronic respiratory inflammatory disease in children, the prevalence of AR in domestic children is about 15.8%, and is increasing year by year[2]. AR has recurrent course and is difficult to cure, which seriously affects the quality of life and study in children, and can be accompanied by bronchial asthma, sleep-related breathing disorder and otitis media, bringing heavy psychological and economic burden to children and parents[3].
At present, glucocorticoids and antihistamines are the main drugs in the treatment of AR in Western medicine,and they can produce a rapid effect. It can significantly improve the symptoms of rhinitis, and improve the
quality of life and learning efficiency. However, the adverse reactions are obvious, and the disease is easy to relapse after withdrawal[4]. In recent years, a study has found that traditional Chinese medicine treatment can improve the constitution of patients with AR, enhance their immunity, relieve the clinical symptoms, and has no obvious adverse reactions, thus having good application prospects[5]. In this study, we used mild moxibustion plus loratadine tablets for children with AR, and compared it with loratadine tablets alone.
1 Clinical Materials
1.1 Diagnostic criteria
1.1.1 Diagnostic criteria in Western medicine
The diagnostic criteria for AR in Western medicine referred to theChinese Guidelines for Diagnosis and Treatment of Allergic Rhinitis[6]. At least two symptoms of nasal obstruction, nose itching, runny nose and sneezing, cumulative or lasting for more than 1 h per day;may be accompanied by ocular symptoms such as itchy eyes and conjunctival congestion; swelling and pale nasal mucosa, inferior nasal concha edema, watery nasal secretions; with special signs such as allergic salute,allergic shadows, or allergic folds; skin prick test or serum specific IgE positive.
1.1.2 Criteria for syndrome differentiation in traditional Chinese medicine (TCM)
According to theClinical Guidelines for Diagnosis and Treatment of Pediatric Diseases in Chinese Medicine:Allergic Rhinitis in Children[7], criteria for TCM syndrome differentiation of lung Qi deficiency cold in this study were established. Primary manifestations: nasal obstruction, nose itching, runny nose, and sneezing.Secondary manifestations: fear of wind and cold, easy to catch a cold, spontaneous sweating, low and timid voice,weak and lazy to speak, a pale red tongue with thin white coating, weak pulse.
1.2 Inclusion criteria
Those who met the above diagnostic criteria in Western medicine and the syndrome differentiation criteria in TCM; aged 3-14 years old; children’s legal guardians signed the informed consent; children who could accept mild moxibustion and Western medications,with good compliance; had not received any other treatment, or had stopped other therapy for more than two weeks.
1.3 Exclusion criteria
Those who had obvious deflected nasal septum, or with complications such as bronchial asthma attacks and nasal polyps; who were allergic to loratadine; those with severe primary diseases or congenital diseases.
1.4 Elimination and dropout criteria
Those who had severe adverse reactions or accidents during the trial; with incomplete data records; whose legal guardians asked for withdrawal from the trial; those received other treatment without authorization.
1.5 Statistical methods
All data were statistically analyzed by the SPSS version 22.0 statistical software. Counting data were processed by Chi-square test. Measurement data in normal distribution and having homogeneous variance were expressed as mean ± standard deviation (±s), and analyzed byt-test. If data did not meet the normal distribution or not have homogeneous variance, nonparametric test was applied.P<0.05 was considered to indicate a statistically significant difference.
1.6 General data
A total of 80 children with AR who met the inclusion criteria were enrolled from our hospital, between January 2018 and December 2019. All patients were randomly divided into a control group and an observation group by the random number table method,with 40 cases in each group. During the trial, there was no dropout case in either group. There were no significant differences in gender, age, or duration of disease between the two groups (P>0.05), indicating that the two groups were comparable (Table 1).
