Evaluation of the clinical efficacy of muscle regions of meridians needling method for refractory facial paralysis based on infrared thermal imaging technology
2021-12-17 10:52:32MaoTingli毛廷麗WangZhuxing王竹行TianFengwei田豐瑋ZhouXi周熙
關鍵詞:科技
Mao Ting-li (毛廷麗), Wang Zhu-xing (王竹行), Tian Feng-wei (田豐瑋), Zhou Xi (周熙)
1 Chongqing University Central Hospital/The Fourth People’s Hospital of Chongqing, Chongqing 400014, China
2 Chongqing Traditional Chinese Medicine Hospital, Chongqing 400021, China
Abstract
Keywords: Acupuncture Therapy; Musculature of 12 Meridians; Needling Methods; Facial Paralysis; Infrared Rays;Thermography
Peripheral facial paralysis belongs to the category of peripheral facial neuritis or facial nerve palsy in modern medicine. Most patients with facial paralysis recover well through systemic treatment, and some even recover without treatment[1]. However, some patients remain uncured and develop into refractory facial paralysis over a long time. The difference in facial nerve injury segments is directly related to the course and curative effect of acupuncture for facial paralysis[2], thereby affecting the prognosis of facial paralysis.
In this study, we observed the curative effect of muscle regions of meridians needling method for refractory facial paralysis, and explored the correlation between the efficacy and disease location. By observing the rules of infrared thermal imaging, we explored the practicability of estimating the location of facial paralysis and evaluating the treatment effect based on thermal imaging.
1 Clinical Materials
1.1 Diagnostic criteria
1.1.1 Diagnostic criteria in Western medicine
This study referred to the diagnostic criteria of idiopathic facial palsy in theNeurology[3].
1.1.2 Diagnostic criteria in traditional Chinese medicine (TCM)
This study referred to the diagnostic criteria of facial paralysis in theScience of Acupuncture and Moxibustion[4].
1.1.3 Anatomical diagnosis of facial nerve injury
The facial nerve injury was located according to the symptoms and manifestations.
At stylomastoid foramen or below (distal end of chorda tympani branching): The facial expression muscles on the affected side were paralyzed.
At chorda tympani: The facial muscles on the affected side were paralyzed, with taste changes in the front 2/3 of the tongue and salivary gland secretion dysfunction.
At stapedial branch: The facial muscles on the affected side were paralyzed, with taste changes in the front 2/3 of the tongue, salivary gland secretion dysfunction, and hearing loss.
At geniculate ganglion: The facial muscles on the affected side were paralyzed, with taste changes in the front 2/3 of the tongue, hearing loss, abnormal lacrimal gland secretion, dizziness and headache.
1.2 Inclusion criteria
Those who met the diagnostic criteria for peripheral facial palsy in Western medicine and TCM; with disease duration ≥2 months but ≤1 year; the House-Brackmann(H-B) grading was Ⅲ-Ⅵ levels; aged over 18 years old;those had other diseases that would not affect the treatment of this disease during the treatment period;with clear consciousness and in good general condition,and was able to cooperate with examination and treatment; agreed to participate in this trial and signed informed consent.
1.3 Exclusion criteria
Patient with facial paralysis due to otogenic diseases,acoustic neuroma, parotitis, Guillain-Barre syndrome,retromandibular purulent lymphadenitis, neuro-Lyme disease, cerebellopontine angle arachnoiditis, posterior fossa tumor, or meningitis; combined with severe primary diseases of heart, liver, kidney, or hemopoietic system; psychotics; pregnant women; those who were intolerant to acupuncture treatment.
1.4 Elimination and dropout criteria
Those with poor compliance and unable to receive the acupuncture treatment on time; dropped out due to changes in the disease condition, economic reasons, or other factors; those who did not receive the treatment as protocol, making it unable to evaluate the efficacy, or those who had incomplete data that affected the efficacy or safety evaluation.
1.5 Statistical methods
All the data were statistically analyzed by the SPSS version 20.0 statistical software. The counting data were processed by Chi-square test. The measurement data were expressed as mean ± standard deviation (±s),and analyzed by thet-test. Rank-sum test was applied to the comparison of the ranked data. In two-side tests,P<0.05 was considered to indicate a statistically significant difference.