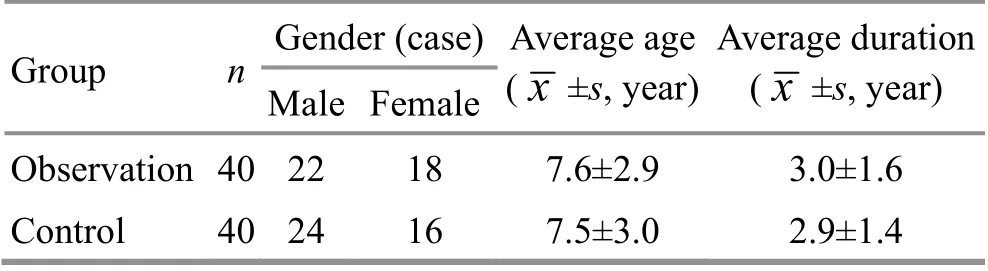
Table 1. Comparison of the general data between the two groups
2 Treatment Methods
2.1 Control group
Children in the control group were treated with oral loratadine tablets [State Food and Drug Administration Approval No. H10970410, Shanghai Schering-Plough Pharmaceutical Co., Ltd., China]. For children over 12 years old, 10 mg/time; for children between 3 and 12 years old, weight >30 kg, 10 mg/time, or weight ≤30 kg,5 mg/time. Once a day, take with warm water every night before going to bed. The treatment continued for two weeks.
2.2 Observation group
Children in the observation group were treated with additional mild moxibustion treatment based on oral loratadine tablets. The usage and dosage of loratadine were the same as in the control group.
Acupoints: Dazhui (GV 14), bilateral Fengmen (BL 12)and Feishu (BL 13).
Methods:Children took a prone position, in a quiet state, with the skin of acupoint area exposed. After lighting the moxa stick, the doctor placed the index finger and middle finger of his left hand around the acupoint,and held the moxa stick in his right hand, aiming at the
selected acupoint. Mild moxibustion was applied 3-5 cm away from the skin, and each point for about 10 min each time till the doctor's fingers became warm and the children's skin flushed[8]. The moxibustion treatment was performed once every other day for two weeks.
3 Observation of Curative Efficacy
3.1 Observation items
3.1.1 Total nasal symptom score (TNSS)
Before and after treatment, the severities of nasal obstruction, nose itching, runny nose and sneezing in both groups were scored. Zero point stands for none,1 point for mild symptoms, 2 points for moderate symptoms, and 3 points for severe symptoms. The TNSS was 0-12 points. The higher the score, the more severe the AR symptoms[9].
3.1.2 Serum eosinophils (EOS) count
Before and after treatment, fasting venous blood was taken from the children, and the serum EOS count was measured by an automatic blood cell analyzer.
3.1.3 Serum interleukin (IL)-27 and macrophage migration inhibitory factor (MIF) level
Before and after treatment, fasting venous blood was collected from the children, and the serum IL-27 and MIF levels were determined by enzyme-linked immunosorbent assay.
3.2 Criteria of curative efficacy
The TNSS reduction rate was used as the criteria for curative efficacy in this study[10]. TNSS reduction rate =(TNSS before treatment - TNSS after treatment) ÷ TNSS before treatment × 100%.
Markedly effective: After treatment, TNSS reduction rate was ≥66%.
Effective: After treatment, TNSS reduction rate was >25%, but <66%.
Invalid: TNSS reduction rate was ≤25%.
3.3 Treatment results
3.3.1 Comparison of the curative efficacy
The total effective rate of the observation group was 95.0%, higher than 77.5% of the control group, and the difference between the two groups was statistically significant (P<0.05), (Table 2).
3.3.2 Comparison of the TNSS
Before treatment, there were no statistical differences in the scores of nasal obstruction, nose itching, runny nose and sneezing and general TNSS between the two groups (P>0.05). After treatment, the scores of nasal obstruction, nose itching, sneezing and general TNSS in the control group decreased (P<0.05), while the score of runny nose had no significant change (P>0.05). In the observation group, the scores of nasal obstruction, nose itching, runny nose and sneezing and general TNSS all decreased (P<0.05), and were all lower than those in the control group (P<0.05), (Table 3).
3.3.3 Comparison of the serum EOS count
Before treatment, there was no statistical difference in the serum EOS count between the two groups (P>0.05).After treatment, the serum EOS count in both groups decreased (P<0.05), and the serum EOS count in the observation group was lower than that in the control group (P<0.05), (Table 4).
3.3.4 Comparison of the serum IL-27 and MIF levels
Before treatment, there were no statistical differences in the serum IL-27 and MIF levels between the two groups (P>0.05). After treatment, the serum IL-27 level in the control group had no statistical difference from that before treatment (P>0.05), and the serum MIF level was lower than that before treatment (P<0.05).Compared with the same group before treatment, the serum IL-27 level in the observation group increased and the serum MIF level decreased (P<0.05), and were statistically different from those in the control group(P<0.05), (Table 5).

Table 2. Comparison of the clinical efficacy between the two groups (case)
Table 3. Comparison of the TNSS between the two groups ( ±s point)

Table 3. Comparison of the TNSS between the two groups ( ±s point)
Note: Compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
Group n Time Nasal obstruction Nasal itching Runny nose Sneezing TNSS Observation 40 Before treatment 2.60±0.50 2.55±0.50 2.32±0.83 2.52±0.50 10.00±0.91 After treatment 1.00±0.751)2) 0.98±1.051)2) 1.03±0.801)2) 1.05±0.811)2) 4.05±1.841)2)Control 40 Before treatment 2.65±0.48 2.50±0.51 2.03±0.77 2.53±0.51 9.70±1.39 After treatment 1.57±1.151) 1.58±1.211) 1.68±1.10 1.37±0.491) 6.20±2.161)
Table 4. Comparison of the serum EOS count between the two groups ( ±s ×109/L)
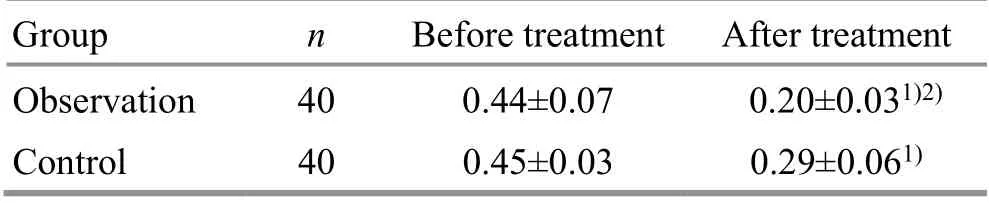
Table 4. Comparison of the serum EOS count between the two groups ( ±s ×109/L)
Note: Compared with the same group before treatment, 1) P<0.05;compared with the control group after treatment, 2) P<0.05
Group n Before treatment After treatment Observation 40 0.44±0.07 0.20±0.031)2)Control 40 0.45±0.03 0.29±0.061)
Table 5. Comparison of the serum IL-27 and MIF levels between the two groups ( ±s
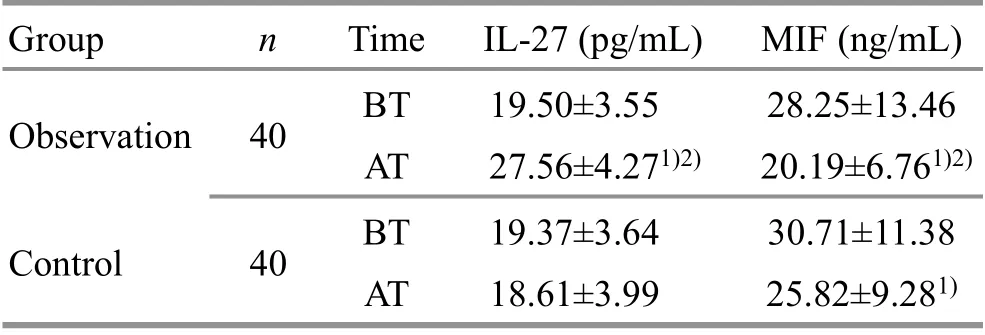
Table 5. Comparison of the serum IL-27 and MIF levels between the two groups ( ±s
Note: BT=Before treatment; AT=After treatment; compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
Group n Time IL-27 (pg/mL) MIF (ng/mL)Observation 40 BT 19.50±3.55 28.25±13.46 AT 27.56±4.271)2) 20.19±6.761)2)Control 40 BT 19.37±3.64 30.71±11.38 AT 18.61±3.99 25.82±9.281)
4 Discussion
Modern medicine believes that the incidence of AR is closely related to heredity, exposure to allergens and environmental factors. AR has a clear tendency of family aggregation. Data show that the prevalence of AR in children with only one parent having a history of AR is about 30.0%. If both parents have a history of AR, the prevalence in their children is as high as about 50.0%[11].Allergens are the direct factors inducing AR. According to the way allergens enter the body, they are mainly divided into inhalation, ingestion, contact, and injection.Allergens entering the human body can stimulate the body to produce specific IgE and cause allergic reactions[12]. In addition, environmental factors such as increasingly serious air pollution and pets also have an important impact on the occurrence and development of AR[13].