1.6 General data
A total of 110 patients with refractory facial paralysis were enrolled from the Acupuncture Department of Chongqing Traditional Chinese Medicine Hospital between January 2017 and December 2018. The simple randomization grouping method was applied using SAS software package to generate a random allocation table on the computer. The patients were randomly divided into an observation group and a control group according to the enrolling sequence, with 55 cases in each group.During the trial, there were three dropout cases in the observation group, and four in the control group. Thus, a total of 103 cases completed this trial. There were no significant differences in gender, age, or duration of disease between the two groups (P>0.05), indicating that the two groups were comparable (Table 1).
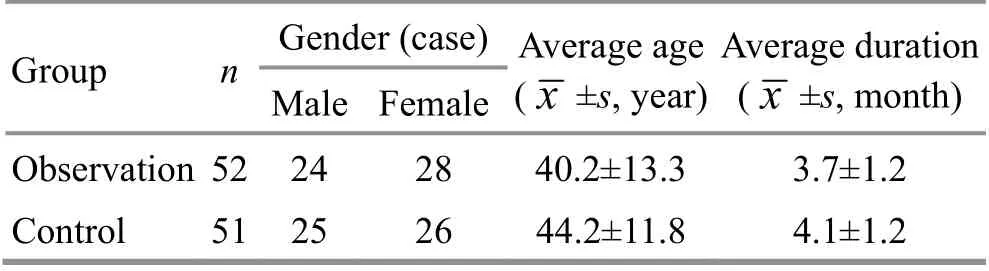
Table 1. Comparison of the general data between the two groups
2 Treatment Methods
Both groups received corresponding treatments for basic diseases such as coronary heart disease,hypertension, and diabetes. All acupuncture operations were performed by professional acupuncturists.
2.1 Observation group
Patients in the observation group were treated with muscle regions of meridians needling method summarized by Professor Shi Xue-min[5].
Major acupoints: Muscle regions of Yangming meridians between Yangbai (GB 14), Dicang (ST 4) and Jiache (ST 6); Taiyang (EX-HN 5), Quanliao (SI 18), and Dicang (ST 4).
Adjunct acupoints according to syndrome differentiation: Patients with a bitter taste in the mouth and tinnitus belonged to the syndrome of liver fire exuberance, and were treated with additional Waiguan(TE 5), Shuaigu (GB 8) and Xingjian (LR 2) with twirling reducing manipulation. Patients suffering from longterm disease or with a weak constitution were treated with additional bilateral Zusanli (ST 36) with twirling reinforcing manipulation. Those presenting with facial spasm were treated with additional Taiyang (EX-HN 5)and Quanliao (SI 18) on the healthy side, and bloodletting puncture and cupping therapy.
Methods:After routine disinfection, the four-point penetrating needling method was applied to Yangbai(GB 14), that was, four needles at one acupoint. It was punctured with the needle tip and the skin forming a 15°angle, towards Shangxing (GV 23), Touwei (ST 8),Cuanzhu (BL 2), and Sizhukong (TE 23), respectively.Aligned needling method was applied to the muscle regions of Yangming meridians between Dicang (ST 4)and Jiache (ST 6), that was, the aligned needling method was performed with multi-needle and superficial needling along the route of muscle regions of Yangming meridians between the two acupoints, with one needle at every 0.5 Cun. Taiyang (EX-HN 5) was punctured toward Dicang (ST 4) through Quanliao (SI 18), with 2.5-3.0 Cun in depth. The two-point penetrating method was applied to Sibai (ST 2), with two needles at one acupoint.It was punctured with the needle tip and the skin forming a 15° angle, toward the inner canthus and outer canthus,respectively. Twirling reducing manipulation was performed and the needles were retained for 30 min.
2.2 Control group
According to the treatment protocol for facial paralysis disease (facial neuritis) in theDiagnosis and Treatment Protocols of Traditional Chinese Medicine for 22 Professionals and 95 Diseases[6], the control group was treated with point selection along meridians plus facial three-line needling method.
Acupoint selection along meridians: Baihui (GV 20),Fengfu (GV 16), Fengchi (GB 20), Taichong (LR 3), Hegu(LI 4), Shenting (GV 24), Taiyang (EX-HN 5), Xiaguan (ST 7),Yifeng (TE 17), Zusanli (ST 36), and Neiting (ST 44).