When allergens invade the human body for the first time, the specific IgE antibodies are combined with mast cells and basophils in nasal mucosa, making them sensitized. When exposed to the same allergen again,the IgE-mediated allergic inflammatory response is provoked. Mast cells and basophils release histamine,leukotrienes and other inflammatory mediators, which stimulate sensory nerve endings and blood vessels of nasal mucosa, excite the parasympathetic nerves, and cause nasal symptoms such as sneezing, runny nose, and nasal obstruction[14]. After about 4-6 h, EOS differentiates, matures, migrates, chemotaxis, and accumulates to the nasal mucosa, releasing inflammatory mediators, resulting in capillary dilatation,increased permeability and secretion of glands, and releasing toxic proteins, which damage the nasal mucosa,and aggravate inflammation, cause symptoms such as persistent nasal obstruction, nose itching, sneezing and runny nose[15].
IL-27 is a cytokine with a dominant immunemodulatory function. It can promote the differentiation of initial CD4+T cells into helper T cells (Th) 1, secrete interferon, and inhibit them from developing to Th2 and Th17. It plays an important role in maintaining the dynamic balance of Th1/Th2 and Th17/Treg in the immune system[16]. The pathogenesis of AR is related to the immune imbalance of Th1/Th2 and Th17/Treg, which is characterized by the dominance of Th2 and the inhibition of Th1, the dominance of Th17 and the dysfunction of Treg[17-18]. Cytokines such as IL-4 and IL-6 secreted by Th2 cells stimulate the proliferation and differentiation of B cells, and promote the synthesis of IgE antibodies[17]. Th17 cells secrete IL-17 and participate in airway allergic reactions[18]. Yang FW,et al[19]detected the expression of IL-27 and IL-17 in the serum of AR patients and healthy participants. The results showed that the serum IL-27 level in AR patients was lower than that in the healthy participants, the serum IL-17 level was higher than that in the healthy participants, and the serum IL-27 level of AR patients was negatively correlated with IL-17. This result suggested that IL-27 had an immunomodulatory effect on IL-17. It can be seen that regulating the IL-17 level and promoting the rebalance of the Th1/Th2 and Th17/Treg is the possible direction for the treatment of AR.
MIF is an important mediator in the process of inflammatory immune response. It can inhibit macrophage migration, promote monocyte adhesion and vascular inflammatory response, and exist in EOS at inflammatory sites[20]. A study has shown that the serum MIF level of AR patients is significantly higher than that of healthy participants, and the MIF level is closely related to the severity of AR[21]. Ma HJ[22]found that the serum MIF level of patients with nasal polyps was positively correlated with the degree of EOS infiltration in nasal polyps. It can be seen that down-regulating the level of MIF can inhibit the inflammatory response,reduce EOS infiltration, and relieve the symptoms of AR.
Loratadine is a classic second-generation antihistamine. It can directly block the binding of histamine to H1receptors and has anti-inflammatory effects. It is the first-line drug for the treatment of AR. It has definite curative effect, and can reduce allergic symptoms such as nasal itching, sneezing and runny nose. It acts faster than glucocorticoid, and has relatively high compliance and safety rating[23].