Facial three-line needling method: The line from Shenting (GV 24), Yintang (EX-HN 3), Shuigou (GV 26) to Chengjiang (CV 24) is on the midline of the human face and thus is called the midline; from Yangbai (GB 14),Yuyao (EX-HN 4), Chengqi (ST 1), Sibai (ST 2), Juliao (ST 3)to Dicang (ST 4) is another line, called the lateral line;from Taiyang (EX-HN 5), Xiaguan (ST 7) to Jiache (ST 6) is the third line, called the side line.
Adjunct acupoints according to syndrome differentiation: The same as those in the observation group.
Methods:After routine disinfection, the needles were punctured by 0.5-1.5 Cun in depth. Even reinforcingreducing manipulation and intermittent rapid minor twisting manipulation were applied. The needle was twisted for 2 min at 200 times/min, and was retained for 8 min. The above manipulations were repeated three times for a total of 30 min.
Patients in both groups were treated once a day, and rested for one day after six consecutive treatments. The efficacy was evaluated after four weeks.
3 Observation of Curative Efficacy
3.1 Infrared imaging detection
M301B medical infrared thermal imager [Associated Technology (Chongqing) Corp., China] was placed in a shielded room. The basic value of temperature was 35.0 ℃. The room temperature was controlled at 25-27 ℃. The participant should not receive any facial operation 8 h before the measurement. After entering the shielded room, the participant would rest for 5 min,with the cheeks and neck fully exposed. The far-infrared thermal images of the left and right sides of the face and around the ears were collected before and after treatment. The infrared thermal images were output via computer, and the following items were observed.
Color scale of the affected side: Different color scales represent different temperatures. White is the ultra-high temperature zone; yellow in red or red is the high temperature zone; red in yellow or yellow is the warm zone; yellow in green or green is the cool zone; green in blue or blue is the low temperature zone; blue in purple or purple is the ultra-low temperature zone. Under the same temperature window and temperature width, the changes of skin color scale on the affected side of the two groups were observed before and after treatment.
The temperature differences between the healthy side and affected side of the face and around the ears on the infrared thermal images were observed, and the average temperature difference on both sides was recorded and the corresponding temperature difference was calculated (△t = Skin temperature on the healthy side of the face - Skin temperature on the affected side of the face). The changes of △t before and after treatment in the two groups were observed.
3.2 Criteria for curative efficacy
According to the criteria in the facial nerve grading system[7]combined with theClinical Diagnostic Basis and Criteria for Cure and Improvement of Disease[8], the criteria for curative efficacy in this study were established.
Cured: H-B grading was level Ⅰ.
Markedly effective: H-B grading was improved by 2 levels or more.
Effective: H-B grading was improved by 1 level.
Invalid: H-B grading was improved by less than 1 level.
3.3 Treatment results
3.3.1 Comparison of the clinical efficacy
After treatment, the total effective rate of the observation group was 92.3% and that of the control group was 70.6%. The difference between the two groups was statistically significant (P<0.05), indicating that the clinical efficacy of the observation group was superior to the control group (Table 2).among the four-disease locations was statistically significant (P<0.05). The between-group difference in the efficacy for facial paralysis located at geniculate ganglion was statistically significant (P<0.05). The between-group differences in the efficacy of the rest disease locations were not statistically significant (P>0.05), indicating that the curative effect for the severe cases in the observation group was better than that in the control group (Table 3).

Table 2. Comparison of the clinical efficacy between the two groups (case)
3.3.2 Relationship between the disease locations and efficacy
There was no statistical difference in the distribution of disease location between the two groups before treatment (P>0.05). After treatment, there was no statistical difference in the curative effect among the four-disease locations in the observation group (P>0.05).In the control group, the difference in the curative effect
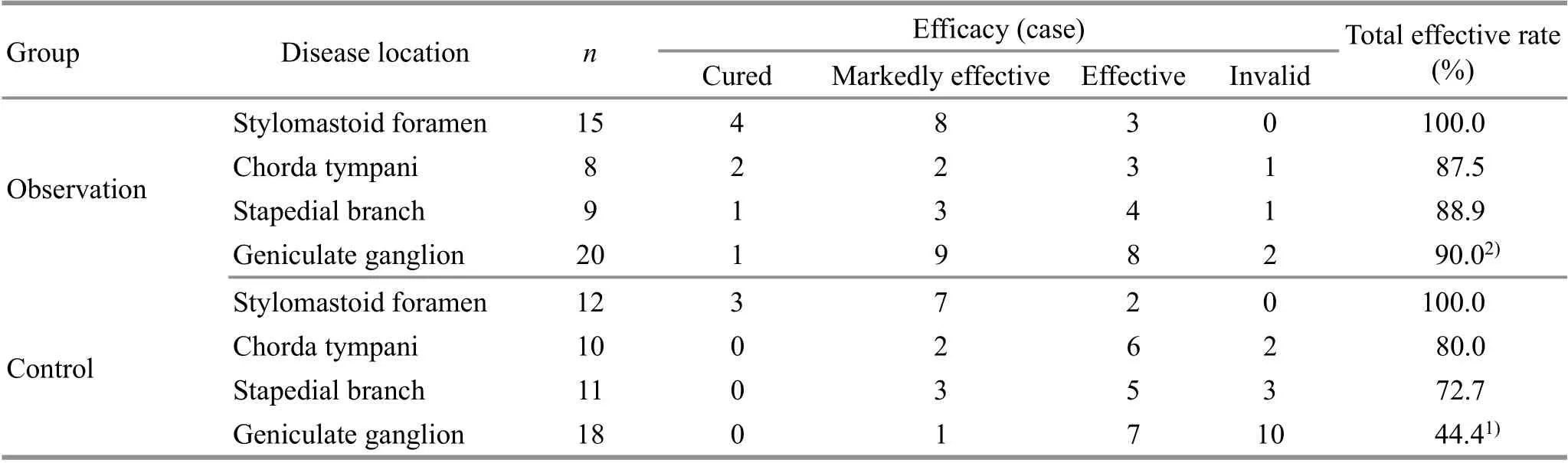
Table 3. Relationship between the disease locations and efficacy in the two groups
3.3.3 Color scale comparison of the infrared thermal imaging
Before treatment, there were no high temperature,ultra-high temperature, or ultra-low temperature zones in the infrared thermography images of the two groups.The changes of color scale were mainly concentrated in the warm, cool, and low temperature zones. There was no significant difference in the proportion of each temperature zone of color scale between the two groups(P>0.05). After treatment, the numbers of warm zones of the affected facial side in the two groups were significantly increased, and the intra-group differences were statistically significant (P<0.01). The proportion of warm zone in the observation group after treatment was significantly higher than that in the control group(P<0.01), (Figure 1 and Table 4).
3.3.4 Comparison of the temperature difference between the healthy side and affected side
Before treatment, the facial and periotic temperature differences between the healthy side and affected side in both groups were not statistically significant (P>0.05).After treatment, the temperature differences between the healthy-affected facial sides and periotic areas in both groups were reduced, and the intra-group differences were statistically significant (P<0.01,P<0.05).The temperature differences between the healthyaffected facial sides and periotic areas in the observation group were lower than those in the control group, and the differences between the two groups were statistically significant (P<0.05), (Table 5).
3.3.5 Relationship between the disease locations and color scale
Before treatment, the color scale distributions between the four-disease locations in the two groups were significantly different, and the intra-group differences were statistically significant (P<0.05). In terms of the proportion of the cold and low temperature zones, patients with the disease location in the geniculate ganglion accounted for the highest, followed by disease location at the facial chorda tympani and stapedial branch, and disease location below the stylomastoid foramen accounted for the lowest (Table 6).