AR belongs to Bi Qiu (AR) in TCM. The internal cause of the disease is the deficiency of the lung, spleen and kidney, and the external cause is nasal orifices invaded by the six climatic exogenous pathogens and pathogenic Qi. The lung is delicate and opens into the nose. If the lung Qi is deficient, the Wei-Defensive Qi will be weak.The exogenous pathogen invades the lung through the nose, and the lung loses its function in governing diffusion and purification and descending, resulting in symptoms such as nasal obstruction and runny nose. The insufficiency of lung Qi and generation of deficient cold,plus the invasion of cold pathogen cause runny nose[24].It can be seen that syndrome of lung Qi deficiency cold is the common syndrome of Bi Qiu (AR), which is usually caused by deficient cold constitution and invasion of exogenous pathogens. Treatment should be based on the principles of warming the lungs and dispelling cold,replenishing Qi and solidifying the exterior[25].
Mild moxibustion has the effects of warming yang for dispelling cold, and strengthening body resistance and benefiting Qi. It is moderately warm and comfortable,and suitable for AR children. Dazhui (GV 14) is a key point of the Governor Vessel, with significant effects of dispelling pathogenic wind for relieving superficies,dispelling cold and warming Yang, which can clear the nasal orifices, and treat exogenous diseases. Fengmen(BL 12), the crossing point of the Bladder Meridian and Governor Vessel mainly for the wind diseases, has the effects of relieving exogenous pathogenic factors and facilitating the lung, and invigorating Qi for consolidating the exterior. Feishu (BL 13) is the Back-Shu point of lung,a key point for lung diseases. It can relieve superficies and facilitate the lung, regulate and invigorate lung Qi.The combination of the above acupoints, with the application of mild moxibustion, has the effects of benefiting Qi and warming Yang, relieving superficies and dispelling cold, and clearing nasal orifices.
Results in this study showed that the total effective rate of the observation group was higher than that of the control group. After treatment, the general TNSS in both groups decreased, and the general TNSS in the observation group was lower than that in the control group. Compared with those before treatment, the serum EOS count in both groups decreased, and the serum EOS count in the observation group was lower than that in the control group. It suggested that mild moxibustion plus loratadine tablets was effective in treating AR in children, which could significantly improve the nasal symptoms and reduce the serum EOS count.After treatment, the serum IL-27 in the control group had no obvious change, and the serum MIF level decreased.In the observation group, the serum IL-27 level increased and the serum MIF level decreased, which were statistically different from those in the control group. It suggested that the combination of mild moxibustion and loratadine tablets could regulate the serum IL-27 and MIF levels in children with AR.
In summary, mild moxibustion plus loratadine tablets is effective in the treatment of AR in children. It can significantly improve the nasal symptoms and reduce the serum EOS count, which may be related to the regulation of serum IL-27 and MIF levels in children with AR.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Acknowledgments
There was no project fund supporting this study.
Statement of Informed Consent
Informed consent was obtained from the guardians of the recruited children in this study.Received: 14 September 2020/Accepted: 25 December 2020
 Journal of Acupuncture and Tuina Science2021年6期
Journal of Acupuncture and Tuina Science2021年6期
- Journal of Acupuncture and Tuina Science的其它文章
- Effects of sinew-regulating bone-setting manipulations on chondrocytes, IL-1β and NO in rabbits with knee osteoarthritis
- Efficacy observation of auricular point sticking in combination with a healthy diet for simple obesity in children
- Clinical efficacy of sticking-needle acupuncture plus tendon-regulating manipulation in the treatment of acute ankle sprain
- Therapeutic efficacy observation of warm needling moxibustion plus spine subtle adjusting manipulation for cervical radiculopathy
- Evaluation of the clinical efficacy of muscle regions of meridians needling method for refractory facial paralysis based on infrared thermal imaging technology
- Clinical study on Tuina plus umbilical therapy for senile functional constipation