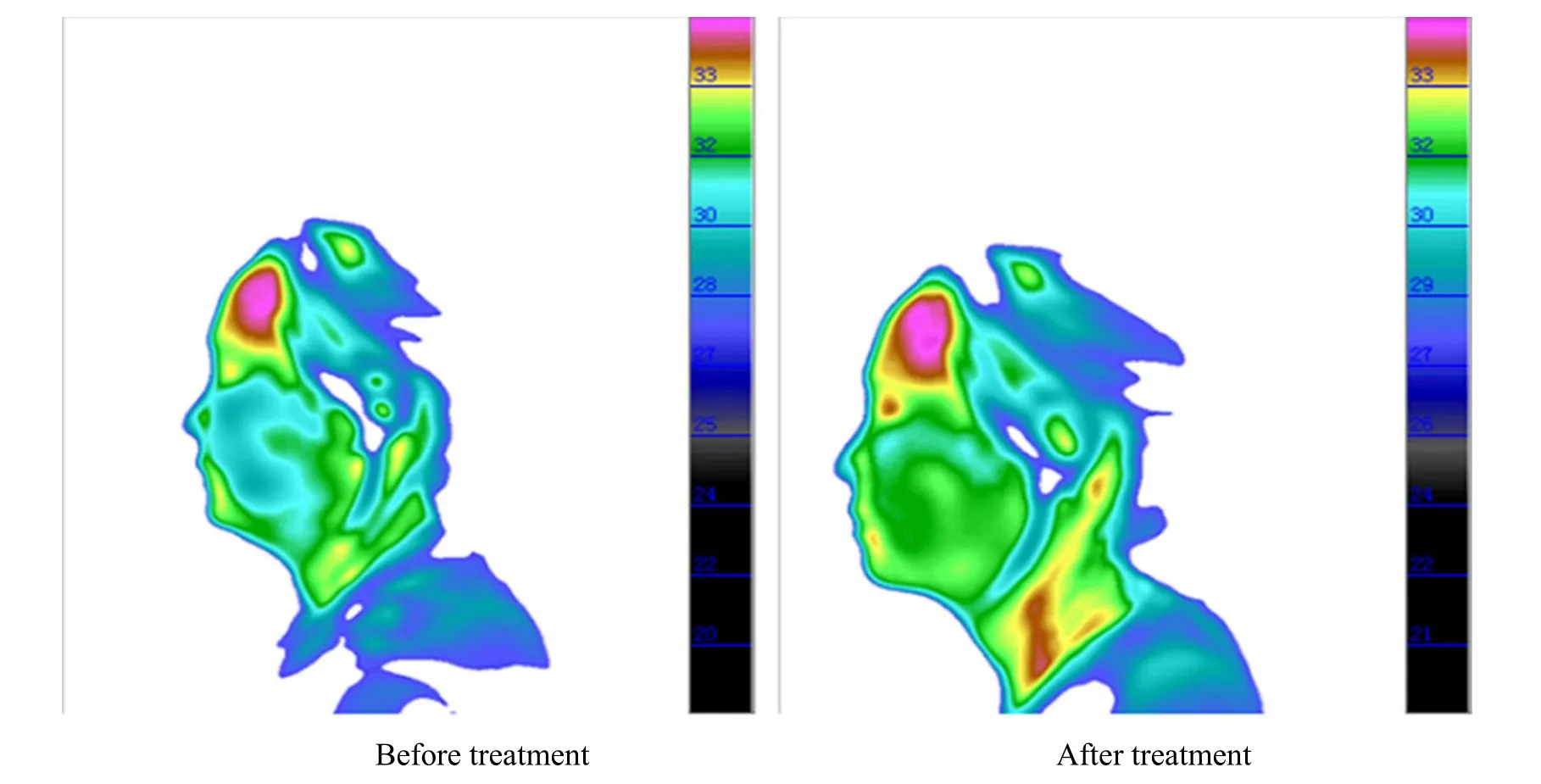
Figure 1. Infrared thermal images of the affected side before and after treatment

Table 4. Comparison of the color scales of the affected side between the two groups
Table 5. Comparison of the temperature differences between the two groups between the health-affected facial sides and periotic areas ( ±s ℃)

Table 5. Comparison of the temperature differences between the two groups between the health-affected facial sides and periotic areas ( ±s ℃)
Note: Compared with the same group before treatment, 1) P<0.01, 2) P<0.05; compared with the control group after treatment, 3) P<0.05
Group n Facial Periotic Before treatment After treatment Before treatment After treatment Observation 52 0.28±0.12 0.11±0.131)3) 0.48±0.35 0.16±0.111)3)Control 51 0.23±0.18 0.16±0.112) 0.54±0.37 0.21±0.142)
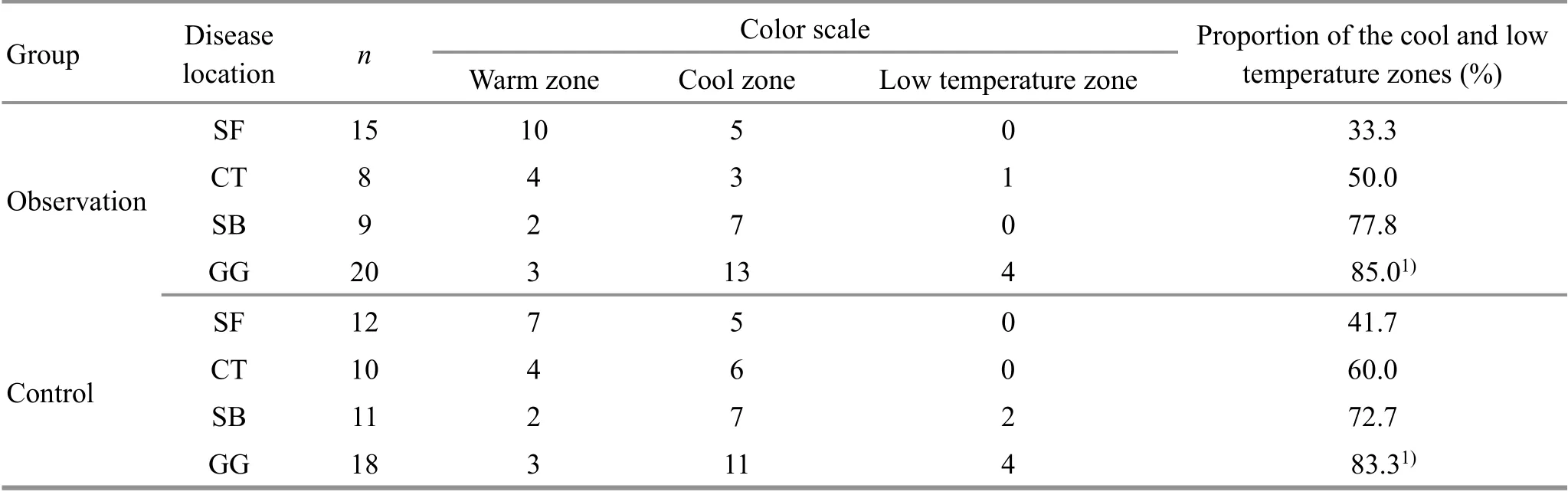
Table 6. Comparison of the relationship between the disease locations and color scale distributions
4 Discussion
The extracranial segment of facial nerve is divided into temporal branch, zygomatic branch, buccal branch,marginal mandibular branch, and cervical branch. Its distribution is basically consistent with the aggregation and distribution of the muscle regions of the three Yang meridians of hand and foot on the face, indicating that facial paralysis is a meridian disease. Professor Shi Xue-min believes that muscle regions of foot Taiyang,hand Yangming and foot Yangming meridians are mainly distributed on the head and face. The muscle regions of meridians go along the superficial tendons, muscles, and joints, easily getting invaded by exogenous pathogens.When the healthy Qi of the human body is insufficient and the Wei-Defensive Qi is weak, the exogenous pathogens will take advantage of the deficiency to enter the collaterals. Thus, the meridian Qi fails to distribute normally and the Qi and blood are blocked, resulting in malnourished meridians, flabby tendons and muscles,and subsequent facial paralysis[9]. Facial paralysis that does not heal over time will become refractory. The main pathogenesis lies in the deficiency of healthy Qi, longtime insufficient production of Qi and blood, or the deeply invaded pathogenic Qi blocking the body fluids,causing malnutrition in the muscle regions of meridians on the face for a long time and resulting in flab and apraxia. At this time, the treatment should be replenishing Qi and blood in the meridians and collaterals, and nourishing and relaxing the tendons.Acupuncture for the paralyzed facial muscles should mainly focus on the muscle regions of meridians penetrating needling and aligned needling[10].
Results in this study showed that compared with conventional acupuncture therapy, muscle regions of meridians needling method had a higher total effective rate in the treatment of refractory facial paralysis.Analyzed from the meridian theory aspect, Yangbai(GB 14) is the crossing point of the Gallbladder Meridian and Yang Link Vessel, and is the key point of the muscle regions of three Yang meridians of hand and foot coursing on the forehead. The four-point penetrating needling method applied to Yangbai (GB 14) can strengthen the meridian Qi of its own, and meanwhile activate meridian Qi of other meridians, to expulse pathogens out. Study has shown that four-point penetrating needling method applied to Yangbai (GB 14)can extensively stimulate the distribution area of the temporal branch of the facial nerve and significantly improve the frontal muscle strength of the patients with peripheral facial paralysis[11]. Aligned needling method was applied to the muscle regions of Yangming meridians between Dicang (ST 4) and Jiache (ST 6), and aligned needling and penetrating needling method were applied to Taiyang (EX-HN 5) and Quanliao (SI 18) toward Dicang (ST 4). The acupuncture positions are basically the same as the accumulation and distribution of the muscle regions of Yangming and Taiyang meridians,bearing the effect of regulating Qi and blood circulation,and unblocking muscle regions of meridians. From the perspective of Western medical anatomy, Yangbai (GB 14)is located in the frontal muscle and innervated by the temporal branch of the facial nerve; Dicang (ST 4) is located in the orbicularis oris muscle and Jiache (ST 6) is located in the masseter muscle, which are respectively innervated by the buccal branch and marginal mandibular branch of the facial nerve; Taiyang (EX-HN 5)is located in the temporal muscle and is innervated by the temporal branch and zygomatic branch of the facial nerve; Quanliao (SI 18) is located in the zygomatic and temporal muscles and innervated by the zygomatic branch of the facial nerve. The above-mentioned acupoints are located at important branches of the extracranial segment of the facial nerve. So, it is speculated that compared with conventional acupuncture, local muscle regions of meridians penetrating needling and aligned needling can stimulate the facial nerve distribution areas to a greater extent,promote the contraction of facial muscle fibers, and improve nerve nutrition, to better promote the recovery of facial nerve function in patients with refractory facial paralysis[5].
The specific cause of refractory facial paralysis is not yet clear. Some research has summarized that improper or failed treatment, long course of disease, high disease location, severe nerve injury, and weak constitution of the patients are the main factors causing refractory facial paralysis[12]. The recovery time of facial paralysis is closely related to the injury level of facial nerve. At present, It is generally believed that the higher the injured facial nerve segment and the degree of axonal degeneration, the more serious the disease and the more the accompanying symptoms, making it harder to get a cure[13]. Some researchers believe that most of the lesions below the stylomastoid foramen are milder and have a high clinical cure rate[14-15]; those lesions in the stapedial muscle or chorda tympani are mainly mild-tomoderate, which is the moderate type; and lesions at the geniculate ganglionitis and above are mostly severe type,with a long treatment time and poor prognosis. In addition, the more serious the injury of facial nerve, the easier it is to form intractable facial paralysis. Gao HW[16]has found that the prognosis of facial paralysis is directly determined by the degree of facial nerve injury, and the prognosis of facial nerve neurite or nerve trunk rupture is far worse than that of facial nerve temporary conduction obstruction. Therefore, among the three common types of peripheral facial paralysis, simple facial paralysis with external facial nerve injury has the best treatment result with acupuncture, Bell's facial paralysis runs the second, and Hunt's facial paralysis is the worst[17]. Results in this study showed that although the two groups of patients with lesions located at the stylomastoid foramen, chorda tympani and stapedial branch had the similar curative effect, it could also be seen that with the rise of the injury location, the effective rate of the conventional acupuncture method gradually decreased; and when the disease location was above the geniculate ganglion, the therapeutic advantage of muscle regions of meridians needling method was more obvious.
At present, there is no uniform standard for the diagnosis of refractory facial paralysis in the medical field.Most of the existing studies have defined the course of disease of more than two or three months as the main standard[18-20]. In the early stage of facial paralysis,excessive spontaneous discharges of facial expression muscles are gradually formed after facial nerve injury,which causes a circumscribed slowdown of the blood flow of the face and affects the blood supply to the nerve tissue[21], thereby reducing the function of the facial nerve. Meanwhile, the secretion of sweat glands is inhibited, resulting in the decrease of local skin heat dissipation function, and the scattering of heat on the skin surface is reduced, forming a temperature difference with the adjacent parts[22]. The more severe the facial nerve injury, the more obvious the temperature difference. And with the recovery of facial nerve injury, the temperature difference will gradually reduce[23]. Therefore, in this study, we tried to use the change of temperature difference as a judgmental basis to measure the severity of facial paralysis and guide the treatment. The medical infrared thermal imaging technology can directly receive the thermal energy radiation emitted by the human body. With computer processing, it reacts to a two-dimensional temperature map, which is used to compare the temperature difference of the observed objects before and after the intervention[24-27]. When the facial nerve is damaged, its innervated muscles become dysfunctional and the capillary network and nerves in the lower layer of the dermal skin tissue are damaged, resulting in low blood supply or ischemia and lead to microcirculation disorders[28-29]. Finally, the facial surface temperature decreases. Acupuncture can promote facial nerve regeneration by improving the local blood circulation[30].In this study, we used an infrared thermal imager to capture the color scale changes of the affected side, and observed that patients with the disease position in the geniculate ganglion had the highest proportions of cool and low temperature zones, followed by the disease locations at the chorda tympani and stapedial branch,and disease location below the stylomastoid foramen accounted for the lowest proportion. After treatment,the blood circulation of local tissues gradually became abundant, the blood flow increased, and the local temperature increased, presenting as a high temperature in the infrared thermal image. However, the unrecovered tissues presented as low temperature because the blood supply was still in a depressed state.Therefore, the change of color scale can also be used as an evaluation indicator for the prognosis of facial paralysis. Results in this study showed that the proportion of warm zone in the observation group after treatment was significantly higher than that in the control group, indicating that the muscle regions of meridians needling method could significantly increase the infrared temperature of the affected side of the face.Meanwhile, using the symmetrical balance of the left and right facial temperature of a normal human body, we found that the temperature differences between the healthy and affected sides of the face and periotic areas after the treatment of muscle regions of meridians needling method were significantly lower than those after conventional acupuncture.
In this study, muscle regions of meridians needling method was applied for refractory facial paralysis, and the results showed that both the muscle regions of meridians needling method and conventional needling method were effective in the treatment of refractory facial paralysis, but the former had more significant efficacy, especially for those with higher injured segments of the facial nerve (above the geniculate ganglion). Besides, the results also showed that the muscle regions of meridians needling method could promote the facial microcirculation of the affected side,improve the blood and oxygen supply to local tissues,and thus promote the repair of the peripheral facial nerve. The incidence of low temperature zone in the infrared thermal images of patients with refractory facial paralysis was correlated with the disease location, that is,the higher the disease location, the higher the incidence of cool and low temperature zones. The color scale distribution in the infrared thermal images of different disease locations had certain specificity, suggesting that infrared thermal imaging can be used as an auxiliary detection method for clinical diagnosis of facial paralysis location and the condition of the disease.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Acknowledgments
This work was supported by the Special Program of Chongqing Social Undertakings and Livelihood Security Science and Technology Innovation Project (重慶市社會民生科技創新專項, No. cstc2016shmszd10001).
Statement of Informed Consent
Informed consent was obtained from all individual participants.
Received: 14 September 2020/Accepted: 25 December 2020
猜你喜歡
中國化妝品(2022年4期)2022-09-15 11:59:04
科技智囊(2022年4期)2022-04-28 19:00:58
科技智囊(2022年4期)2022-04-28 19:00:58
中國核電(2021年3期)2021-08-13 08:57:04
學苑創造·B版(2021年2期)2021-03-15 05:50:49
科學中國人(2018年8期)2018-07-23 02:26:34
少兒科學周刊·兒童版(2017年9期)2018-03-15 15:00:11
兒童故事畫報·發現號趣味百科(2017年4期)2017-06-30 12:41:53
兒童故事畫報·發現號趣味百科(2016年6期)2016-08-19 06:35:19
兒童故事畫報·發現號趣味百科(2015年10期)2016-01-20 00:47:36
 Journal of Acupuncture and Tuina Science2021年6期
Journal of Acupuncture and Tuina Science2021年6期
- Journal of Acupuncture and Tuina Science的其它文章
- Effects of sinew-regulating bone-setting manipulations on chondrocytes, IL-1β and NO in rabbits with knee osteoarthritis
- Efficacy observation of auricular point sticking in combination with a healthy diet for simple obesity in children
- Clinical efficacy of sticking-needle acupuncture plus tendon-regulating manipulation in the treatment of acute ankle sprain
- Therapeutic efficacy observation of warm needling moxibustion plus spine subtle adjusting manipulation for cervical radiculopathy
- Clinical study on Tuina plus umbilical therapy for senile functional constipation
- Effect of acupuncture on serum PYY and nesfatin-1 in obese patients with insulin resistance